Last updated 18 June 2026. Educational content, not medical advice. Most peptides sold online carry “for research use only” labels and are not approved for human use. Speak to a licensed clinician before starting any injectable program.
Short answer: Some peptides are among the most rigorously tested drugs in medicine. GLP-1 receptor agonists like semaglutide and tirzepatide have over 20 years of clinical data and more than 80 FDA-approved peptide drugs exist across all categories. Oral collagen peptides have 19 randomized controlled trials behind them. But the injectable “research peptides” most people ask about, including BPC-157, TB-500, CJC-1295, and retatrutide, have almost no published human safety data. The safety question does not have one answer: it has one answer per peptide type, and the honest version of each answer is very different from what the forums say.
GLP-1 peptides have 20 years of clinical data, but your own bloodwork is the data that matters most for you. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Why “are peptides safe” is the wrong question to Google
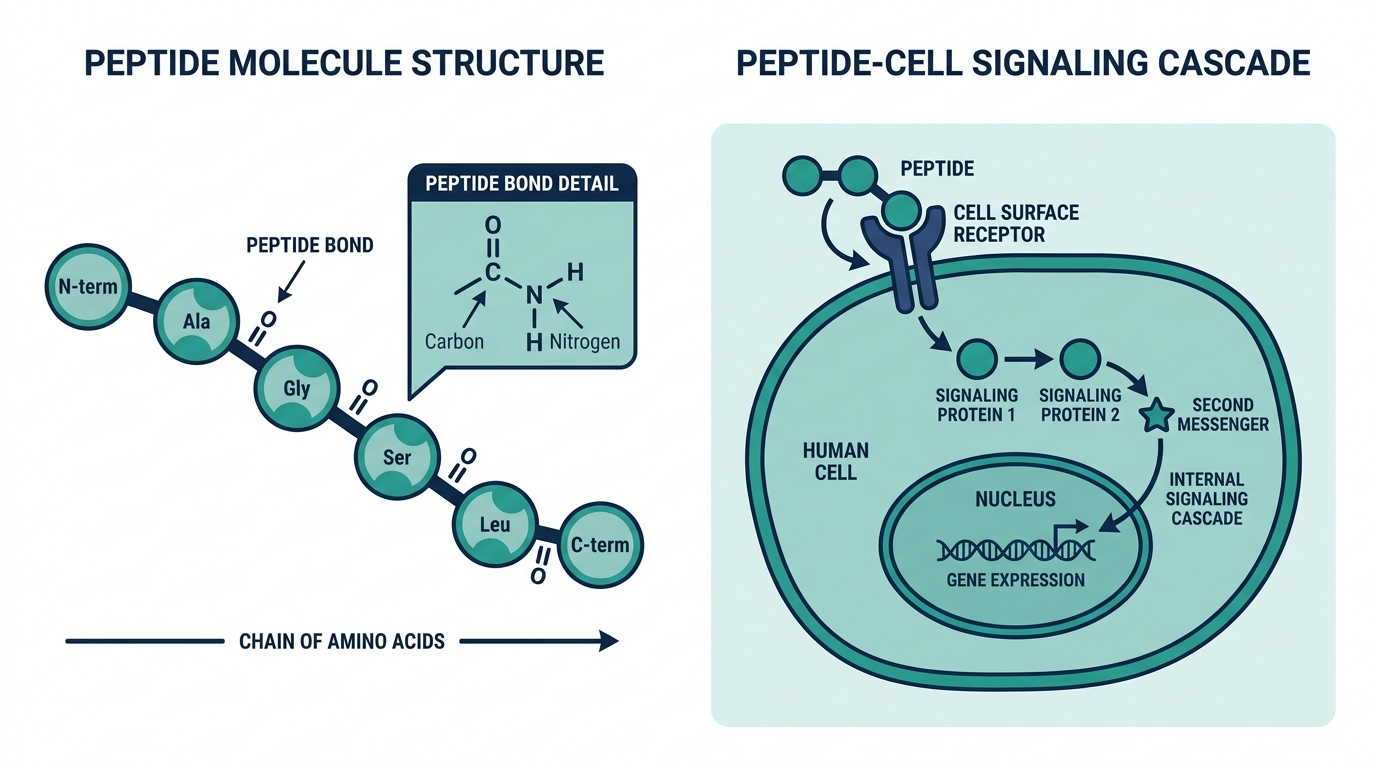
Peptides are not a category the way “supplements” is a category. They are a structural description: any chain of 2 to 50 amino acids linked by peptide bonds. That definition covers insulin, the first injectable peptide therapy and one of the most studied drugs in history, and it also covers retatrutide, a weight-loss molecule that independent testing found at less than 75% purity in multiple batches at one of the grey market’s most-trusted vendors, Peptide Sciences, before it shut down in March 2026.
