Last updated June 2026. Educational content, not medical advice. Talk to a licensed clinician before starting any supplement protocol.
Short answer: Yes, with an important asterisk. A 2026 meta-analysis of 19 randomized controlled trials covering 1,341 participants found statistically significant improvements in skin hydration (MD = 5.79, p < 0.01) and wrinkle depth after oral collagen peptide supplementation, at doses typically between 5 and 15 grams per day for 8 to 12 weeks. For joints, a September 2025 trial using 3,000 mg per day of low-molecular-weight collagen showed meaningful pain reduction and improved function over 180 days in adults with mild knee osteoarthritis. Results are real, but they are not uniform, not fast, and strongly dependent on dose, form, and whether you already eat enough protein. One caveat to hold onto from the first line: a 2025 meta-analysis in the American Journal of Medicine (Myung and Park, 23 trials) found that the studies showing benefit were largely industry-funded, while higher-quality independent trials showed no significant effect. Collagen also is not a complete protein, since it contains no tryptophan, so it does not replace your regular protein intake.
Collagen research shows real skin benefits on average. Want to see if it’s actually working for your body? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Why does this question keep coming up?
The supplement aisle has been selling collagen for a decade. Beauty influencers stir it into coffee. Athletes swear it healed a tendon injury that physical therapy alone could not crack. Then a Tufts University dermatologist publishes a review saying oral supplements are “not currently recommended to treat skin aging,” and everyone is suddenly confused about whether they wasted $40 a month.
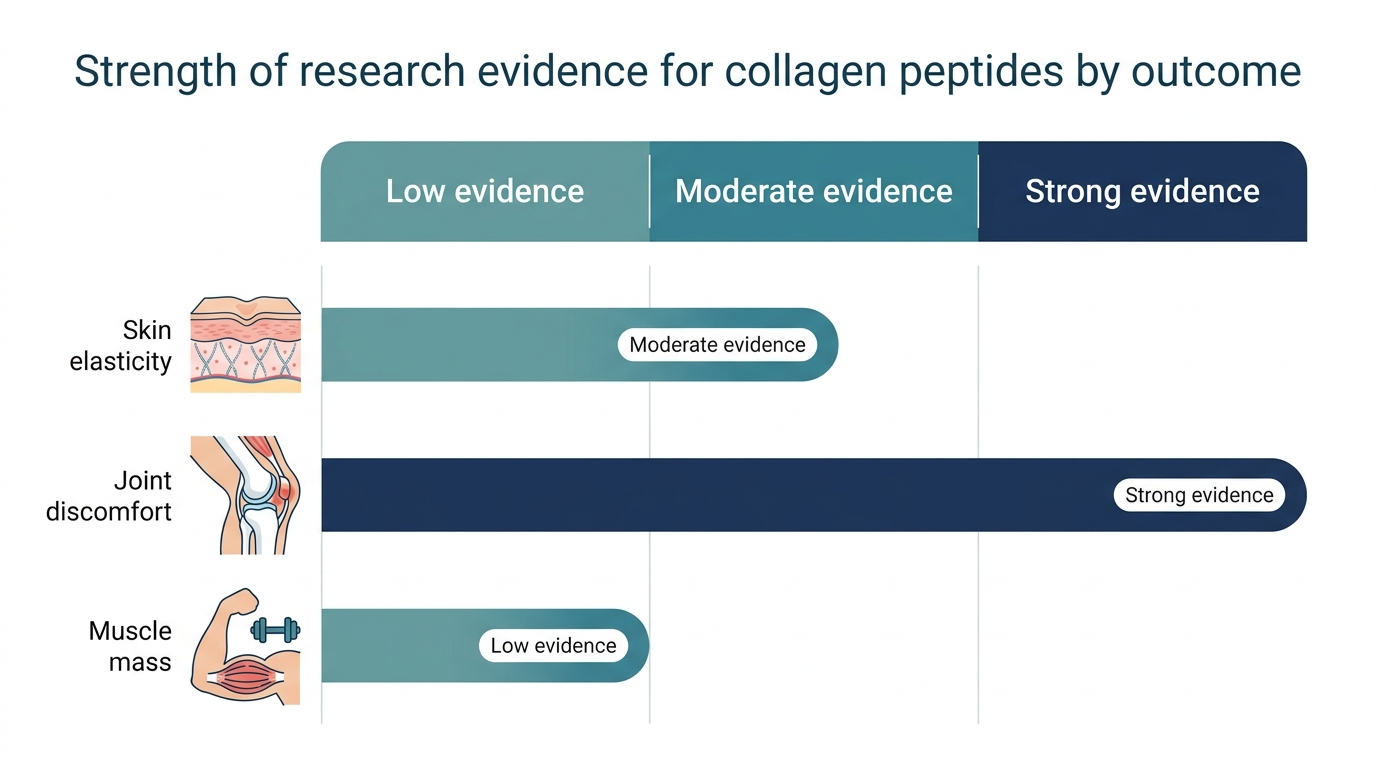
The confusion is legitimate. Collagen sits in an awkward zone between food and drug, between marketing and medicine, and the studies supporting it are unevenly distributed across outcomes. Skin research has the most trials. Tendon research is promising but thinner. Gut health research has decent mechanistic data but fewer large trials. The blanket claim “collagen works” and the blanket dismissal “it all just breaks down to amino acids” are both wrong, and both are everywhere.
