Last updated 18 June 2026. Educational content, not medical advice. Peptide regulations are actively shifting in 2026; verify current status with a licensed clinician or pharmacist before making any purchase decision.
Short answer: Most peptides are legal to buy in the US in some form, but the form matters enormously. FDA-approved peptide drugs like semaglutide (Ozempic) and tirzepatide (Mounjaro) are fully legal with a prescription. Collagen peptides are legal over the counter as supplements. Injectable “research use only” peptides like BPC-157 and TB-500 exist in a grey zone where selling them is technically legal and injecting them yourself is not, though individual buyers rarely face prosecution. On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. announced that 14 of 19 restricted peptides are expected to be moved back into legal compounding access, with a critical FDA committee vote scheduled for July 23 to 24, 2026.
Peptide legality keeps shifting in 2026, but your bloodwork is one thing you can check right now, legally, at home. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Why is the question “are peptides legal” so hard to answer?
Because the word “peptide” covers an enormous range of molecules, and the US regulatory system treats them through four completely different frameworks simultaneously. A collagen hydrolysate in your morning smoothie, the semaglutide in a Wegovy pen, and a vial of BPC-157 powder from a research vendor are all technically “peptides.” They share almost nothing else about their legal situation.
Regulatory confusion is not an accident here. The grey-market research peptide industry was built on that confusion, using a single word to blur the line between a breakfast supplement and an unapproved injectable drug. Getting the legal picture right requires separating four distinct categories that the marketing deliberately mixes together.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
What are the four legal lanes for peptides in the US?
The simplest way to actually get this done
Superpower is a full-body lab membership that runs 100+ biomarkers, has each result reviewed by a doctor, and tracks your numbers year over year (about $199/year). It is what we point readers to when they would rather get one clean, complete draw than chase single tests one at a time. Here is superpower reviewed in full.
Understanding legality requires sorting every peptide purchase into one of these four frameworks. The problems start when someone mistakes Lane 3 for Lane 1.
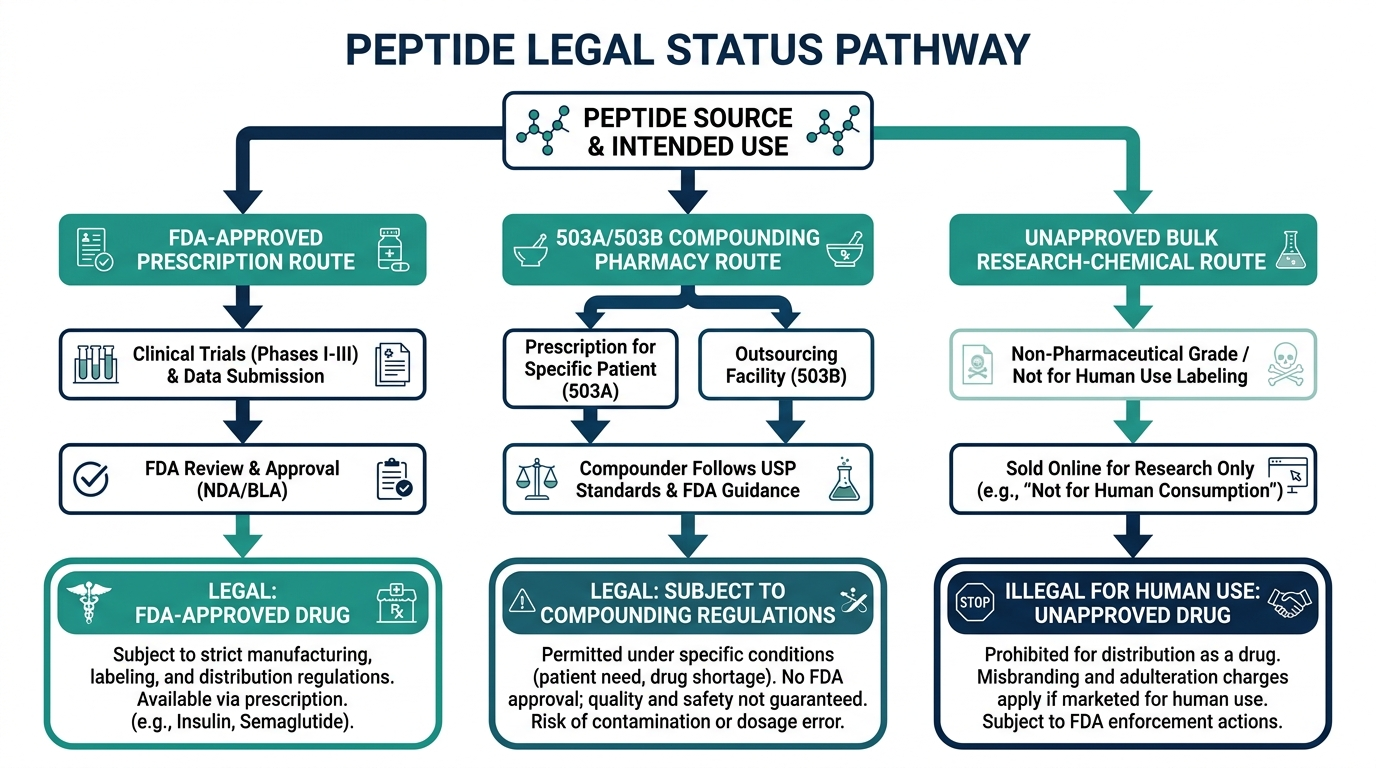