Asking whether peptides are safe is like asking whether liquids are safe. The answer is completely determined by which one, at what dose, from what source, administered how, and into whose body.
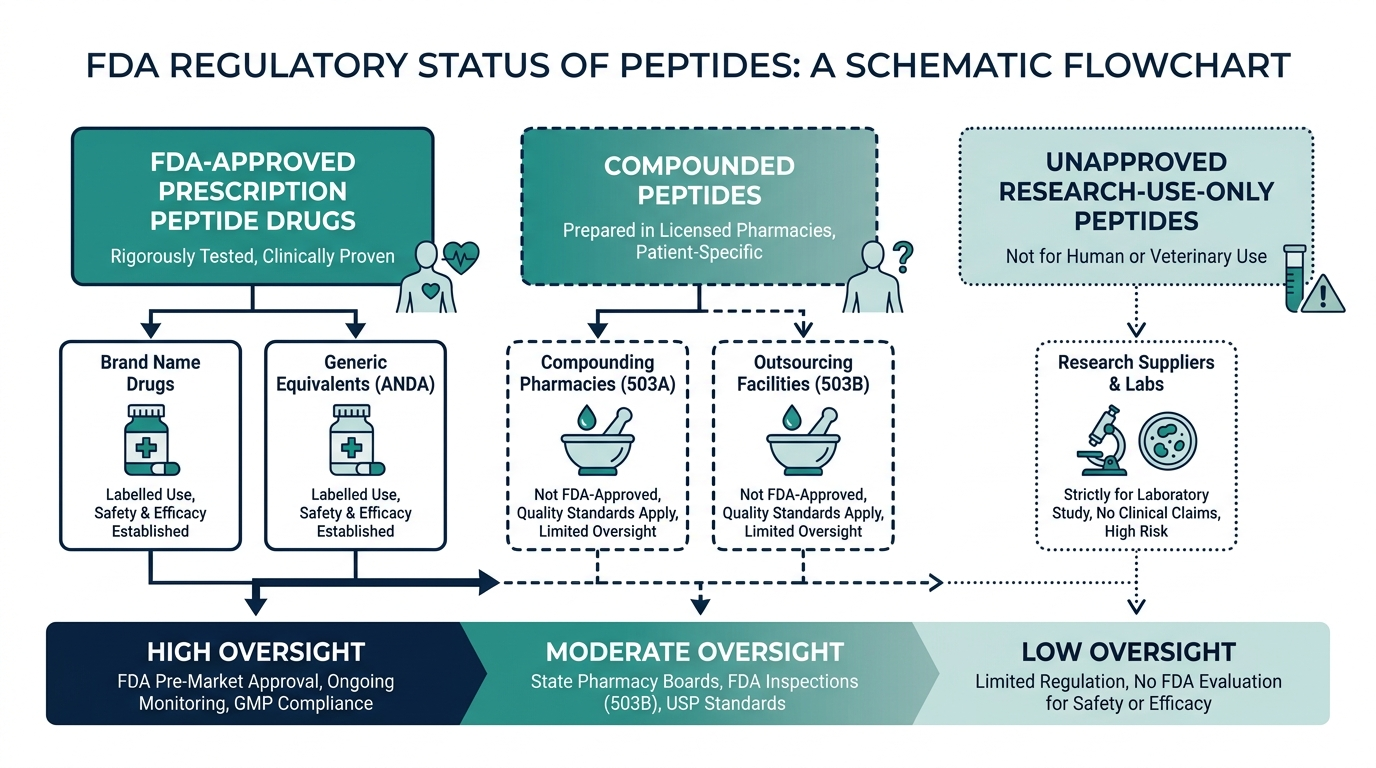
What follows is the real breakdown by category. Each category has a different evidence base, a different regulatory status, and a different risk profile. None of them is zero risk. The first category is as close to zero as pharmaceutical science gets.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Are FDA-approved peptides safe?