What actually matters is which outcome you are after, what product and dose you use, and what the independent trials (not the ones funded by collagen brands) actually found.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
What even is a collagen peptide?
Collagen is the most abundant protein in your body, roughly 30% of total protein mass, forming the structural scaffold of skin, tendons, cartilage, bones, and the gut lining. It is a triple-helix protein built from repeating chains of amino acids, primarily glycine, proline, and hydroxyproline. That last one is unusual: hydroxyproline is almost exclusive to collagen, which is why researchers use it as a biomarker to track collagen in blood.
Collagen peptides, also called hydrolyzed collagen, are made by breaking that triple-helix structure down into shorter fragments using water and enzymes, a process called hydrolysis. The result is a soluble powder that dissolves in liquid and is digested differently from intact collagen protein.
The “hydrolyzed” part is not marketing. It is the chemical step that actually changes the bioavailability story.
Regular gelatin, like what sets in a bone broth when cooled, contains partially unwound collagen chains that still require significant digestive work before absorption. Fully hydrolyzed peptides arrive at the gut already broken into fragments small enough to be absorbed much more directly.
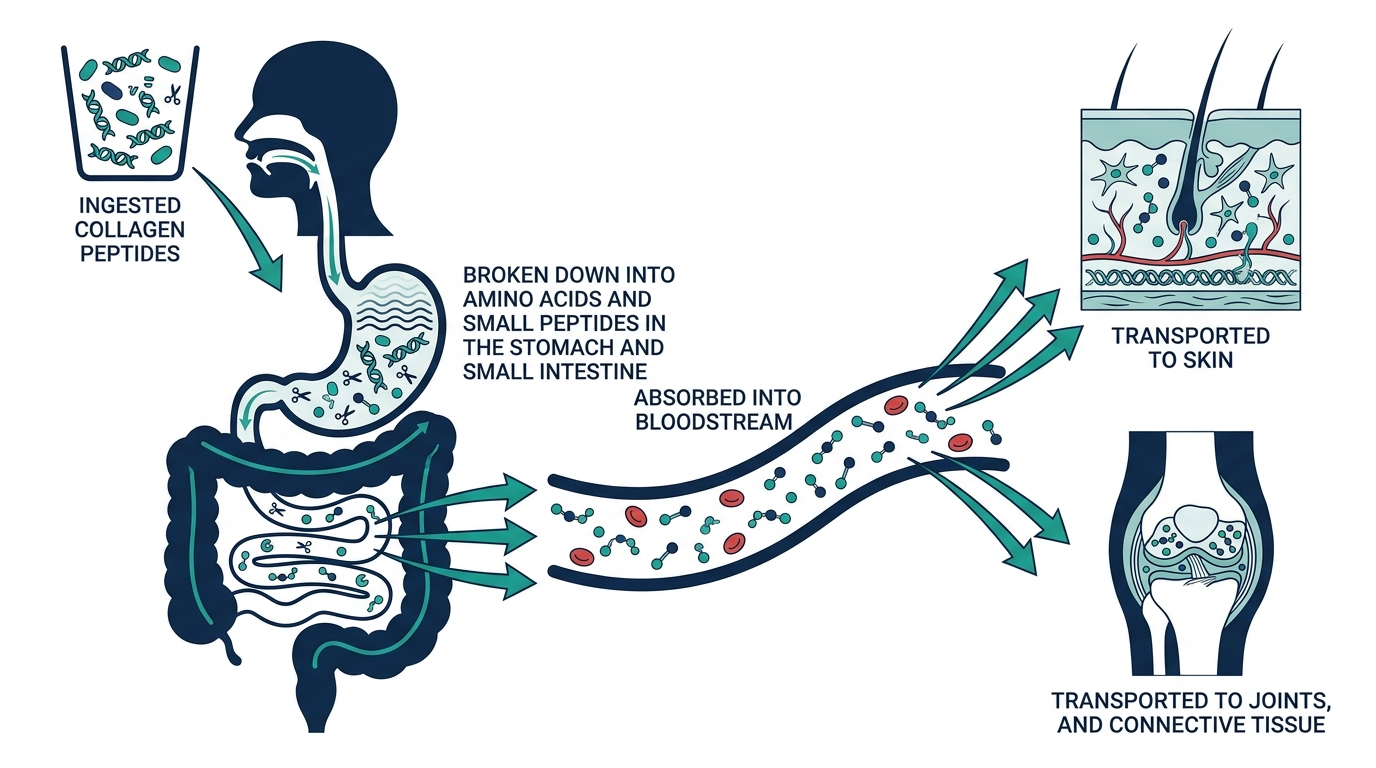
Does the body actually absorb them, or does stomach acid destroy everything?
