
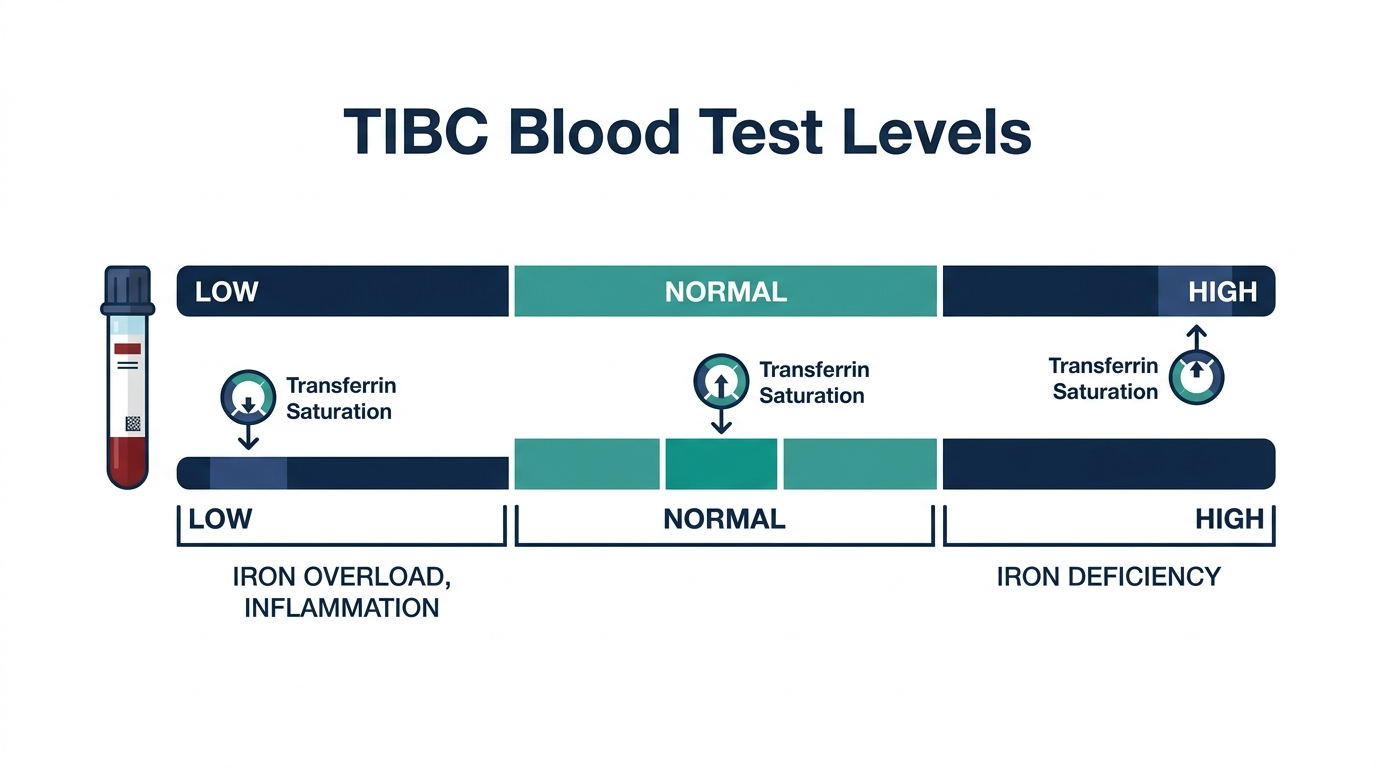
- A low total iron-binding capacity (TIBC) usually means your body has too much iron or chronic inflammation is suppressing transferrin, the protein TIBC measures, and the normal TIBC range is roughly 240 to 450 mcg/dL (Cleveland Clinic).
- Low TIBC paired with high blood iron and a transferrin saturation above 45 percent points toward iron overload such as hereditary hemochromatosis, while low TIBC with low iron points toward chronic disease, infection, liver disease, or malnutrition (StatPearls, NIH).
- Low TIBC is a clue, not a diagnosis, so the result must be read together with serum iron, ferritin, and transferrin saturation, and you should review the full iron panel with your clinician.
Part of our Iron Studies guide.