The simplest way to actually get this done
Superpower is a full-body lab membership that runs 100+ biomarkers, has each result reviewed by a doctor, and tracks your numbers year over year (about $199/year). It is what we point readers to when they would rather get one clean, complete draw than chase single tests one at a time. Here is superpower reviewed in full.
Yes, with documented side effects and extensive clinical-trial monitoring. There are over 80 FDA-approved peptide drugs, covering diabetes, weight management, fertility, cardiovascular disease, cancer, and sexual function. These are the most studied peptides in the world. Insulin, a 51-amino-acid peptide, has been in clinical use since 1921. Semaglutide and tirzepatide, the GLP-1 class driving the weight-loss conversation, went through massive phase 3 programs before approval.
The SURMOUNT-1 trial for tirzepatide enrolled 2,539 adults and reported mean body-weight loss of 22.5% at the highest dose. A 2026 meta-analysis of 10 tirzepatide trials covering 6,836 participants documented adverse events thoroughly: nausea in roughly 37% of users, vomiting in 16%, constipation in 15%, and discontinuation due to side effects in 4 to 6% of participants. Those numbers sound alarming until you compare them to placebo groups, where 76.7% of participants in SURMOUNT-3 reported at least one adverse event. The point is not that GLP-1s are without side effects. The point is that their side effects are known, quantified, and manageable through dose titration, because 20 years and tens of thousands of trial participants said so explicitly.
Thyroid C-cell tumors appeared in rodent carcinogenicity studies for both semaglutide and tirzepatide. FDA labeling carries a warning. No increase in human thyroid cancer has been demonstrated, but anyone with a personal or family history of medullary thyroid carcinoma should not use GLP-1s.
A rule worth memorizing: the safety profile of any peptide is as good as the clinical trial program behind it. GLP-1s have massive trial programs. Most research peptides have none.
Are collagen peptides safe? (The most asked, easiest answered)
Yes. Oral collagen peptides have the best safety profile of any peptide category, backed by actual RCTs. A 2026 systematic review and meta-analysis published in Frontiers in Medicine analyzed 19 randomized controlled trials with 1,341 participants and found “minimal adverse events,” limited to isolated cases of mild gastrointestinal discomfort. No serious adverse events were reported across the full trial pool.
The efficacy signal is real, not just the safety. The same meta-analysis found significant wrinkle reduction (MD = 0.27, p = 0.04), improved skin hydration for oral tripeptides (MD = 5.79, p < 0.01), and significant skin brightness improvement (MD = 2.40, p < 0.01). A separate double-blind placebo-controlled trial found that 12 weeks of bioactive collagen peptide supplementation produced lasting improvements in skin hydration and dermal structure even after a 4-week washout period.
The mechanism is well-understood. Hydrolyzed collagen breaks into bioactive di- and tripeptides that are transported across the intestinal wall by the PEPT-1 transporter. They are not absorbed as intact large proteins, which eliminates the allergic-reaction risk that comes with higher-molecular-weight biologics.
Myth-buster: “Collagen supplements are just expensive protein.” The absorption mechanism matters. Collagen-derived di- and tripeptides, particularly those rich in hydroxyproline, behave differently from whey protein fragments. The skin-benefit signal in the RCT pool is specific to collagen hydrolysates, not to dietary protein in general. That is not marketing language; it is the finding from the clinical data.