Lane 1: FDA-approved prescription drugs. GLP-1 peptides like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) are fully approved drugs. So are sermorelin and tesamorelin for specific medical indications, as well as insulin, oxytocin, and a handful of others. These are legal with a valid prescription from a licensed clinician, dispensed through a licensed pharmacy. There is no grey zone here.
Lane 2: Compounded peptides through licensed pharmacies. Licensed 503A compounding pharmacies can legally prepare specific peptides for individual patients with a prescription, as long as the substance appears on the FDA’s permitted bulk drug substance list (Category 1). This lane nearly collapsed in 2023 when the FDA moved 19 peptides to Category 2 (substances that “may present significant safety risks”), banning them from compounding. It is now reopening.
Lane 3: Collagen peptides and cosmetic topicals. Hydrolyzed collagen is Generally Recognized as Safe (GRAS) under 21 CFR 184.1553 and is sold as a dietary supplement without a prescription. Topical copper peptide (GHK-Cu) serums are regulated as cosmetics as long as they do not make drug claims. These are fully legal over the counter, widely available, and in an entirely different risk class from injectable research peptides.
Lane 4: “Research use only” peptides. This is the grey market. Vendors sell peptides like BPC-157, TB-500, CJC-1295, Ipamorelin, and retatrutide with a “for laboratory research only, not for human use” disclaimer. Selling them with that label is technically legal. Using them on yourself is not within that label’s protection, and the FDA presumes any peptide shipped to a residential address with no institutional affiliation is intended for human use, regardless of what the label says. Enforcement targets sellers, not buyers, but the “research use only” model is under serious federal pressure in 2026.
| Lane | Examples | Prescription needed? | Legal to inject? | OTC available? |
|---|---|---|---|---|
| FDA-approved drugs | Semaglutide, tirzepatide, sermorelin | Yes | Yes, if prescribed | No |
| Compounded pharmacy | BPC-157 (pending), CJC-1295 (pending) | Yes | Yes, if compounded legally | No |
| Supplements / cosmetics | Collagen peptides, GHK-Cu topicals | No | N/A (oral/topical) | Yes |
| Research use only | TB-500, retatrutide, melanotan | No (but illegal to self-inject) | Not legally | Grey market only |
What exactly did RFK Jr. change for peptides in 2026?
On February 27, 2026, HHS Secretary Robert F. Kennedy Jr. announced on the Joe Rogan Experience that roughly 14 of the 19 peptides the FDA had placed on the Category 2 restricted list in 2023 would be moved back to Category 1, reopening the legal compounding pathway through licensed pharmacies (Meto Health).
