Last updated June 2026. Educational content, not medical advice. Talk to a licensed dermatologist or clinician before starting any new skincare or supplement regimen.
Short answer: Peptides signal your skin cells to rebuild collagen, relax the muscle contractions that carve expression lines, and reinforce the skin barrier, with the strongest clinical results appearing between weeks 8 and 12 of consistent twice-daily use. A 2025 randomized trial of 70 adults found significant wrinkle-depth improvements as early as day 10 with 1,650 mg daily of low-molecular-weight collagen peptides, and a 2026 systematic review of 19 RCTs covering 1,341 participants confirmed meaningful gains in hydration and brightness. The evidence is real. But the mechanism matters enormously, and most peptide marketing glosses over which type you are actually buying.
Peptides need 8 to 12 weeks to visibly rebuild collagen in your face, so what’s happening internally in the meantime? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Why does your face lose firmness in the first place?
Starting around age 25, your skin produces roughly 1% less collagen per year, and the rate accelerates after menopause due to falling estrogen. Meanwhile, matrix metalloproteinases (MMPs), enzymes the skin uses to remodel the extracellular matrix, become increasingly aggressive with UV exposure and inflammation. The result: the scaffolding that keeps skin dense and resilient thins faster than it rebuilds.
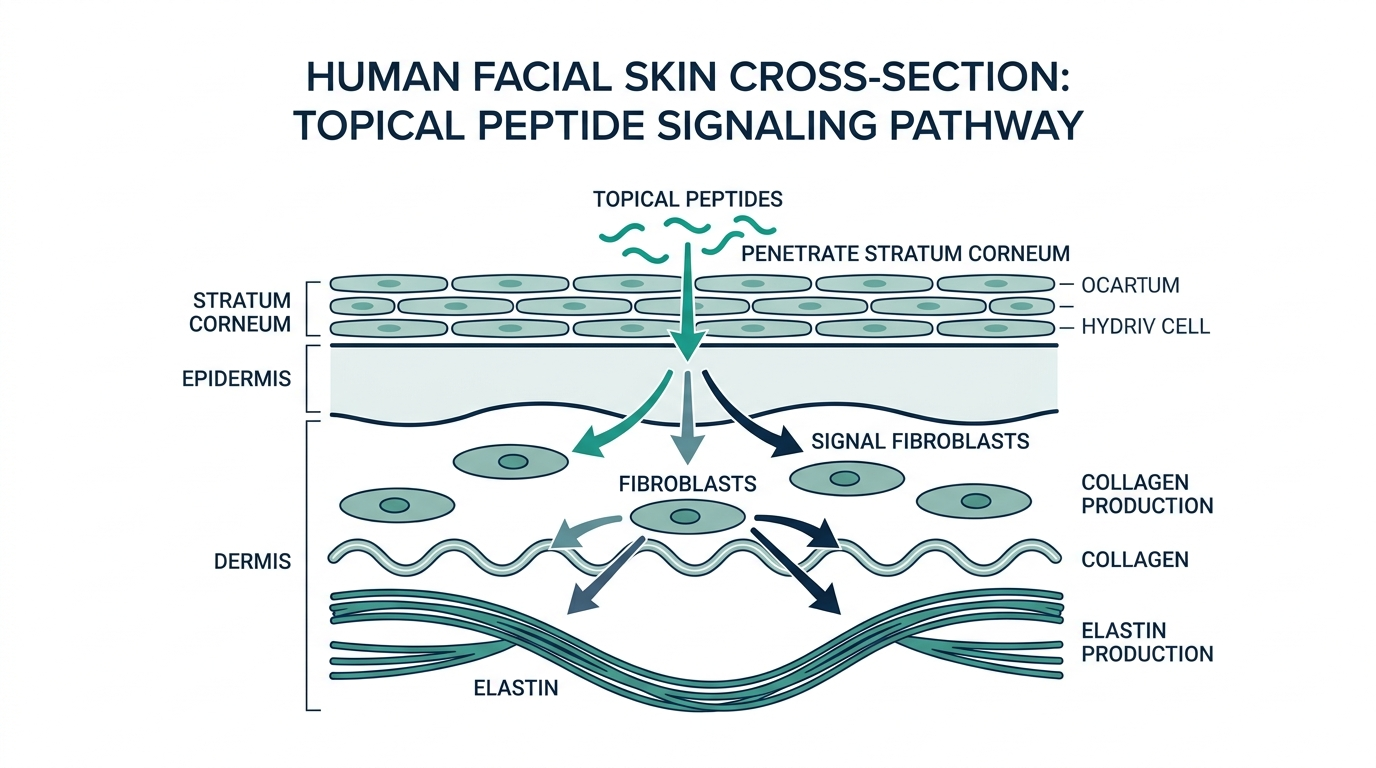
Peptides sit at the intersection of that problem. They are short chains of amino acids, usually 2 to 10 residues long, that behave as molecular messengers. Unlike applying collagen protein topically (which cannot penetrate the skin barrier due to its enormous molecular weight), well-designed peptides are small enough to reach the dermis and tell fibroblasts to do something.