Sensible precautions for collagen supplements: choose brands with third-party testing (NSF Certified or Informed Sport certified), verify the source (marine, bovine, chicken), and check for heavy metal testing, especially in marine-sourced products.
Are injectable research peptides safe?
This is the hard question, and the honest answer is that we do not have enough human data to say definitively, for most of them.
Take BPC-157, the most popular research peptide by search volume. Animal studies are extensive and promising. Rat and mouse models show accelerated tendon repair, gut-healing properties, and neuroprotective effects. But the human evidence base, as of mid-2026, consists of exactly three small published studies: a 2024 pilot in 12 patients with interstitial cystitis, a 2021 knee-pain study in 16 patients, and a 2025 IV safety study in 2 adults. No randomized controlled trials. No placebo arms. No pharmacokinetic data to confirm how humans actually metabolize it. We do not know the right dose for a human. We do not know how long it takes to clear. We do not know the threshold at which it causes harm.
Growth hormone secretagogues like CJC-1295 and Ipamorelin have a different evidence gap: we understand the mechanism well (stimulating endogenous GH release), and the clinical concern is specific. Chronically elevated IGF-1, which these peptides produce, carries published epidemiological evidence of modestly increased risk for colorectal, breast, and prostate cancers. Research published in The Lancet Oncology found that higher circulating IGF-1 correlated with increased risk in several cancer types. The biological rationale is clear: IGF-1 receptor activation promotes cell proliferation, inhibits apoptosis, and encourages angiogenesis. This does not mean every user will develop cancer. It means anyone considering this class of peptide should have a baseline IGF-1 drawn and should have a clinician review their personal and family cancer history before starting.
| Peptide | Evidence base | Key specific risk | Route |
|---|---|---|---|
| Semaglutide / Tirzepatide | Phase 3 RCTs, 20,000+ participants | Nausea (37%), thyroid C-cell tumor signal in rodents | Subcutaneous injection (prescription) |
| Sermorelin | Phase 2 clinical program, FDA-approved 1997 | Headache, flushing; IGF-1 elevation requires monitoring | Subcutaneous injection (prescription/telehealth) |
| BPC-157 | 3 small pilot studies, no RCTs | Unknown metabolic fate in humans; purity/contamination from grey sources | Research only; injectable or oral |
| TB-500 (Thymosin Beta-4) | Animal data; no published human trials | Unknown; frequently paired with BPC-157 | Research only; injectable |
| CJC-1295 / Ipamorelin | Pharmacology well-understood; limited human RCTs | Chronic IGF-1 elevation; cancer-history contraindication | Research only; injectable |
| Retatrutide | Phase 2 trial (Eli Lilly) as prescription drug | Not approved; grey market product failed independent purity testing | Research only; injectable |
| GHK-Cu (topical) | Multiple RCT-backed skin studies | Excellent topical safety profile | Topical cosmetic |
| GHK-Cu (injectable) | Very limited | Elevated to different risk class from topical | Research only; injectable |
| Oral collagen peptides | 19 RCTs, 1,341 participants | Minimal; rare mild GI discomfort | Oral supplement |
The table shows the asymmetry clearly. The safest peptides have the most human data. The most hyped injectable research peptides have the least.
What makes a research peptide genuinely dangerous?
The answer is usually not the molecule itself. It is the five things that happen before the molecule reaches you.
1. Unknown purity. Independent testing in 2024 found that up to 40% of grey-market peptide samples contained incorrect dosages or undeclared ingredients, and nearly 25% contained compounds not listed on the label. The Finnrick independent testing database, which has run more than 8,000 tests across 225 vendors, failed Peptide Sciences’ retatrutide with an “E” rating across 37 batches, with purity dipping as low as 75%. A 75%-pure vial is a 25%-mystery. No one can tell you what the mystery 25% is.
2. Bacterial endotoxins. Endotoxins are fragments of bacterial cell walls that contaminate improperly manufactured peptides. Even a small endotoxin load injected subcutaneously causes inflammatory reactions: fever, chills, hypotension. In severe cases, it can look like sepsis. Pharmaceutical-grade peptides must clear a pyrogen test. Research-grade peptides are not required to. Some vendors test for endotoxins voluntarily. Most do not.