This is the skeptic’s best argument, and for about a decade it was a fair one. The logic went: all protein is digested into individual amino acids, so eating collagen is no different from eating chicken. Your body cannot “direct” those amino acids to go rebuild skin or cartilage.
The research from 2024 to 2025 has substantially complicated that picture.
A randomized, double-blind crossover study published in Frontiers in Nutrition had participants ingest a single 10-gram dose of collagen hydrolysate from fish, porcine, or bovine sources, then tracked blood composition closely. The key finding: 36 to 47% of the absorbed hydroxyproline circulated in peptide-bound form, not as free amino acids. The most abundant peptide detected was Pro-Hyp (proline-hydroxyproline), reaching plasma concentrations of approximately 3.8 micrograms per milliliter in the porcine group. Hyp-Gly (hydroxyproline-glycine) also appeared at 0.29 to 0.76 micrograms per milliliter.
This matters because Pro-Hyp is one of the peptides that, in cell culture studies, stimulates fibroblasts to produce new collagen. The intact peptide arrives at cells as a signaling molecule, not just as raw amino acid material to be reassembled. The old dismissal assumed 100% breakdown. The actual number is closer to 53 to 64% breakdown, with meaningful fractions surviving digestion intact.
Brush border membrane enzymes in the small intestine produce the Xaa-Hyp dipeptides that are preferentially absorbed, according to a 2025 ScienceDirect study on hydroxyproline-containing peptide production. Gastroduodenal enzymes do not produce these specific fragments, which is why the hydrolysis process upstream matters.
The practical upshot: your stomach does not fully destroy collagen peptides. A meaningful fraction survives to act on tissues. How large that fraction is, and whether it is large enough to produce a measurable clinical effect, is what the trials are actually measuring.
What does the skin evidence actually show?
This is where the trial record is strongest, and where the numbers are specific enough to be useful.
A 2026 systematic review and meta-analysis in Frontiers in Medicine pooled 19 randomized controlled trials with 1,341 participants and a mean age of 50.2 years, with study durations of 4 to 12 weeks. On skin hydration, the pooled effect was statistically significant (mean difference 5.79, p < 0.01), with oral tripeptide formulations showing the strongest response (MD = 16.50). On wrinkle depth, the pooled effect was also significant (MD = 0.27, p = 0.04). Skin elasticity and density did not reach statistical significance in the pooled analysis, though individual trials did show effects.
A specific 12-week double-blind, placebo-controlled trial using low-molecular-weight collagen peptides found skin hydration increased by 13.8%, the elasticity index increased by 22.7%, and wrinkle measurements decreased by 19.6% versus placebo. A confocal microscopy analysis in a separate trial observed a 44.6% decrease in collagen fragmentation versus placebo after 12 weeks.
Here is the nuance the headline numbers miss, and it is a large one. A 2025 meta-analysis in the American Journal of Medicine (Myung and Park) pooled 23 trials and found that when researchers separated the studies by funding source and quality, the picture changed sharply: industry-funded trials showed benefit, but non-industry-funded trials and the higher-quality studies showed no significant improvement in hydration, elasticity, or wrinkles. A January 2026 review from Tufts University dermatologist Dr. Farah Moustafa reached the same conclusion and went further, stating that oral collagen supplements are “not currently recommended to treat skin aging.” She also pointed out that marine-sourced collagen carries a methylmercury contamination risk, and that the FDA does not check supplements for safety or effectiveness before they reach market.