The announcement made headlines in the peptide community. The reality of what it actually changed is more nuanced, and most coverage has not been careful about the distinction.
Here is what the announcement did NOT do: it did not legalize any peptide, it did not constitute formal FDA rulemaking, and it did not immediately allow any compounding pharmacy to start dispensing BPC-157 or TB-500. RFK’s statement was an intent signal, not a regulatory action.
What it did do was initiate a review process that matters. The FDA removed BPC-157 (both acetate and free base forms) from Category 2 on April 22, 2026, returning it to an evaluative state. The Pharmacy Compounding Advisory Committee (PCAC) is scheduled to meet on July 23 to 24, 2026 at FDA’s White Oak Campus in Silver Spring, Maryland, to formally review seven peptides: BPC-157, KPV, TB-500, and MOTs-C on Day 1; Emideltide (DSIP), Semax, and Epitalon on Day 2 (FDA docket FDA-2025-N-6895). Public comment closed July 22, 2026.
Even a favorable PCAC vote does not add a substance to the 503A Bulks List immediately. That requires formal FDA rulemaking that occurs after the committee meeting, meaning a compounding pharmacy cannot legally prepare BPC-157 from the PCAC vote alone. A pharmacist or telehealth platform advertising injectable BPC-157 as fully legal today is running ahead of where the regulations actually sit.
The full list of 14 peptides RFK identified as candidates for reclassification includes BPC-157, Thymosin Alpha-1, TB-500, GHK-Cu, AOD-9604, MOTS-C, KPV, Semax, Selank, Kisspeptin-10, Epitalon, Emideltide/DSIP, CJC-1295, and Ipamorelin (Meto Health). Not all of them are through the PCAC process yet.
How did the FDA enforcement crackdown change what you can actually buy?
The shift from lenient oversight to active enforcement between late 2024 and mid-2026 removed a significant portion of the research peptide market and changed the risk profile for what remains.
The enforcement timeline runs roughly as follows. In December 2024, the FDA issued its first wave of warning letters to grey-market peptide vendors, signaling a shift from looking away to active enforcement. In June 2025, federal agents raided the warehouse of Amino Asylum, one of the largest research-chemical sellers, taking it offline overnight. By September 2025, more than 50 warning letters had gone out simultaneously to vendors, compounding pharmacies, and telehealth platforms. Later in 2025, the DOJ secured guilty pleas in cases involving illegal peptide distribution, moving the enforcement ceiling from civil penalty to federal crime.
The most significant criminal case involved Tailor Made Compounding LLC, which pleaded guilty to introducing unapproved new drugs into interstate commerce, including BPC-157 distribution, and was forced to forfeit $1.79 million (AMC Defense Law). That case established that a compounding pharmacy shipping BPC-157 cannot escape federal prosecution by arguing grey-zone status.
Peptide Sciences, for years the most-referenced vendor in online forums, voluntarily closed all operations on March 6, 2026, with no advance notice and no refund process for outstanding orders (The Peptide Catalog). Science.bio had done nearly the same thing two months earlier. The research peptide industry lost more vendors between mid-2025 and early 2026 than in the previous five years combined.
Do not believe anyone who tells you this crackdown was only about bad actors. The FDA also began using AI to scrape vendor websites for dosing information that contradicted “research use only” disclaimers. The model for identifying targets shifted from complaint-driven to proactive, which means the vendors who survived the cull are still operating in an enforcement environment that is actively scanning them.
Are “research use only” peptides actually legal to buy?
This is the most misunderstood question in the whole space, and the answer requires separating two different acts.
Purchasing a “research use only” peptide vial from a US-based vendor is technically legal for the buyer. The vendor is legally selling a research chemical. You are legally buying one. Nothing about that transaction puts you in legal jeopardy on purchase.
The moment you draw the peptide into a syringe and administer it to yourself, you have left the legal fiction of “research use only” behind. The label was never a shield for self-administration; it was a shield for the vendor. Federal law requires that drugs administered to humans be FDA-approved (or compounded through licensed channels with a prescription). No exemption exists for self-experimentation.