The size distinction matters more than most brands admit. A tub of collagen cream does not rebuild your dermis. A copper tripeptide serum might.
What do peptides actually do inside your skin?
The simplest way to actually get this done
Superpower is a full-body lab membership that runs 100+ biomarkers, has each result reviewed by a doctor, and tracks your numbers year over year (about $199/year). It is what we point readers to when they would rather get one clean, complete draw than chase single tests one at a time. Here is superpower reviewed in full.
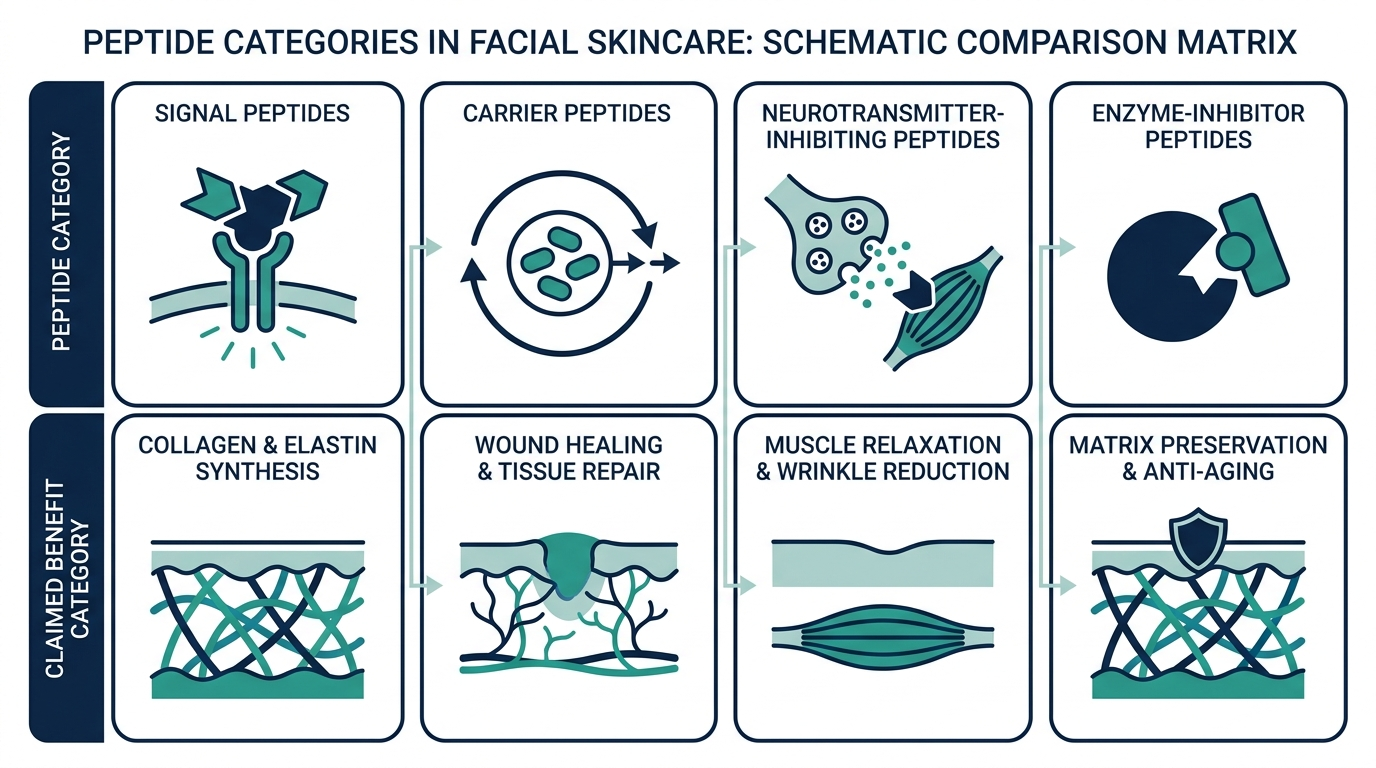
The field distinguishes four functional peptide categories, and knowing which one you are using changes what to expect:
Signal peptides instruct fibroblasts to upregulate collagen, elastin, and glycosaminoglycan production. The flagship example is Matrixyl (palmitoyl pentapeptide-4). A double-blind, placebo-controlled trial with 93 Caucasian women showed visible improvement in fine lines and skin appearance after 12 weeks of twice-daily use, with wrinkle surface area reduced by up to 36% in other controlled studies of the same peptide.
Carrier peptides ferry trace elements, most importantly copper, to the sites that need them. The classic is GHK-Cu (glycyl-L-histidyl-L-lysine copper), which occurs naturally in human plasma at roughly 200 ng/mL around age 20 and falls to about 80 ng/mL by age 60. GHK-Cu stimulates collagen, elastin, and glycosaminoglycan synthesis while modulating thousands of genes involved in tissue repair. An 8-week serum study showed significantly smaller wrinkle depth compared to vehicle-only controls and commercially available Matrixyl 3000 products.