Both of these things can be simultaneously true: some pooled analyses report real effects, and the quality of that evidence is uneven enough that confident conclusions are not yet justified. The honest read is that oral collagen peptides may produce modest improvements in skin hydration and wrinkle depth, most plausibly in women over 40, but the benefit shrinks or disappears once you weight for study quality and funding. Treat it as a low-risk supplement that might help at the margins, not a proven anti-aging treatment. If you want a structured look at specific products and how they stack up, our best collagen peptides guide breaks down the formulations.
Personally, I find the hydration data more convincing than the elasticity data. Hydration shows up across more independent trials with less heterogeneity. The elasticity claims in marketing copy routinely outrun what the studies actually found.
What about joints?
Skeptics sometimes dismiss the joint evidence entirely, treating it as marketing dressed up as science. That is no longer accurate.
A September 2025 randomized, double-blind, placebo-controlled trial published in Frontiers in Nutrition tested 3,000 mg per day of low-molecular-weight collagen peptides in adults with mild knee osteoarthritis over 180 days. The result: significant improvements in both pain and physical function, with no adverse events reported. The 180-day duration is notable because most skin studies run 12 weeks, and joints respond more slowly.
A separate trial using 10 grams per day of CollaSel PRO (Type I and Type III hydrolyzed collagen) ran 8 weeks in 160 adults with osteoarthritis and found meaningful reductions in joint pain and stiffness compared to placebo.
The tendon story is where things get particularly interesting for athletes. A 2025 systematic review with meta-analysis found GRADE A evidence for increases in tendon cross-sectional area and stiffness with collagen supplementation at 15 to 30 grams per day combined with resistance training. The key detail the gym community often gets right but for the wrong reason: timing matters. A landmark study from Keith Baar’s group at UC Davis showed that subjects who took 15 grams of vitamin C-enriched gelatin one hour before exercise doubled the aminoterminal propeptide of collagen I in blood compared to placebo, indicating significantly elevated collagen synthesis. The vitamin C is not decoration. It is required for the hydroxylation step that stabilizes the collagen triple helix.
Do not believe any protocol for tendon repair that skips the vitamin C and the pre-exercise timing. The molecule alone, taken randomly throughout the day, is likely far less effective.
What about nails and hair?
This is where marketing runs furthest ahead of the data. The most cited nails study is a small 2017 trial: 25 people with brittle nails took 2.5 grams of collagen daily for 24 weeks and saw improved growth and less brittleness. The problem is that it had no placebo group, so it cannot rule out the natural improvement that often happens just from people paying attention to their nails.
Hair is weaker still. Most of the apparent hair benefits in the literature come from products that combine collagen with other micronutrients and antioxidants, which makes it impossible to credit the collagen specifically. There is mechanistic and animal work suggesting low-molecular-weight collagen peptides may signal hair follicles, but the human RCT evidence is mixed and thin. If glossy nails and thicker hair are your only reason for buying collagen, the honest answer is that the evidence does not yet support that expectation.
Does it help with gut health?
The gut health angle is the youngest of the three major claims, and it has the thinnest trial record, though the mechanistic evidence is sound.
Collagen is a major structural component of the gut’s extracellular matrix, and the intestinal wall depends on Type I and Type III collagen for integrity. The amino acids most abundant in collagen, especially glycine and proline, play direct roles in maintaining tight junction proteins that control what crosses the intestinal wall. Glycine in particular has demonstrated anti-inflammatory effects on gut epithelial cells across multiple studies.
A study in Nutrients found that collagen peptide supplementation was associated with significant reductions in zonulin levels, a biomarker of intestinal permeability, in adults with gut dysfunction. The effect was meaningful but the trial was small, and larger, independent studies are still needed before gut health becomes a primary evidence-based reason to supplement with collagen.
The practical position: if you are already taking collagen for skin or joint reasons, there is plausible mechanistic support for secondary gut benefits. Buying collagen specifically to fix leaky gut is ahead of the trial evidence.
Type I vs. Type II vs. Type III: does it actually matter which you buy?
Yes, more than the marketing copy usually explains.
Type I collagen is the most abundant in the body and forms the structural backbone of skin, tendons, bones, and ligaments. It is the default form in most bovine and marine collagen supplements. Vital Proteins’ standard collagen peptides, for example, are Type I and II from bovine hide.