What a low TIBC result means and the cutoff
A low TIBC means there is less transferrin available to carry iron, which most often happens because iron stores are already high or because chronic inflammation has lowered transferrin production. The normal TIBC range is generally 240 to 450 mcg/dL, so a value below about 240 mcg/dL is flagged low, though exact cutoffs vary by lab (Cleveland Clinic; StatPearls, NIH).
Low TIBC often ties back to iron and inflammation. See both sides of that picture at once. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
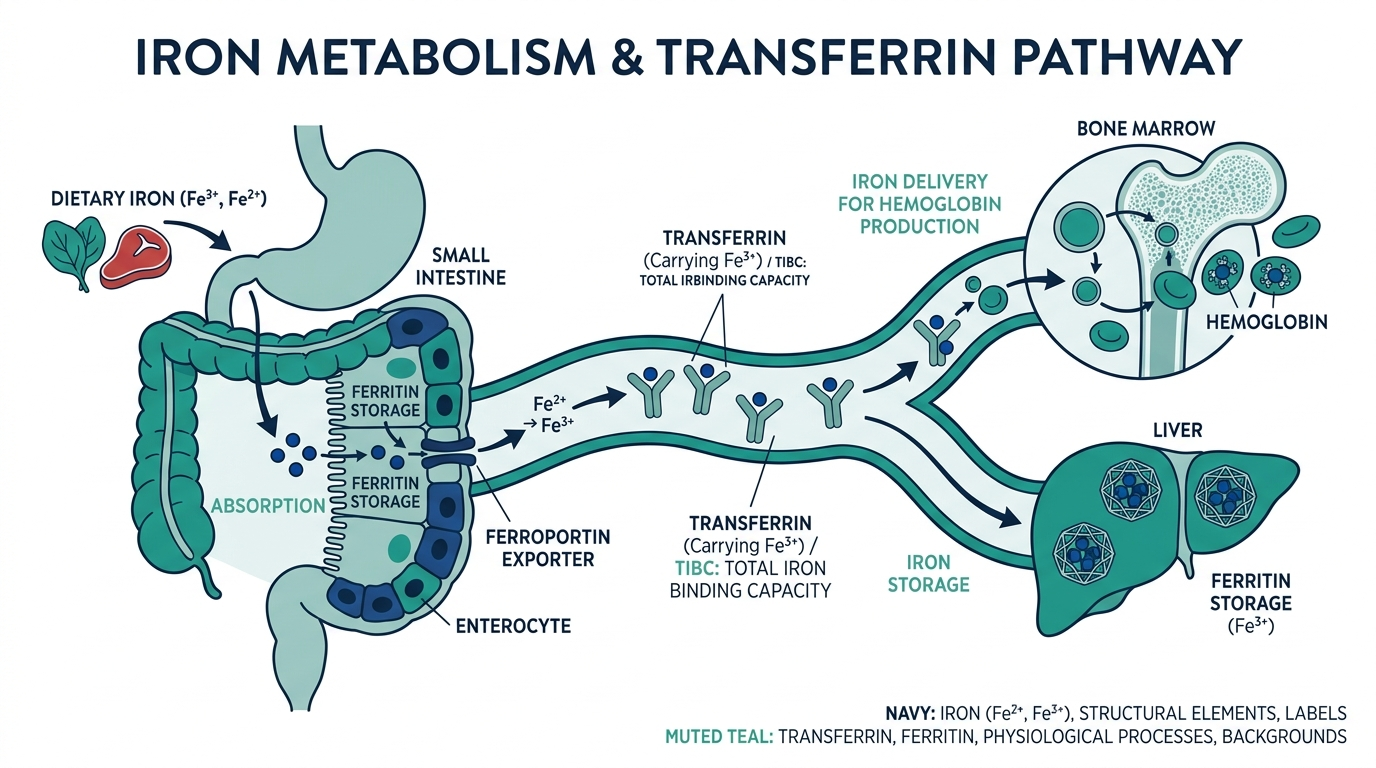
Transferrin is the protein your liver makes to ferry iron through the blood. TIBC estimates how much iron all that transferrin could bind if it were full. When iron is plentiful, transferrin seats fill up and the body makes less of it, so the unused binding capacity drops. That is why TIBC tends to move in the opposite direction of iron stores: high iron, low TIBC.