Neurotransmitter inhibitor peptides work like a topical approximation of Botox by blocking acetylcholine release at neuromuscular junctions, which reduces the muscle contractions that deepen expression lines. Argireline (acetyl hexapeptide-3) is the most studied example. A randomized, double-blind trial in Chinese subjects with periorbital wrinkles reported 48.8% anti-wrinkle efficacy versus placebo, and a separate formulation study with 10% Argireline showed up to 30% reduction in wrinkle depth after 30 days. Syn-Ake (tripeptide-3, derived from synthetic temple viper venom) showed up to 52% improvement in forehead fine lines in 45 subjects.
Enzyme inhibitor peptides reduce the activity of collagen-degrading MMPs, effectively slowing the breakdown side of the collagen-loss equation. They pair naturally with signal peptides in well-formulated serums.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
What does the clinical evidence actually show?
The most rigorous recent summary is a 2026 systematic review in Frontiers in Medicine analyzing 19 RCTs and 1,341 participants (mean age 50.2 years). The pooled findings were:
- Wrinkle reduction: statistically significant (p = 0.04), with oral polypeptides driving the strongest effect (pooled mean difference 1.5, p = 0.01)
- Skin hydration: highly significant improvement (MD = 5.79, p < 0.01), with oral tripeptides delivering a mean difference of 16.50 versus 2.37 for placebo
- Brightness: significantly improved (MD = 2.40, p < 0.01)
- Elasticity: minimal and non-significant effect at MD = 0.09
An important caveat the review flags: 17 of the 19 trials tested oral formulations. The topical data, while positive in individual studies, is thinner at the meta-analysis level. Oral peptides, particularly low-molecular-weight collagen peptides at doses of 1,000 to 5,000 mg daily, have the strongest pooled evidence for hydration and wrinkle reduction. Topical peptides have stronger mechanistic rationale for targeted delivery to specific problem areas.