3. Self-administered injection errors. The clinical literature is consistent: injection-site infections, abscesses, and tissue damage are documented complications of unsupervised self-injection. Proper sterile technique, swabbing stoppers, using insulin syringes, choosing correct sites, rotating sites, and disposing of sharps correctly is a trainable skill. Most people who buy a grey-market vial have never been trained. Three people at a Las Vegas anti-aging festival were fined by authorities after two attendees became critically ill following unsupervised peptide injections; causes remained undetermined. That story is not a reason to panic. It is a reason to take the “trained clinician” part seriously.
4. Reconstitution errors. Most injectable research peptides are lyophilized (freeze-dried) powders that must be reconstituted with bacteriostatic water before injection. Getting the concentration math wrong by one decimal place changes your dose by a factor of ten. Not five percent. Ten times. A 500 mcg dose intended as BPC-157 becomes 5,000 mcg if someone misreads the syringe markings. No one will know until something goes wrong.
5. Drug interactions. Peptides affecting the GH-IGF-1 axis can require adjustments to thyroid medication, insulin, and blood pressure drugs. A grey-market vial comes with no pharmacist, no interaction check, and no one whose license is at stake if those interactions matter for your specific situation.
Personally, I think the forum culture underweights these five risks because the population of people who report outcomes skews heavily toward younger, healthy adults doing relatively short cycles at reasonable doses and sourcing from the handful of vendors who actually publish third-party COAs. The tail of the distribution, the people who got a contaminated batch, developed an infection, or misjudged a dose, is mostly invisible online because those are not the stories people post.
Who should not use injectable peptides at all?
The contraindications for clinically supervised peptide therapy are narrow but firm. Anyone outside a supervised clinical setting should treat these as personal red lines:
Active or recent malignancy. Growth hormone secretagogues (sermorelin, CJC-1295, ipamorelin) are contraindicated in patients with active cancer. IGF-1 elevation can theoretically promote tumor growth by activating cell-proliferation pathways. This is not a theoretical footnote; it is a hard clinical contraindication that every credentialed peptide clinic enforces.
Pregnancy and breastfeeding. No injectable therapeutic peptide has been adequately studied in pregnant or nursing women. This is a blanket contraindication for the entire category except insulin and the few drugs with pregnancy-specific labeling.
Personal or family history of medullary thyroid carcinoma or MEN2. The thyroid C-cell tumor signal in GLP-1 rodent studies creates a specific contraindication for semaglutide and tirzepatide in these populations, written directly into prescribing information.
Uncontrolled diabetes or insulin resistance. Peptides affecting the GH axis alter insulin sensitivity in ways that can destabilize glucose management. This is not a contraindication to supervised care; it is a contraindication to unsupervised grey-market self-dosing.
Severe autoimmune conditions. Immune-modulating peptides, including thymosin alpha-1 and BPC-157 at high doses, require careful physician evaluation before use in active autoimmune disease. The evidence is not clear in either direction, which is exactly the problem.
A subtlety worth flagging: the “no cancer history” rule applies mainly to growth-hormone-affecting peptides. The GLP-1 class is actively being investigated for potential anti-tumor properties in insulin-resistant cancers, which makes the picture more nuanced than a blanket “peptides and cancer don’t mix.” But that research is preliminary and does not change the contraindication for the GH axis class.
What does “safe” actually mean in the clinical lane?
The telehealth peptide market has matured enough in 2026 that “supervised” and “unsupervised” are genuinely different products, not just different prices for the same molecule.
Clinics like Defy Medical, Marek Health, and Hone Health now offer structured peptide programs with baseline labs required before any prescription, not optional. Defy Medical charges $99 to $150 per month with a 40+ biomarker baseline panel. Marek Health runs $225 to $350 a month with a 65 to 100+ biomarker panel and prescribes sermorelin, CJC-1295/Ipamorelin, GHK-Cu, and BPC-157 through named licensed compounding pharmacies. Sermorelin specifically is available through telehealth at $175 to $225 a month compared to $600 to $1,200 for traditional synthetic HGH. Broader peptide therapy programs typically run $199 to $399 a month with monitoring included.
