Last updated June 2026. Educational content, not medical advice. Consult a licensed dermatologist before starting any new skincare regimen.
Short answer: Peptides are short chains of amino acids that act as biological messengers in the skin, stimulating collagen production, improving hydration, relaxing expression lines, and reinforcing the skin barrier. A 2026 systematic review of 19 randomized controlled trials involving 1,341 participants found peptides significantly improved skin hydration and wrinkle depth, with oral collagen peptides driving the strongest measurable results and topical peptides showing real but more targeted benefits.
Peptides act as messengers that rebuild your skin from the inside, so what are your own biomarkers messaging right now? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Why does skin age in the first place?
Before understanding what peptides do, you need to understand what they are fighting. Skin gets its structure from a dense scaffold of collagen and elastin fibers embedded in the dermis, the deeper layer beneath the surface you see. Starting around age 25, your body produces roughly 1% less collagen per year. By your 40s, not only is production slowing, but an enzyme class called matrix metalloproteinases (MMPs) is also breaking down existing fibers faster than they can be replaced. The result is visible: thinner skin, more pronounced lines, reduced bounce-back, and a dull texture that skincare brands love to describe vaguely as “loss of radiance.”
Peptides step into this system. They do not create collagen themselves. What they do is send chemical signals to the cells, primarily fibroblasts, that do the building. Think of them as work orders arriving at a construction site that has been running on reduced staff for a decade. The building capacity is still there; the signal just got quiet.
The subtler truth: skin aging is also driven by oxidative stress, chronic low-grade inflammation, advanced glycation end-products (AGEs) from high blood sugar, and hormonal shifts. Peptides address the signaling piece but not all the others, which is why no single ingredient is the whole answer.
What do peptides actually do inside skin cells?
The mechanism breaks cleanly into four categories, each mapped to a named peptide class. Understanding these stops you from buying something that sounds impressive but does not match what you actually need.
Signal peptides: the collagen builders
Signal peptides bind directly to fibroblast receptors and trigger intracellular pathways, mainly TGF-beta and MAPK signaling, that tell the cell to synthesize more collagen, elastin, and hyaluronic acid. The best-studied example is Palmitoyl Pentapeptide-4, sold as Matrixyl by Sederma. In a double-blind, placebo-controlled trial, it produced a 36% reduction in wrinkle surface area after 12 weeks, with results comparable to retinol 0.07% but without retinol’s irritation. The second-generation formula, Matrixyl 3000, confirmed a 190% increase in type I collagen synthesis and an 80% increase in type IV collagen in vitro, with measurable improvements in skin density by high-frequency ultrasound after two months of twice-daily use.
Other signal peptides include Acetyl Tetrapeptide-9 (Dermican), which stimulates type I collagen, and Tetrapeptide-30 (PKEK), which reduces hyperpigmentation by inhibiting tyrosinase activity, making it relevant to both aging and post-inflammatory marks.
Carrier peptides: the copper delivery system
Carrier peptides do not stimulate cells directly; they ferry trace minerals to the places that need them. The most commercially important is GHK-Cu, or Copper Tripeptide-1, which binds copper ions and delivers them to copper-dependent enzymes including lysyl oxidase, the enzyme that cross-links and stabilizes newly formed collagen fibers. Without functional lysyl oxidase, new collagen is structurally weak regardless of how much of it you stimulate.
GHK-Cu occurs naturally in human plasma, but levels fall sharply with age: roughly 200 ng/mL at age 20 down to 80 ng/mL by age 60, a decline of over 60%. After 8 weeks of topical application, one trial found wrinkle depth became significantly smaller compared to vehicle control or a commercial benchmark product. It also upregulates extracellular matrix genes (COL1A1, elastin, decorin) and suppresses inflammatory cytokines. Formulations at 0.5% to 1% GHK-Cu are the range most dermatologists recommend for anti-aging purposes, with hydration improvements appearing at 1 to 2 weeks and firmness and wrinkle improvements building between weeks 6 and 12.