The 2025 trial of 70 adults taking 1,650 mg daily of collagen peptides (94% female, mean age 46.7) showed improvements in crow’s feet depth, nasolabial fold depth, and neck wrinkling beginning at day 10 and sustained two weeks after supplementation ended. Compliance was 98.6% and no adverse events occurred. The mechanism they measured: suppression of MMP-3 and MMP-13 (collagenases) alongside increased dermal fibroblast activity.
Personally, the day-10 onset in that trial surprises most people. The standard expectation is weeks. The explanation is that skin hydration responds faster than collagen remodeling, and early improvements often reflect water retention in the dermis before structural changes accumulate.
How do different peptides compare?
| Peptide | Type | Claimed benefit | Strongest evidence | Typical product concentration |
|---|---|---|---|---|
| Palmitoyl pentapeptide-4 (Matrixyl) | Signal | Collagen synthesis, wrinkle reduction | Up to 36% wrinkle surface reduction in 12-week DBT | 0.005% to 0.01% |
| Palmitoyl tripeptide-1 + tetrapeptide-7 (Matrixyl 3000) | Signal | Collagen I, III, IV, fibronectin | Considered superior to original Matrixyl in head-to-head data | Varies |
| Acetyl hexapeptide-3 (Argireline) | Neurotransmitter inhibitor | Expression line reduction | 48.8% anti-wrinkle vs. placebo in periorbital RCT | 5% to 10% |
| Tripeptide-3 (Syn-Ake) | Neurotransmitter inhibitor | Forehead fine lines | 52% improvement in 45 subjects | 4% to 8% |
| GHK-Cu (copper tripeptide-1) | Carrier | Collagen, elastin, repair, anti-inflammatory | 28% collagen density increase in 21-person IRB trial at 3 months | 0.05% to 1% |
| Manganese tripeptide-1 | Carrier | Hyperpigmentation, fine lines | Significant hyperpigmentation reduction in 15 subjects age 40 to 70 | 0.005% |
| Low-MW collagen peptides (oral) | Signal (systemic) | Hydration, wrinkle depth, elasticity | Meta-analysis of 17 RCTs; significant hydration and brightness | 1,000 to 5,000 mg/day |
Building a face peptide routine that actually works
Peptides reward consistency more than cleverness, but the order you apply them to your face still matters. Here is a simple template that respects the compatibility rules without turning your bathroom into a chemistry lab.
Morning: cleanse, then vitamin C, then let it absorb for a minute, then a peptide serum, then moisturizer, then SPF. Vitamin C and most signal peptides coexist fine in the same routine. The one exception is a dedicated copper peptide, which you should not pair with vitamin C.
Evening: cleanse, then peptide serum on slightly damp skin, wait a minute, then retinol if you use it, then moisturizer to seal everything in. If you run a copper peptide, this is its home, kept well away from the morning vitamin C.
Apply to the whole face, but press an extra drop into the zones that age first: the crow’s feet at the outer eye, the nasolabial folds running from nose to mouth, the forehead, and the neck, which people forget until it gives their age away. Two to three drops covers face and neck. More serum does not absorb better, it just runs off.
How long does it take to see results?
Realistic expectations matter more than most brands want to admit. The honest timeline based on clinical data:
- 2 to 4 weeks: Hydration improvements and a subtle luminosity shift are often the first changes you notice. These reflect the hyaluronic acid upregulation and barrier-strengthening effects.
- 6 to 8 weeks: Surface texture, pore appearance, and early firmness changes become visible. This is when most users either stick with a product or abandon it before the real payoff.