Personally, I think the “research use only” framing is one of the more cynical constructs in the supplement industry. The vendors know their customers are injecting. Their customers know the vendors know. The label exists solely to transfer legal liability from seller to buyer, not to accurately describe the actual transaction. A first-year law student could see through it.
The practical prosecution picture for individual buyers is less severe. Federal authorities have focused enforcement on commercial sellers, distributors, and compounding pharmacies rather than individual users. Buying one vial of BPC-157 for personal use does not appear to have resulted in individual prosecution. The risk remains concentrated on the supply side. But that risk profile can shift as enforcement matures, and it provides zero protection against the actual risk, which is not legal prosecution but the quality, purity, and identity of what is in the vial.
What about GLP-1 peptides? Is compounded semaglutide still legal?
This lane closed faster than most buyers realized. The FDA declared tirzepatide’s drug shortage resolved on October 2, 2024, and semaglutide’s shortage resolved on February 21, 2025 (FDA). Once a shortage resolves, compounding pharmacies lose the legal basis to produce copies of the branded drugs.
The enforcement discretion periods gave pharmacies time to wind down: 503A pharmacies had until April 22, 2025 for semaglutide and February 19, 2025 for tirzepatide. 503B outsourcing facilities had until May 22, 2025 for semaglutide. Courts denied preliminary injunctions filed by the Outsourcing Facilities Association; the deadlines held. The window for compounded GLP-1s at $99 to $149 a month is effectively closed as of mid-2026.
Semaglutide and tirzepatide remain fully legal through the branded prescription route (Ozempic, Wegovy, Mounjaro, Zepbound). The SURMOUNT-1 trial established tirzepatide’s mean body-weight reduction at 22.5% over 72 weeks, which is why the demand never went away. Telehealth providers like Hone Health, Defy Medical, and Ro can prescribe branded GLP-1s after a clinical intake, though the cost without insurance is substantially higher than the compounded alternatives were.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Which peptides can you legally buy without a prescription right now?
Three categories are genuinely accessible without a prescription, but they cover very different territory than most “are peptides legal” searches are actually asking about.
Collagen peptides (hydrolyzed collagen): Fully legal dietary supplements. Widely available at major retailers, from grocery stores to Amazon. The FDA classifies hydrolyzed collagen under GRAS status and dietary supplement regulations. Research on collagen supplementation includes a clinical trial (NCT07302789, active on ClinicalTrials.gov as of June 2026) examining two oral bioactive collagen peptides on skin aging hallmarks. There is no prescription needed and no meaningful legal question here.
Topical copper peptide (GHK-Cu) products: Sold as cosmetics, regulated under the FD&C Act’s cosmetic provisions. Dozens of skincare brands sell GHK-Cu serums legally. The legal boundary is the drug claim. A serum that says “reduces wrinkles” is a cosmetic claim; a serum that says “repairs damaged tissue” is a drug claim and puts the product outside cosmetic regulation.
Certain topical peptides in skincare (Argireline, Matrixyl, Leuphasyl, etc.): These signal molecules are marketed as cosmetics globally and sold without restriction. They work at the topical level and have never been subject to FDA compounding restrictions.
What is not available OTC legally: injectable therapeutic peptides, GH secretagogues, healing peptides, metabolic peptides, or any peptide that requires reconstitution from a lyophilized powder. Any website selling those “no prescription needed, for human use” is operating outside the rules. The label “no prescription needed” on an injectable peptide is a regulatory violation, not a convenience feature.
What does the legal route actually cost?