One number rarely tells the story. TIBC is interpreted alongside serum iron and transferrin saturation, which is normally about 25 to 35 percent (StatPearls, NIH). The pattern of all three is what matters, not TIBC alone.
Optimal versus standard: reading the TIBC range with nuance
Most labs flag TIBC as low below roughly 240 mcg/dL, but the reference band is wide, and a value sitting in the low-normal zone can still be meaningful when it pairs with a high transferrin saturation. Clinicians tend to care less about the exact TIBC digit and more about where it lands relative to serum iron. A TIBC of 250 mcg/dL looks normal on paper, yet if serum iron is high enough to push saturation past 45 percent, that low-normal TIBC is already part of an overload pattern (StatPearls, NIH).
Units trip people up here. Some labs report TIBC in micrograms per deciliter (mcg/dL) and others in micromoles per liter (umol/L), where the normal band is roughly 45 to 80 umol/L. If your number looks wildly different from the 240 to 450 figure, check the units before you worry, because you may be reading a umol/L result against a mcg/dL range. Always compare your value to the reference interval printed on your own report, since instruments and populations shift the cutoffs (Cleveland Clinic).
What causes a low TIBC
The simplest way to actually get this done
Superpower is a full-body lab membership that runs 100+ biomarkers, has each result reviewed by a doctor, and tracks your numbers year over year (about $199/year). It is what we point readers to when they would rather get one clean, complete draw than chase single tests one at a time. Here is superpower reviewed in full.
The most common cause of low TIBC is iron overload, where excess iron fills transferrin and the body downregulates it; the next most common are chronic inflammation, infection, liver disease, and malnutrition (StatPearls, NIH; Cleveland Clinic). These split into two patterns based on what your serum iron is doing.
- Low TIBC with high iron: Suggests iron overload, classically hereditary hemochromatosis, where transferrin saturation climbs well above normal.
- Low TIBC with low iron: Suggests anemia of chronic disease or inflammation, where iron is present but locked away and not easily used.
- Liver disease such as cirrhosis: The liver makes transferrin, so when it is damaged, TIBC falls (StatPearls, NIH).
- Malnutrition and low protein states: Too little protein means too little transferrin, lowering TIBC (StatPearls, NIH).
- Nephrotic syndrome: Protein, including transferrin, is lost in the urine, dropping TIBC (Cleveland Clinic).
Because TIBC falls as part of the acute-phase response, a recent infection or flare of an inflammatory condition can lower it temporarily.
How TIBC fits with the rest of your iron panel
TIBC almost never travels alone. It is one of four numbers that only make sense together: serum iron, ferritin, TIBC, and transferrin saturation. Saturation is simply serum iron divided by TIBC, expressed as a percentage, which is why a low TIBC nudges saturation upward even when iron itself has not moved much (StatPearls, NIH).
Two low-TIBC patterns cover most cases:
- The overload pattern: low or low-normal TIBC, high serum iron, high ferritin, and high saturation. This is the fingerprint of hereditary hemochromatosis and other iron-loading states.
- The inflammation pattern: low TIBC, low serum iron, and a ferritin that is normal or high because ferritin rises as an acute-phase reactant. Here saturation is often low or normal, which separates it from true overload.
Ferritin is the marker that fools people most, because it climbs both when iron stores are genuinely full and when the body is simply inflamed. That is why transferrin saturation, anchored partly by TIBC, becomes the deciding number. If you only remember one thing, remember that a single iron marker cannot settle the question, and TIBC earns its keep precisely because it helps calculate saturation.
There is a practical ordering lesson buried in this. If a clinician draws only a ferritin and it comes back high, that alone cannot tell you whether you are iron loaded or inflamed. Adding TIBC and serum iron, which together produce saturation, is what turns a confusing single value into an answer. This is why a proper iron workup is a small panel rather than one test, and why paying for the panel up front usually saves a second trip to the lab.
Symptoms, or why low TIBC is often silent
Low TIBC itself causes no symptoms, because TIBC is a lab measurement rather than a disease. Any symptoms you feel come from the underlying cause, and many people with mild low TIBC feel completely normal until the driving condition advances (StatPearls, NIH).