- 10 to 12 weeks: Collagen-density changes become measurable. This is the window for the full anti-wrinkle and firming outcomes documented in most trials. The Matrixyl studies, the GHK-Cu IRB trial, and the 2025 collagen peptide RCT all hit statistical significance in this window.
- 3 to 6 months: Peak structural remodeling for daily-use serums. Some benefits, notably elasticity, continue to improve with longer use.
Do not believe brands promising dramatic transformation in two weeks. The biology does not permit it. The collagen synthesis pathway requires time, cofactors, and repetition.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
Matching the peptide to the part of your face
Different areas of the face age through different mechanisms, so the smartest serum choice depends on where your main concern sits.
- Forehead lines and crow’s feet are expression-driven, carved by repeated muscle movement. This is the zone where neurotransmitter-inhibiting peptides like Argireline and Syn-Ake earn their place, softening the micro-contractions that etch those lines deeper each year.
- Nasolabial folds and overall cheek firmness are structural, about collagen density in the mid-face. Signal peptides such as Matrixyl and carrier peptides like GHK-Cu are the better match here, because the problem is a thinning scaffold rather than muscle motion.
- Under-eye crepiness and thin skin respond best to gentle barrier-supporting peptides plus copper peptides, since the skin there is delicate and intolerant of harsher actives.
- The neck and jawline need the same signal and carrier peptides as the mid-face, applied with the same discipline, because neck skin has fewer oil glands and shows laxity early.
A well-built multi-peptide serum covers several of these at once, which is why combination formulas are popular. Just remember that a formula only helps a zone if the relevant peptide is present at a real concentration, not a trace.
Which peptide products are worth considering?
The market spans three price bands, and the correlation between price and efficacy is not linear.
Budget tier ($10 to $30): The Ordinary’s Multi-Peptide + HA Serum packs eight peptides, including 1% copper tripeptide-1, at around $12 for 30 mL. For pure peptide delivery on a tight budget, it is difficult to beat. The Inkey List Collagen Booster Peptide Serum runs around $15 and layers well under moisturizer.
Mid-tier ($35 to $80): Paula’s Choice Pro-Collagen Multi-Peptide Booster concentrates signal and carrier peptides in a dropper format. NIOD CAIS 3:1, at approximately $55, delivers 3% GHK-Cu alongside a ceramide complex. Olay Regenerist Collagen Peptide 24 MAX Serum hits this range with vitamin B3 (niacinamide) added, which assists barrier function and brightening separately.
Premium ($100+): SkinMedica TNS Advanced+ Serum uses a dual-chamber pump that mixes growth factors with peptides at application, around $280 for 1 oz. The evidence base for growth factor serums is meaningful but mostly proprietary. NIOD Copper Amino Isolate Serum 1:1 is a dedicated copper-peptide product for anyone prioritizing GHK-Cu above other peptide types.
Two things the product pages rarely clarify: concentration and vehicle. A peptide at 0.001% in a formula does nothing measurable. And a poorly designed emulsion that degrades the peptide before it absorbs negates the active entirely. Brands that publish their actual concentrations and third-party stability data deserve the benefit of the doubt.
What should you NOT mix with peptides?
The layering question trips up more experienced skincare users than beginners, because the rules are counterintuitive:
AHAs and BHAs: Use acid exfoliants on alternate evenings or wait at least 30 minutes. Peptide bonds can hydrolyze at very low pH, degrading the peptide before it penetrates. This is more of a concern with high-concentration acid products (20%+ glycolic) than with typical daily-use formulations around pH 3.5.
Vitamin C (L-ascorbic acid): Apply first in the morning, before your peptide serum, and let it absorb. Vitamin C is most effective at low pH; layering it over a peptide serum that has buffered skin pH upward reduces its stability.
Copper peptides and retinol: These can be used in the same routine, but not in the same layer at the same moment. Apply copper peptide serum first, wait 10 to 20 minutes, then apply retinol. The copper in GHK-Cu can oxidize retinol if they sit together in a wet layer.