What “safe” means inside that lane: the prescription comes from a licensed clinician. The compound is dispensed from a named, verifiable 503A compounding pharmacy subject to USP 797 sterile compounding standards, which specify endotoxin testing, environmental monitoring, and batch release criteria. Follow-up labs catch early signals before they become problems.
Do not believe any clinic that offers injectable BPC-157, TB-500, or CJC-1295 without requiring a consultation, baseline labs, and follow-up monitoring. That is not a real clinical program. It is a grey-market vendor with a better website.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
The regulatory shift in 2026 changes the calculation
A specific development in 2026 is reshaping the safety landscape for the most popular research peptides. On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. announced that 14 of 19 previously restricted peptides are expected to return to legal compounding status, including BPC-157, thymosin alpha-1, TB-500, CJC-1295, and ipamorelin. The Pharmacy Compounding Advisory Committee was scheduled to meet July 23-24, 2026, to finalize that reclassification.
The FDA had removed BPC-157 from its Category 2 (potentially unsafe) list on April 22, 2026, reversing the 2023 restriction. That is a meaningful signal. The FDA’s original 2023 restriction cited peptide-related impurities, immunogenicity risk, and insufficient human safety data. The reversal signals not that those concerns have been fully resolved, but that the risk-benefit picture under supervised compounding is being reassessed.
What this means practically: the safest way to access BPC-157 or CJC-1295 may become the licensed compounding pharmacy route, not the grey-market vial. The gap between the safe option and the accessible option is closing. The grey-market reason to self-source these peptides is narrowing by the month.
How to assess any peptide’s safety before using it
Five questions worth asking before any injectable peptide, regardless of source:
1. What human clinical data exists? Not animal data. Not anecdotes. Published human studies, ideally randomized controlled trials, with sample sizes, adverse event reporting, and a methods section you can read. For GLP-1s, there are thousands of pages. For most research peptides, there are a handful of pages at best.
2. Is the source verifiable? For prescription peptides, the compounding pharmacy name is on the label and verifiable. For research peptides, a real third-party Certificate of Analysis from Janoshik Analytical, MZ Biolabs, or Colmaric Analyticals is the minimum. The batch number on the COA must match the number on the vial. The purity must clear 96% HPLC, and a Mass Spectrometry identity match must confirm the molecule is actually the one named on the label.
3. Does any clinician stand behind this dose for your specific situation? The dose that improved BPC-157 outcomes in a 16-person knee-pain pilot is not a dose recommendation for your body weight, health history, or concurrent medications. A clinician who has reviewed your labs and medical history and written a specific prescription is structurally different from a forum consensus dosing protocol, regardless of how many people upvoted it.
4. Do you know all your relevant health contraindications? Active cancer, pregnancy, thyroid history, autoimmune conditions, and current medications are the big ones. Not checking these is not a calculated risk. It is an uncalculated one.
5. Can you perform sterile injections reliably? If the honest answer is “I watched a YouTube video,” that is not sufficient preparation for a subcutaneous or intramuscular injection program. Clinical settings provide this skill as a service. If you are not in a clinical setting, you are providing it yourself, and the standard required to avoid infection complications is higher than most guides imply.
Don’t just read about your health, track it.
A single result is a snapshot. Superpower re-tests 100+ markers over time so you can watch them move as you change sleep, food, and training.
Frequently asked questions
Are peptides safe to take every day?
It depends entirely on the peptide and the form. Oral collagen peptides at 2.5 to 10 grams daily are safe for long-term daily use based on RCT data, with no serious adverse events in the clinical literature. FDA-approved prescription peptides like sermorelin are designed for regular dosing schedules under clinical supervision. Daily self-injection of research peptides without clinical oversight is a different category: the limiting factor is not the molecule’s inherent toxicity (which is largely unknown in long-term human use) but the cumulative risks of unsupervised injection, unverified purity, and the absence of monitoring to catch early adverse signals.