Pricing in 2026 splits cleanly by lane, and the cheap option almost always reflects the absence of something you actually want.
| Source | Peptide | Monthly cost | What is included |
|---|---|---|---|
| Retail / OTC | Collagen peptides | $20 to $60 | Just the product, reputable brands |
| Grey-market vendor | BPC-157, TB-500 (research) | $40 to $120 per vial | Molecule only, no oversight, no supplies |
| Telehealth clinic | Sermorelin | $175 to $225/mo (IvyRx) | Consult, prescription, compounded pharmacy |
| Telehealth clinic | BPC-157 or peptide therapy | $199 to $425/mo (PeakedLabs) | Full program, labs, monitoring |
| In-person clinic | BPC-157 single cycle | $445+ per cycle (PerfectB) | In-person clinical oversight |
| Branded prescription | Semaglutide (Wegovy) | $1,000 to $1,350/mo without insurance | Approved drug, no compounding |
One number worth noting: sermorelin at $175 to $225 a month through a telehealth clinic costs roughly one-fifth of what synthetic HGH used to cost at $600 to $1,200 a month. The licensed route is meaningfully cheaper than the alternatives it replaced for growth hormone support.
None of the prescription or clinic options are covered by standard insurance when prescribed for longevity, recovery, or optimization. Budget accordingly before the first invoice.
Is it legal to import peptides from overseas?
Importing unapproved drugs for personal use exists in a murky space. The FDA has a longstanding policy of personal importation discretion, generally allowing individuals to import up to a 90-day supply of a drug for personal use if no domestic equivalent is available and there is no unreasonable risk to health. This policy has never been extended in any clear form to injectable research peptides.
Practically: US Customs has seized peptide shipments from overseas vendors. Foreign peptide vendors offer zero quality assurance, no regulatory accountability, and no recourse if the product is contaminated or mislabeled. The independent testing platform Finnrick has documented purity failures even among domestic vendors with strong reputations, and international products carry additional risk from uncontrolled cold chains (many peptides degrade rapidly outside refrigeration).
There is no safe lane for importing injectable research peptides from overseas. The risk is not primarily legal, it is biological.
Myth-busting: five things the peptide internet gets wrong about legality
Myth 1: “Research use only” means it is legal to use on yourself. No. It means the vendor is legally allowed to sell it as a research chemical. The label transfers legal risk to you, not away from it. The FDA presumes intent to inject based on shipping address and context, regardless of the label.
Myth 2: RFK Jr. made peptides legal in 2026. His February 27 announcement was an intent signal. No peptides have been formally reclassified to Category 1 as of June 2026. The PCAC vote in July 2026 is a necessary step, but formal rulemaking comes after that.
Myth 3: If a telehealth clinic is selling it, it must be legal. Not necessarily. Some telehealth platforms sourced from grey-market suppliers and dressed it up with a clinical interface. A legitimate telehealth provider names its compounding pharmacy (licensed 503A or 503B), requires lab work before prescribing, and only prescribes substances that are currently permitted for compounding. If a site offers injectable BPC-157 or TB-500 today without acknowledging the PCAC review, it is worth asking exactly which pharmacy is filling it and under what authority.
Myth 4: Collagen peptides are in the same regulatory category as injectable peptides. Completely false. Hydrolyzed collagen is GRAS as a food ingredient, sold as a dietary supplement under DSHEA. Injectable GH secretagogues are unapproved drugs. Calling both “peptides” does not make their legal situation similar.
Myth 5: Buying peptides is as risky as selling them. Federal enforcement in 2025 to 2026 has focused almost exclusively on commercial sellers, distributors, and compounding pharmacies. Individual buyers purchasing small quantities for personal use have not been the prosecution targets. That said, the product risk (purity, identity, sterility, dose accuracy) falls entirely on the individual buyer once the vendor’s accountability ends at shipment.
What is the smartest move given where regulations are right now?
The July 2026 PCAC meeting is a genuine inflection point. If the committee votes favorably on BPC-157 and the other six peptides under review, formal rulemaking will follow, which would eventually allow licensed compounding pharmacies to legally prepare them for patients with prescriptions. That would be the end of any meaningful case for using grey-market vendors for those compounds.
Personally, given where the regulations sit in June 2026, the highest-leverage thing someone can do is work with a legitimate telehealth clinic for the peptides currently available on prescription (sermorelin, tesamorelin, NAD+, and GLP-1s) and wait for the formal compounding pathway to open for BPC-157 and similar compounds. Paying a grey-market vendor now for something that may be legally available through a licensed pharmacy in 6 to 12 months means paying for the grey zone twice.