Copper peptides and strong antioxidants (vitamin C, E): These compete for the same skin absorption pathways. Separate them by routine (vitamin C in AM, copper peptide in PM) rather than stacking in one session.
What pairs beautifully with peptides: hyaluronic acid, niacinamide, ceramides, panthenol. These are all barrier-supportive, non-reactive, and amplify the hydration and repair effects without interfering with peptide stability.
Myth-busting: three things peptide marketing gets wrong
Myth 1: Collagen creams and collagen peptides are the same thing. Applying a cream made with collagen protein does not deliver collagen to your dermis. Collagen’s molecular weight runs 300,000+ daltons; the theoretical maximum for skin penetration is around 500 daltons. Collagen creams moisturize via occlusion, not structural delivery. Hydrolyzed collagen peptides, at 1,000 to 5,000 daltons depending on the hydrolysis degree, are small enough to be absorbed in topical formulations and meaningfully small in oral supplements.
Myth 2: More peptides in a formula means better results. Formulas listing eight, ten, or twelve peptides are marketing constructs, not evidence of synergy. The key variables are whether the active peptides are at efficacious concentrations and whether the formula preserves their stability. Three well-dosed peptides in a stable vehicle beat twelve at trace concentrations every time.
Myth 3: Peptides are gentle alternatives that work slowly. Signal peptides and copper peptides are genuinely mild, but neurotransmitter inhibitor peptides (Argireline, Syn-Ake) cause real and measurable muscle relaxation over time. They are not Botox in a bottle, the depot effect and localized concentration achievable with an injection are categorically different, but calling them “just moisturizing” undersells what they do.
What about peptide injections and injectables?
Topical peptides are cosmetics and are legally sold without a prescription. Injectable peptide formulations, including injectable GHK-Cu, are an entirely different regulatory and risk category.
The distinction is important: GHK-Cu at 0.05% to 1% in a serum has decades of published topical safety data. The same molecule prepared as an injectable solution, unlicensed and sold by a research-chemical vendor, carries an unverified purity profile and zero clinical oversight. This is the gap between “cosmetic peptide skincare” and “research peptide therapy,” and the gap is not small.
For anyone interested in peptide therapy beyond topical skincare, whether for systemic aging, recovery, or hormonal health, the path with any real accountability is a licensed telehealth clinic prescribing from a named compounding pharmacy, not a grey-market vendor. As of mid-2026, platforms like Defy Medical and Marek Health operate in exactly that licensed lane with prescription-grade peptide protocols supervised by a clinician.
Don’t just read about your health, track it.
A single result is a snapshot. Superpower re-tests 100+ markers over time so you can watch them move as you change sleep, food, and training.
FAQ
Do peptides actually work for the face?
Yes, with specifics. Signal peptides like Matrixyl reduce wrinkle surface area by up to 36% in 12-week double-blind trials. Argireline reduces expression-line depth by up to 30% at 10% concentration. Oral collagen peptides show significant hydration and wrinkle improvements across a 2026 meta-analysis of 19 RCTs and 1,341 participants. The evidence is real; the caveat is that results require consistent twice-daily use for at least 8 to 12 weeks.
Which peptide is best for anti-aging?
It depends on your primary concern. For collagen synthesis and wrinkle reduction: palmitoyl pentapeptide-4 (Matrixyl) or the newer Matrixyl 3000 blend. For repair, skin density, and anti-inflammatory effects: GHK-Cu (copper tripeptide-1). For expression lines around the eyes and forehead: acetyl hexapeptide-3 (Argireline) or tripeptide-3 (Syn-Ake). Most well-formulated serums combine signal and carrier peptides to address multiple mechanisms simultaneously.
Can I use peptides every day?
Yes. Peptides are among the best-tolerated active ingredients in skincare. They are safe for daily use, morning and evening, and are generally compatible with sensitive, acne-prone, rosacea, and post-procedure skin. Unlike retinol or acids, they do not cause initial purging or photosensitivity.