Neurotransmitter-inhibitor peptides: the topical Botox effect
A subset of peptides works at the neuromuscular junction rather than the dermis. Argireline (Acetyl Hexapeptide-3) mimics the N-terminal sequence of SNAP-25, a protein in the SNARE complex that governs acetylcholine vesicle release. Less acetylcholine means less muscle contraction means less deepening of expression lines. In one randomized, double-blind trial, Argireline showed 48.8% anti-wrinkle efficacy versus placebo in periorbital wrinkles over four weeks; a separate trial using 10% Argireline emulsion reduced wrinkle depth by up to 30% after 30 days.
Related options include Pentapeptide-18 (Leuphasyl), which inhibits neuronal activity through a different pathway, and Syn-Ake (Tripeptide-3), a synthetic analog of Waglerin-1 from temple viper venom that acts as an acetylcholine receptor antagonist. These are the peptides worth prioritizing if expression lines rather than structural collagen loss are the main concern.
Enzyme-inhibitor peptides: protecting what you already have
Rather than building new matrix, enzyme-inhibitor peptides slow down the enzymes destroying existing collagen and elastin. Silk peptides capture up to 80% of reactive oxygen species in vitro; rice peptides inhibit metalloproteinase activity. Soybean-derived peptides of 3 to 6 amino acids show similar MMP-inhibiting properties. These work best as maintenance ingredients in mature skin rather than rapid correctors, and they are underrepresented in marketing relative to their defensive utility.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Comparing the four peptide types: what each one is best for
| Peptide type | Mechanism | Best for | Named example | Evidence level |
|---|---|---|---|---|
| Signal peptides | Stimulate fibroblast collagen / elastin synthesis | Structural loss, fine lines, skin density | Matrixyl 3000 (Palmitoyl Pentapeptide-4 + -7) | Strong; multiple placebo-controlled trials |
| Carrier peptides | Deliver copper to stabilize new collagen, reduce inflammation | Skin repair, wound healing, redness, firmness | GHK-Cu (Copper Tripeptide-1) | Moderate-strong; in vitro + clinical trials |
| Neurotransmitter inhibitors | Reduce muscle contraction at expression lines | Forehead lines, crow’s feet, frown lines | Argireline (Acetyl Hexapeptide-3) | Moderate; several short-term RCTs |
| Enzyme inhibitors | Block MMP collagen degradation, neutralize ROS | Maintenance, protection against breakdown | Silk peptides, rice peptides, soybean peptides | Modest; mostly in vitro data |
Personally, if I had to pick one category for a starter protocol, I would choose a signal peptide serum. The evidence is deepest, the mechanism is direct, and the benefits compound over months in a way that enzymatic inhibitors and neurotransmitter peptides do not.