Type II collagen is the dominant form in cartilage. It is found in chicken sternum and is typically sold in a different form (undenatured Type II, or UC-II) at a much lower dose (40 mg versus 10 to 15 grams). The mechanism is different: UC-II works through oral tolerance, a process where small amounts of intact Type II trigger an immune response that reduces cartilage breakdown. It is not interchangeable with hydrolyzed Type I, and the dosing is completely different.
Type III collagen often appears alongside Type I and is found in soft tissue, blood vessels, and the gut wall.
The practical consequence: if your primary interest is skin and tendons, a standard bovine or marine hydrolyzed collagen (Type I, 10 to 15 g per day) is well-matched to your goal. If your primary concern is cartilage specifically, undenatured Type II at 40 mg per day has a separate trial track record and operates through a different mechanism. Mixing them into one product rarely optimizes either.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
How to compare collagen products without getting misled
A few things the ingredient list will not tell you, but matter:
Source and processing. Bovine hide (skin), bovine joint, marine (fish skin), and chicken sternum produce different collagen types and molecular weight profiles. Wild-caught marine collagen tends to have a lower average molecular weight and may have superior bioavailability to bovine, according to some studies, but the practical difference in outcomes has not been definitively established at matched doses.
Molecular weight. Fully hydrolyzed collagen peptides typically run between 2,000 and 5,000 Daltons. Some products are marketed as “low-molecular-weight” at under 2,000 Da (often called collagen tripeptides). The 2026 Frontiers in Medicine meta-analysis found tripeptide formulations showed the strongest hydration effect (MD = 16.50 versus 5.79 overall), suggesting that smaller fragments may have an edge for skin outcomes.
Third-party testing. Unlike pharmaceutical drugs, collagen supplements are not verified by the FDA before sale. Third-party certification programs like NSF International, Informed Sport, and USP confirm that what is on the label is actually in the bottle and that it is free from common contaminants.
Actual cost per gram of collagen. The range in 2026 runs from roughly $0.08 per gram (Orgain, basic formulations) to over $0.13 per gram for premium or certified brands. At a 10-gram daily dose, that is $0.80 to $1.30 per day, or roughly $24 to $40 per month. Price alone does not predict quality, but suspiciously cheap products are more likely to skip third-party testing.
The myth this category is built on
Here is the one claim that collagen marketing repeats constantly and that the biology does not support: the idea that eating collagen sends collagen directly to your skin or joints.
It does not. The body cannot route absorbed peptides or amino acids to specific tissues on demand. What the evidence does support is a different mechanism: some intact Pro-Hyp peptides act as signaling molecules that stimulate fibroblasts to produce more of their own collagen. You are not “feeding” your skin collagen. You are providing a molecular signal that tells skin cells to ramp up their own synthesis.
This distinction matters for expectation-setting. The benefit is indirect, time-lagged (weeks, not days), and depends on your body having adequate vitamin C and the underlying cellular machinery to respond to that signal. Someone who is severely protein-deficient, vitamin C-depleted, or has advanced fibroblast dysfunction from chronic UV damage will likely respond differently than a healthy 45-year-old with otherwise good nutrition.
It also means the “you can just eat chicken instead” argument is not completely right either. Chicken does not deliver intact Pro-Hyp dipeptides in the same concentration as a 10-gram dose of hydrolyzed collagen, because the hydroxyproline content in most muscle meat is low compared to collagen-rich tissue like skin, tendons, and bone. Bone broth is the nearest food equivalent, providing 6 to 12 grams of collagen per cup, but the degree of hydrolysis in broth is lower and more variable than a standardized supplement.
One more thing the marketing rarely mentions: collagen is not a complete protein. It contains no tryptophan and is low in several other essential amino acids, which gives it a protein quality score (PDCAAS) of effectively zero. That does not make it useless, but it means the grams of collagen on the label should not be counted toward your daily protein target the way whey or meat would be. Collagen is a targeted supplement, not a protein source.
What I would actually do
Personally, if I were starting with collagen, I would choose a bovine or marine hydrolyzed collagen with third-party certification (NSF or USP), 10 grams per day for skin purposes or 3 to 10 grams combined with exercise for tendon and joint purposes. I would take it with 50 to 100 mg of vitamin C, ideally 30 to 60 minutes before a workout if joint or tendon health is the goal. I would give it 8 to 12 weeks before evaluating, because the skin trial evidence is consistently at 8 to 12 weeks. And I would expect hydration and texture improvement over elasticity gains, because that is where the independent evidence is stronger.