Are oral collagen peptides worth taking for facial skin?
The evidence is stronger for oral than most people expect. A 2025 RCT showed significant wrinkle-depth improvements from day 10 at 1,650 mg/day, and a 2026 meta-analysis found significant pooled effects on hydration and brightness from oral formulations. The catch: if you are deficient in vitamin C, zinc, or iron, collagen synthesis stalls regardless of supplementation. Test your levels before committing to a 90-day protocol.
How do peptides compare to retinol?
Retinol drives cell turnover and directly upregulates collagen gene expression, with a larger body of evidence than most individual peptides. Peptides are gentler, non-photosensitizing, and work well in combination with retinol. The optimal approach for most people over 35 is retinol in the evening plus a peptide serum in the morning, not choosing between them.
Can peptides replace Botox?
No, honestly. Neurotransmitter inhibitor peptides (Argireline, Syn-Ake) relax surface muscles via a similar but far weaker mechanism than botulinum toxin injections. They soften the appearance of expression lines over time, which is meaningful, but the depot effect and localized concentration achievable with an injection are in a different category entirely. Peptides extend the interval between injections for some people. They are not a clinical substitute.
Are there any side effects from peptide skincare?
Topical peptides at normal cosmetic concentrations (under 10%) have an excellent safety record. Mild stinging is occasionally reported with Argireline at high concentrations, and some users experience temporary skin tightness after first using copper-peptide serums. Allergic contact dermatitis to peptide actives is rare. The more common issue is choosing a formula with sub-efficacious concentrations, which wastes money without causing harm.
Can peptides help with under-eye bags or dark circles?
Partly, and only for some causes. Peptides can thicken and firm the thin under-eye skin over time, which softens fine crepiness and the shadowing that comes from translucency. They do nothing for puffiness driven by fluid, allergies, or fat pad position, and little for dark circles that are purely pigment or genetics. Set expectations by cause: structural crepiness responds, plumbing and pigment issues do not.
Are peptides safe to use on the face during pregnancy?
Topical cosmetic peptides are generally considered low risk in pregnancy, and they are a common stand-in for retinol, which is avoided during pregnancy. That said, guidance varies by ingredient and pregnancy is exactly the time to run any routine past your obstetrician rather than trusting a label. The neurotransmitter-inhibiting peptides in particular have less pregnancy-specific data than the plain signal and hydration peptides.
How much peptide serum should I use on my face?
Two to three drops is enough for the whole face and neck. Peptides work by signaling, not by saturation, so doubling the amount does not double the benefit. Consistency twice a day for at least eight to twelve weeks moves the needle far more than a heavier single application.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources
- Frontiers in Medicine (2026). Oral and topical peptides for skin aging: systematic review and meta-analysis of randomized controlled trials. https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2026.1618306/full
- PubMed Central (2025). Skin Anti-Aging and Moisturizing Effects of Low-Molecular-Weight Collagen Peptide Supplementation in Healthy Adults. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12438954/
- PubMed Central (2025). Peptides: Emerging Candidates for the Prevention and Treatment of Skin Senescence. https://pmc.ncbi.nlm.nih.gov/articles/PMC11762834/
- Grand Ingredients. GHK-Cu Peptide: Clinical Evidence & Skin Benefits 2025. https://grandingredients.com/copper-peptides-clinical-benefits/
- Superpower. Peptide Moisturizers and Creams: What to Look For. https://superpower.com/guides/peptide-moisturizer
- Superpower. Biomarker Blood Testing. https://superpower.com/blood-test-for-biomarkers
- FormBlends. Best Skin Peptides (2026): Evidence-Ranked Guide. https://formblends.com/articles/peptide-hub/best-best-skin-peptides
- Klow Peptide. Matrixyl vs Argireline: Which Peptide Works Best? (2026). https://klow-peptide.com/en/articles/matrixyl-vs-argireline/
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.