The legal route and the effective route are converging. The gap between them is shrinking by quarter, and the sticker price is almost the only thing holding the grey market together now.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Are peptides legal in the US in 2026?
It depends on the peptide and its form. FDA-approved peptide drugs (semaglutide, tirzepatide, sermorelin) are legal with a prescription. Collagen peptides are legal OTC as supplements. Injectable research peptides like BPC-157 and TB-500 occupy a grey zone: legal to sell as research chemicals, not legal to self-inject, and subject to an evolving regulatory review. A PCAC committee meeting on July 23 to 24, 2026 will review seven peptides for potential return to legal compounding status.
Did RFK Jr. make BPC-157 legal in 2026?
Not yet, technically. On February 27, 2026, HHS Secretary Kennedy announced his intent to move 14 peptides from the FDA’s restricted Category 2 list back to Category 1. The FDA removed BPC-157 from Category 2 on April 22, 2026, and scheduled a PCAC review for July 23 to 24, 2026. Formal addition to the 503A Bulks List requires rulemaking after the committee vote. As of June 2026, BPC-157 is not yet legal for pharmacy compounding.
Can you buy peptides over the counter?
Collagen peptides and topical skincare peptides (copper peptides, Argireline, Matrixyl) are legally sold OTC as supplements and cosmetics. Injectable therapeutic peptides and research peptides are not legitimate OTC products. Any vendor selling injectable peptides “no prescription needed, for human use” is operating outside FDA rules.
Is it legal to buy research peptides online in the US?
Purchasing “research use only” peptides from a US vendor is not a federal crime for the buyer in the current enforcement environment. Enforcement targets sellers, not individual buyers. However, self-administering a research peptide is outside what the “research use only” label protects, and the product quality risk (purity, identity, sterility) is entirely yours. Vendors like Amino Asylum have been raided and closed with no notice or refunds.
What peptides are becoming legal through compounding in 2026?
The 14 peptides RFK Jr. identified as candidates for reclassification include BPC-157, Thymosin Alpha-1, TB-500, GHK-Cu injectable, AOD-9604, MOTS-C, KPV, Semax, Selank, Kisspeptin-10, Epitalon, Emideltide/DSIP, CJC-1295, and Ipamorelin. The July 23 to 24, 2026 PCAC meeting reviews BPC-157, KPV, TB-500, MOTS-C, Emideltide, Semax, and Epitalon. Formal rulemaking follows the committee vote.
What is the difference between Category 1 and Category 2 peptides?
Under FDA’s 503A compounding framework, Category 1 substances are permitted for use in compounding by licensed pharmacies with a prescription. Category 2 substances “may present significant safety risks” and are banned from compounding. In 2023, the FDA placed 19 peptides on Category 2, effectively shutting the legal compounding route. The 2026 reclassification effort aims to move most of those back to Category 1, restoring the legal pathway through licensed pharmacies.