When the cause is iron overload, symptoms tend to appear slowly over years and may include fatigue, joint pain, abdominal discomfort, low libido, and a bronze or gray skin tint. In hereditary hemochromatosis these often surface in midlife once iron has accumulated in organs.
When the cause is chronic disease or inflammation, you may notice tiredness, weakness, or pallor from the accompanying anemia, alongside whatever symptoms the primary illness produces. In liver disease or nephrotic syndrome, the dominant signs come from those conditions, such as swelling, jaundice, or foamy urine. The takeaway: do not wait to feel sick, because a low TIBC can show up long before any complaint does.
When a low TIBC is dangerous
A low TIBC becomes concerning when it sits next to a high transferrin saturation, because saturation above roughly 45 percent in screening, and especially above 60 percent, is a strong early signal of iron overload that can damage the liver, heart, and pancreas over time (StatPearls, NIH; Cleveland Clinic). The number itself is not an emergency, but the pattern can be.
Untreated iron overload from hemochromatosis can lead to cirrhosis, liver cancer, diabetes, heart rhythm problems, and joint destruction. These outcomes are largely preventable when iron overload is caught early through the iron panel, which is exactly why a low TIBC with high saturation deserves prompt follow-up rather than a wait-and-see approach.
On the other side, a low TIBC tied to chronic disease signals that an underlying inflammatory or organ condition needs attention. The TIBC is not the threat there; the unaddressed illness is. Either way, a low TIBC that your clinician has not explained is worth a focused conversation.
How to prepare for a TIBC test and what can skew the result
Iron studies are sensitive to timing and preparation, so a single odd TIBC is often worth repeating under clean conditions before anyone acts on it. Most labs prefer a morning draw after an overnight fast, because serum iron can swing by a wide margin across the day and food raises it. Since saturation depends on serum iron, a non-fasting afternoon sample can distort the whole picture even when TIBC itself is stable (StatPearls, NIH).
Things that commonly move these numbers:
- Iron supplements and multivitamins: Taking iron shortly before the draw can spike serum iron and saturation. Many clinicians ask patients to hold supplements for 24 hours before testing, but confirm the exact instruction with the ordering lab.
- Recent inflammation or infection: An acute illness lowers TIBC and can raise ferritin for days to weeks, mimicking the inflammation pattern. Retesting once you are well gives a truer baseline.
- Pregnancy and estrogen: Pregnancy and oral contraceptives tend to raise TIBC and transferrin, so a low TIBC in these settings is less expected and may point more firmly toward overload or protein loss (Cleveland Clinic).
- Recent blood transfusion or iron infusion: Both load the system with iron and can transiently push saturation up and TIBC down.
None of these are reasons to distrust a clearly abnormal panel. They are reasons to standardize the next draw so the trend, not a one-off blip, guides the decision.
What to do next and when to see a doctor
The first step is to look at your low TIBC together with serum iron, ferritin, and transferrin saturation, because that combination usually reveals whether the cause is iron overload or chronic disease (StatPearls, NIH). Ask your clinician for these values if your report shows TIBC alone.
Practical next steps:
- Get the full iron panel: Serum iron, ferritin, and saturation turn an isolated TIBC into a clear picture.
- Share your history: Family history of hemochromatosis, alcohol use, chronic illness, recent infection, and diet all change the interpretation.
- Repeat fasting if needed: Iron studies are often drawn in the morning after fasting because iron levels swing during the day.
- Follow up on high saturation: A saturation above 45 percent may prompt genetic testing for hemochromatosis.
See a doctor promptly if you have fatigue with joint pain and a family history of iron overload, signs of liver disease, or any abnormal iron panel you do not understand. Seek urgent care for severe abdominal pain, confusion, or chest symptoms.
Two real-world patterns behind a low TIBC
Scenario one: the silent overload. A man in his late forties feels a bit tired and has aching knuckles he blames on age. Routine labs show a low-normal TIBC, high serum iron, a high ferritin, and a transferrin saturation over 55 percent. On paper the TIBC looks almost fine, but the trio around it spells iron overload. Genetic testing confirms hereditary hemochromatosis, and because it was caught before organ damage, regular phlebotomy brings his iron down and heads off the cirrhosis and diabetes that late diagnosis invites.