I would not expect it to reverse significant skin aging on its own, and I would stack it alongside proven interventions: sunscreen daily, adequate total dietary protein (0.7 to 1 gram per pound of body weight), and topical retinoids if dermatologist-approved. Collagen is additive to those foundations, not a replacement for them. If you are evaluating where collagen fits among other evidence-graded options, our best longevity supplements guide ranks the categories worth your money against the ones that are mostly hype.
Turn what you just learned into action.
Superpower lets you test 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
Do collagen peptides actually work for wrinkles?
Yes, modestly. A 2026 meta-analysis of 19 RCTs (1,341 participants) found statistically significant wrinkle reduction with oral collagen supplementation. The effect is real but not dramatic, most consistent after 8 to 12 weeks at 5 to 15 grams per day, and strongest in women over 40. Do not expect results comparable to topical retinoids.
How long does it take for collagen peptides to work?
Most skin trials run 8 to 12 weeks before measuring outcomes. Joint and tendon studies typically run 12 to 26 weeks. Expect to give any collagen protocol at least 10 to 12 weeks before drawing conclusions.
How much collagen peptide should I take per day?
The research-backed range is 5 to 15 grams per day for skin and general use, and 3 to 10 grams per day for joints and tendons (combined with exercise). For tendon repair specifically, a pre-exercise dose 30 to 60 minutes before training appears to amplify collagen synthesis more than taking the same dose at rest.
Does it matter if I take bovine or marine collagen?
Bovine (from cattle hide) is Type I, widely studied, and typically the least expensive. Marine (from fish skin) is also primarily Type I, potentially slightly higher bioavailability due to lower average molecular weight, and carries a small methylmercury risk with cheap brands. For most people, a tested bovine product is fine. If you prefer marine, choose a brand with third-party heavy metal testing.
Can I get the same benefit from bone broth?
Partially. Bone broth provides 6 to 12 grams of collagen per cup, along with minerals and glycosaminoglycans. However, the degree of hydrolysis is lower and more variable, meaning fewer intact Pro-Hyp dipeptides reach the bloodstream compared to a standardized hydrolyzed supplement. Bone broth is a good food for collagen-supportive amino acids. It is not an equivalent swap for a clinical-grade hydrolyzed product if the goal is a specific outcome like skin hydration.
Is vitamin C necessary with collagen peptides?
Not strictly for absorption, but yes for synthesis. Vitamin C is a required cofactor for prolyl hydroxylase, the enzyme that creates hydroxyproline and stabilizes the collagen triple helix. The UC Davis study showed a doubling of collagen synthesis markers when vitamin C-enriched gelatin was taken before exercise. Including even 50 mg of vitamin C with your collagen dose is supported by the mechanistic and clinical evidence.
Are collagen peptides safe?
Yes, in the doses used in research. The 2026 meta-analysis reported only mild gastrointestinal discomfort in a small number of participants. The main practical risks are methylmercury from low-quality marine sources and the absence of third-party quality testing in an unregulated supplement market.
Reviewed by the Vital Signs Today Editorial Board. Educational content, not medical advice. Sources linked inline.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
Primary sources:
- Frontiers in Medicine 2026 systematic review and meta-analysis (19 RCTs, 1,341 participants): https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2026.1618306/full
- Frontiers in Nutrition 2025 knee osteoarthritis RCT (3,000 mg LMCP, 180 days): https://www.frontiersin.org/journals/nutrition/articles/10.3389/fnut.2025.1644899/full
- PMC 2024 bioavailability crossover study (Pro-Hyp plasma detection): https://pmc.ncbi.nlm.nih.gov/articles/PMC11325589/
- Wiley 2025 sustained effects of BCP RCT: https://onlinelibrary.wiley.com/doi/10.1111/jocd.70565
- PMC 2024 12-week hydrolyzed collagen trial (skin collagen, hydration, elasticity, hair): https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11254459/
- PMC 2025 tendon meta-analysis (GRADE A evidence, 15-30 g + resistance training): https://pmc.ncbi.nlm.nih.gov/articles/PMC11561013/
- PMC 2017 vitamin C-enriched gelatin pre-exercise (Keith Baar, UC Davis): https://pmc.ncbi.nlm.nih.gov/articles/PMC5183725/
- ScienceDaily January 2026 Tufts University dermatologist review: https://www.sciencedaily.com/releases/2026/01/260129080443.htm
- ScienceDirect 2025 brush border membrane enzyme production of Hyp-containing peptides: https://www.sciencedirect.com/science/article/abs/pii/S0963996925011858
- Superpower.com collagen vs. bone broth comparison: https://superpower.com/guides/collagen-bone-broth
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.