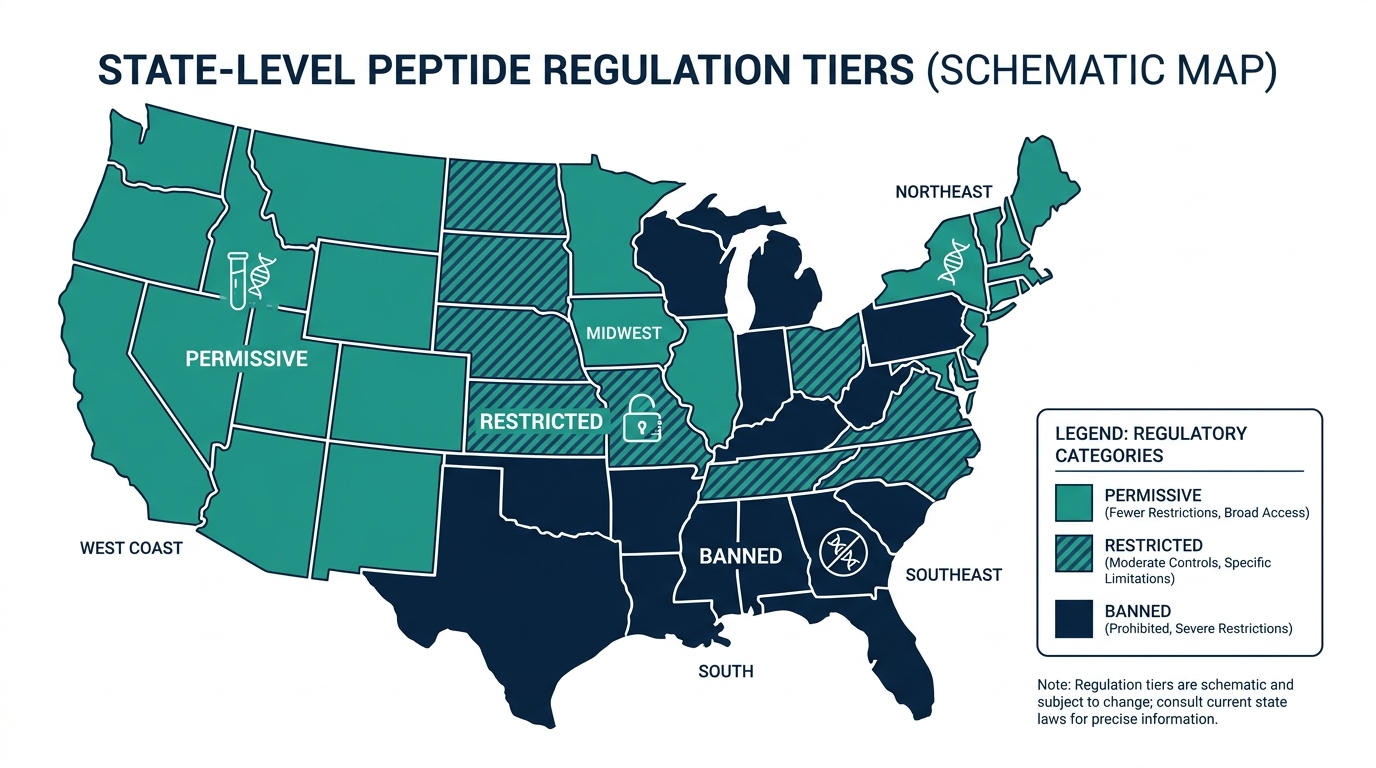
Are peptides legal in every state?
Federal law governs the prescription drug and compounding framework, but states can add restrictions. State pharmacy boards regulate which compounding pharmacies operate in-state. Some states have additional requirements for out-of-state compounded drugs. For research peptide vendors, state law adds another layer that rarely favors the buyer. For practical purposes, if it is not legal at the federal level, state permissiveness does not provide meaningful cover.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources:
– FDA bulk drug substances under 503A, docket FDA-2025-N-6895
– FDA clarifies GLP-1 compounding policies
– Meto Health: 14 peptides expected reclassification 2026
– Loti Labs: BPC-157 legal status 2026 FDA update
– PeakedLabs: BPC-157 cost guide 2026
– IvyRx: Sermorelin cost 2026
– AMC Defense Law: peptide industry federal charges 2026
– The Peptide Catalog: vendor shutdowns 2025-2026
– PerfectB: BPC-157 cost clinic programs
– Lengea Law: FDA 503A review BPC-157 TB-500
– Harris Beach Murtha: GLP-1 off shortage list deadlines
– SURMOUNT-1 trial data, tirzepatide 22.5% weight loss, ClinicalTrials.gov
Want a real clinician to run the numbers, not a guess?
Joi + Blokes is a telehealth clinic that prescribes GLP-1 medication (Zepbound, compounded semaglutide and tirzepatide), hormone therapy (TRT, HRT), thyroid care, and peptides after a real lab panel and clinician review, with no membership or consult fee (prescriptions from about $59/month, lab panels from $149). If the scale will not budge, this is where you find out whether insulin, thyroid, or hormones are the real reason. Here is Joi + Blokes reviewed in full.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.