Do topical peptides actually penetrate skin?
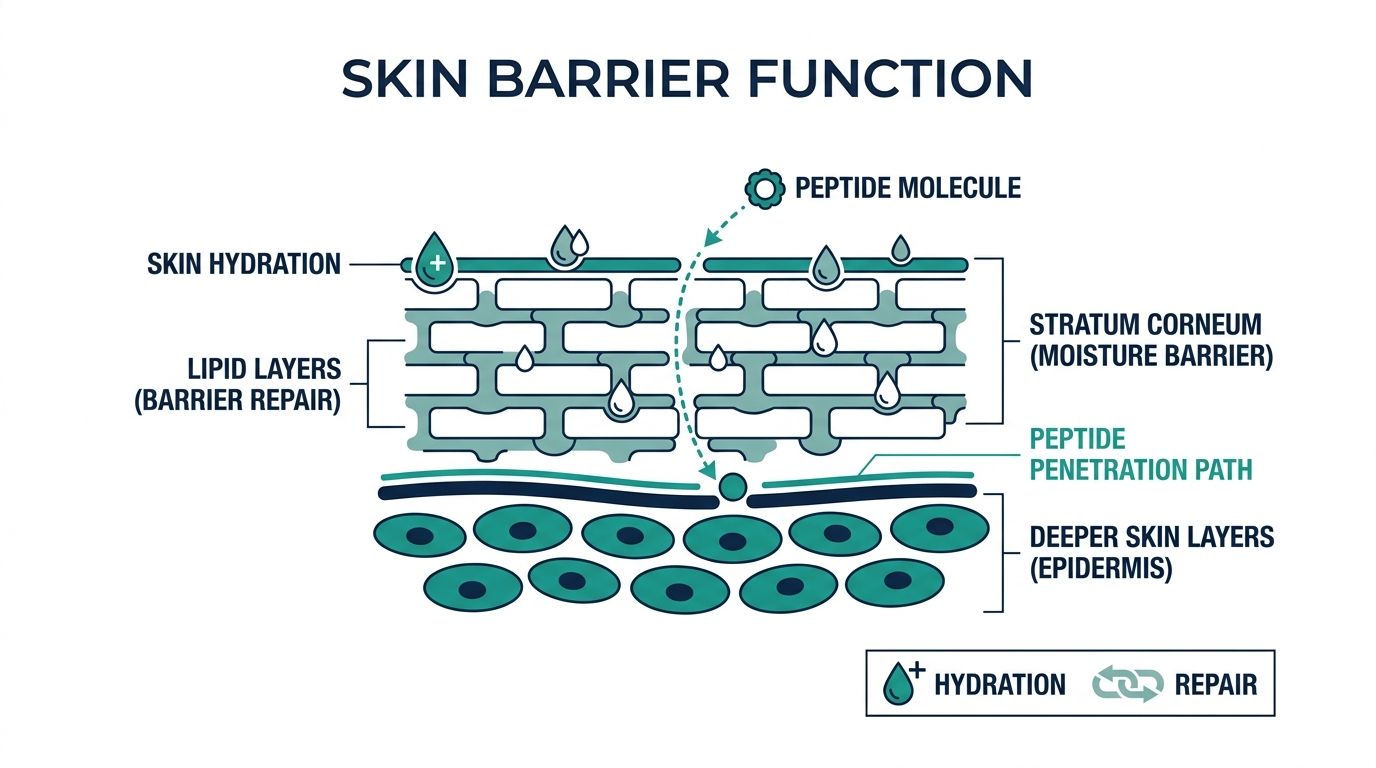
This is the legitimate scientific tension that critics raise, and it deserves a straight answer. The skin’s outer barrier, the stratum corneum, is designed to keep molecules out. Larger proteins cannot cross it at useful concentrations. Peptides, being short chains of 2 to 10 amino acids, sit in a molecular weight range (typically 500 to 4,000 Daltons) where penetration is possible but far from guaranteed.
The 2026 systematic review from Frontiers in Medicine noted this directly: topical peptide formulations showed “limited impact” on wrinkle reduction compared to oral peptides in the pooled data, partly because only two topical studies met the inclusion criteria versus 17 oral studies. That said, individual trial results for specific topical peptides, Matrixyl, Argireline, GHK-Cu, are positive enough to justify their use.
Formulators have developed delivery enhancement approaches that improve penetration meaningfully. Nanoemulsions (20 to 200 nm particle size) and liposomes (0.05 to 5 micrometers) increase skin uptake significantly. Solid lipid nanoparticles also show promise; a trial with Pentapeptide-18 in solid lipid nanoparticles found wrinkle improvement after 8 weeks of daily application. In clinical settings, iontophoresis using electrical current under 500 microamperes per square centimeter and microneedles (25 to 2,000 micrometers in length) dramatically increase delivery. For over-the-counter products, the formulation vehicle matters as much as the peptide concentration, and brands rarely disclose enough detail to evaluate it properly.
There is a phrase that belongs in every skincare article: “in vitro” and “in vivo” are not the same thing. A peptide that shows a 190% collagen increase in a cell culture does not necessarily produce a 190% collagen increase in your face. The cell culture has no barrier, no competing enzymes, no competing signals. Be cautious about any brand that presents cell-culture data as clinical evidence.
Peptides vs. retinol: the comparison everyone searches for
Retinoids remain the most thoroughly validated topical anti-aging ingredient class in dermatology, with decades of peer-reviewed data showing increased cell turnover, collagen stimulation, and reversal of sun damage. Peptides, by contrast, have a shorter and spottier published record, with many trials sponsored by ingredient manufacturers. So why bother with peptides?
Three practical reasons:
Tolerability. Retinoids produce initial irritation, redness, flaking, and photosensitivity in the majority of users. Peptides produce none of these. For anyone with rosacea, sensitive skin, periorbital use, or who is pregnant or breastfeeding (where retinoids are contraindicated), peptides are the workhorse ingredient that retinoids cannot be.