Are peptides safe for women?
GLP-1 receptor agonists, collagen peptides, and cosmetic copper peptide serums have been studied in mixed or predominantly female populations with no sex-specific safety signals beyond the universal contraindication for pregnancy. Growth hormone secretagogues require attention to menstrual cycle effects on GH secretion patterns. No injectable research peptide has adequate human safety data for any population, male or female.
Can peptides cause cancer?
The honest answer is “we do not know for most research peptides.” Growth hormone secretagogues chronically elevate IGF-1, which carries published epidemiological evidence of modestly increased risk for colorectal, breast, and prostate cancers. GLP-1 agents show a thyroid C-cell tumor signal in rodent studies, with no human cancer increase documented so far. Oral collagen peptides have no cancer-risk signal in 19 RCTs. Anyone considering GH-affecting peptides should have baseline IGF-1 measured and review their personal cancer history with a clinician.
Are peptides safe for people over 50?
Age-related decline in growth hormone is actually one of the clinical rationales for sermorelin in adults over 50. But age also increases baseline cancer risk, cardiovascular risk, and the likelihood of relevant comorbidities and drug interactions. This makes the “clinician-supervised” requirement more important, not less. Grey-market self-dosing carries more compounded risk in older adults than in younger, healthy individuals with no concurrent conditions.
Are peptides safe without a prescription?
The ones sold legally without a prescription, collagen supplements and topical cosmetic peptides, have excellent safety profiles. Any injectable peptide used “without a prescription” is either a prescription drug being used off-label without medical oversight, or a research chemical carrying “not for human use” labeling. Neither of those is technically “safe without a prescription” in the pharmacological sense, though the risk levels are very different.
How do I know if a peptide I am taking is causing side effects vs. something else?
This is exactly why baseline labs matter. Without a pre-treatment measurement of your IGF-1, inflammatory markers, and metabolic panel, any change in those values after starting a peptide has no reference point. This is not a philosophical argument for supervised care. It is a practical argument: if you want to know whether a peptide is working or harming you, you need data from before you started.
What is the safest peptide to start with?
Oral hydrolyzed collagen, 5 to 10 grams daily, has the most robust human safety data of any peptide category. If the goal is systemic effects such as weight loss, GH optimization, or tissue repair, a telehealth consultation to evaluate prescription-eligible options is safer than sourcing research peptides directly. Starting with a clinician is not the most exciting answer. It is the one the evidence supports.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources:
– Frontiers in Medicine 2026 meta-analysis, oral/topical peptides for skin aging, 19 RCTs / 1,341 participants
– SafeMedication: Peptide Therapy Benefits, Risks, and What You Need to Know (April 2026)
– Medical Xpress: Injectable peptides are the new anti-aging trend, evidence they’re safe for humans (April 2026)
– Nature Health 2026: Self-reported side effects of semaglutide and tirzepatide in online communities (410,000+ Reddit posts)
– FDA bulk drug substances under 503A (BPC-157 reclassification, April 2026)
– BPC-157 human clinical trials: complete status (Peptide Database, 2026)
– SURMOUNT-1 tirzepatide trial (NCT03951753)
– Grossman Wellness: Is Peptide Therapy Safe? A Physician’s Guide
– IvyRx: Sermorelin Cost and Monthly Pricing Guide (2026)
– PeakedLabs: BPC-157 Cost Guide 2026
– Finnrick independent vendor testing database
– OpenLoop Health: What Peptides Are Becoming Legal in 2026?
Want a real clinician to run the numbers, not a guess?
Joi + Blokes is a telehealth clinic that prescribes GLP-1 medication (Zepbound, compounded semaglutide and tirzepatide), hormone therapy (TRT, HRT), thyroid care, and peptides after a real lab panel and clinician review, with no membership or consult fee (prescriptions from about $59/month, lab panels from $149). If the scale will not budge, this is where you find out whether insulin, thyroid, or hormones are the real reason. Here is Joi + Blokes reviewed in full.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.