Scenario two: the inflammation mimic. A woman with rheumatoid arthritis shows a low TIBC, low serum iron, and a normal-to-high ferritin. It looks like it could be iron overload at a glance, but her saturation is low, not high. This is anemia of chronic disease, where iron is present but locked away by inflammation. The fix is not iron pills, which would not help and could add to stores; it is better control of the underlying arthritis. These two stories share a low TIBC yet demand opposite responses, which is the whole reason the full panel matters.
The insider nuance most reports miss
Here is what clinicians weigh that a lab printout does not: TIBC and transferrin are essentially measuring the same thing, so when they disagree with ferritin, the body is usually telling a layered story. A low-to-normal TIBC with a high ferritin and high saturation is the fingerprint of true iron overload, while a low TIBC with high ferritin but normal saturation often just means inflammation, since ferritin also rises as an acute-phase reactant (StatPearls, NIH).
This is why ferritin alone fools people. Ferritin can be high from inflammation without any extra iron, so transferrin saturation becomes the deciding number. A low TIBC nudges saturation upward mathematically, which makes reading the trio together essential rather than optional. The practical lesson: never act on a single iron marker, and be skeptical of any iron conclusion drawn from ferritin by itself.
Curious where your TIBC really sits?
Baseline TIBC and 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Is a low TIBC serious?
Not on its own. A low TIBC is a clue that needs context from serum iron, ferritin, and transferrin saturation. It becomes important when paired with high iron and high saturation, which can signal iron overload, or with low iron, which can signal chronic disease.
What is the normal range for TIBC?
The normal TIBC range is generally 240 to 450 mcg/dL, although exact cutoffs vary by laboratory (Cleveland Clinic; StatPearls, NIH). Always compare your result to the reference range printed on your own lab report.
Does low TIBC always mean too much iron?
No. Low TIBC with high serum iron suggests iron overload, but low TIBC with low iron usually reflects chronic inflammation, infection, liver disease, or malnutrition. The serum iron and transferrin saturation determine which pattern applies.
Can low TIBC indicate hemochromatosis?
It can be an early clue. Hereditary hemochromatosis typically shows a low-to-normal TIBC with high serum iron and a transferrin saturation above 45 to 60 percent (StatPearls, NIH). Genetic testing confirms the diagnosis after the iron panel raises suspicion.
How do I raise a low TIBC?
You treat the cause, not the number. If iron overload is responsible, lowering iron raises TIBC. If chronic disease, liver disease, or malnutrition is the driver, addressing that condition and protein status helps. Discuss the right plan with your clinician.
Does pregnancy or birth control affect TIBC?
Yes. Pregnancy and estrogen-containing contraceptives typically raise TIBC and transferrin, so a low TIBC in these situations is less expected and may point more clearly toward iron overload or protein loss (Cleveland Clinic). Mention any hormone use or pregnancy when your iron studies are interpreted.
Should I stop iron supplements before a TIBC test?
Often, yes. Iron taken shortly before the draw can raise serum iron and transferrin saturation and cloud the result. Many clinicians ask patients to hold iron and multivitamins for about 24 hours beforehand, but follow the specific instruction from the lab or ordering provider.
What is the difference between TIBC and transferrin?
They measure nearly the same thing from two angles. Transferrin is the iron-carrying protein itself, while TIBC estimates the total amount of iron all that transferrin could bind. Because they track together, a low TIBC almost always means low transferrin, and labs may report one or the other (StatPearls, NIH).
Can a low TIBC be normal for me?
Sometimes. A stable low-normal TIBC with a normal serum iron, normal ferritin, and normal saturation, no symptoms, and no family history of iron overload is usually just your baseline. What matters is the pattern over time and the company TIBC keeps, not a single reading in isolation.
How soon should I retest a low TIBC?
It depends on the cause. If the low TIBC likely reflects a recent infection or flare, retesting after you recover, often several weeks later, gives a cleaner reading. If the pattern points to iron overload, your clinician will usually move faster to confirm serum iron, ferritin, saturation, and sometimes genetic testing rather than simply waiting.
Sources
- Cleveland Clinic, Total Iron-Binding Capacity (TIBC) Test
- StatPearls, NIH/NCBI Bookshelf, Iron-Binding Capacity
- MedlinePlus, Total iron binding capacity
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related: compare the best at-home biomarker and blood tests.
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