Different mechanisms, additive effects. Retinol drives cell turnover and collagen via retinoic acid receptors. Signal peptides drive collagen via fibroblast receptors. Neurotransmitter inhibitors work at the neuromuscular junction. These pathways do not compete; they stack. A morning peptide serum paired with an evening retinol is a legitimate dual-axis approach, with peptides applied first, retinol second, allowing the peptide’s barrier-supporting properties to buffer some of retinol’s irritation.
Eye area and neck applicability. Retinol around the eyes and on the neck is possible but requires care; thinness of the skin amplifies irritation. Argireline and other neurotransmitter peptides are specifically designed for these zones and require no acclimatization period.
Do not believe anyone who tells you peptides are “just as effective as retinol” for treating established deep wrinkles and significant photodamage. The evidence does not support that. But equally, do not dismiss peptides as marketing fluff: the signal-peptide data is real, and the combination approach is genuinely better than either ingredient alone.
Oral collagen peptides vs. topical: which route is stronger?
The 2026 Frontiers in Medicine systematic review analyzed 19 RCTs with 1,341 participants and found oral polypeptides drove the largest pooled effect for wrinkle reduction (mean difference 1.5, p = 0.01) and skin hydration (mean difference 16.50), significantly outperforming topical formulations across most measured outcomes. Skin brightness also showed significant improvement with oral peptides (mean difference 2.40, p < 0.01).
A 2025 randomized, double-blind, placebo-controlled trial published in PMC found low-molecular-weight collagen peptide supplementation significantly improved skin elasticity parameters (R2, R5, and R7 by cutometry), surface and deep hydration, and dermal density, with effects maintained during a 2-week discontinuation period. The bovine-derived bioactive collagen peptide data is also strong: a double-blind trial with 66 women aged 35 to 55 taking 2.5 g per day for 8 weeks found objectively measured improvements in eye wrinkle volume, skin elasticity, and hydration at both the 4-week and 8-week marks.
The usual therapeutic dose for oral collagen peptides runs 2.5 g to 10 g per day, with the most commonly studied dose around 4 g. The mechanism is different from topical peptides: ingested peptides are digested into di- and tri-peptides that enter circulation and are believed to act as systemic signals, triggering fibroblast activity throughout the dermis. They do not “become” collagen directly.
Practically: oral and topical peptides are not competing, they address overlapping but not identical pathways. A reasonable protocol uses both, with oral collagen peptides providing a systemic baseline and topical peptides targeting specific concerns like a peptide serum on expression lines or a GHK-Cu formula for barrier repair.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
How to use peptides in a skincare routine
Layering order matters, and the rules are consistent across formulations:
Morning: cleanser, vitamin C serum (antioxidant protection pairs with peptide synthesis), peptide serum, moisturizer, SPF. Vitamin C goes first because it requires a lower pH environment; peptides are stable across a wider pH range and will not destabilize after vitamin C absorption.
Evening: cleanser, peptide serum (2 minutes to absorb), retinol or retinoid if using, moisturizer. The peptide-first approach lets barrier-supportive peptides, particularly GHK-Cu, buffer some of retinol’s irritation. Peptides and retinol have no pH conflict and no competing mechanisms; the combination is well-tolerated.
One practical note on copper peptides: do not layer GHK-Cu directly with high-concentration vitamin C in the same step. Copper ions and ascorbic acid can interact and potentially oxidize. Keep them in separate AM and PM routines, or allow significant absorption time between them. This is the formulation detail that most “can you mix this?” articles gloss over.
Beginners can build in phases. Weeks 1 to 2: peptide serum morning and evening, confirm tolerance. Weeks 3 to 4: if using retinol, introduce it at 0.1% to 0.3% two nights per week in the evening. Weeks 5 to 10: build retinol to nightly use. The phased approach avoids stacking too many actives simultaneously, making it easier to identify the source of any reaction.
Timeline expectation: hydration improvements with topical peptides can appear in 1 to 2 weeks. Visible firmness and wrinkle improvements build between weeks 6 and 12, with maximum results building over 3 to 6 months. Anyone expecting dramatic change at the 2-week mark will call peptides useless. They work on a slower, structural clock.
Three things dermatologists know that marketing does not say
1. Single-peptide or minimal-peptide systems often outperform stacked formulas. More peptide names on an ingredient list is not evidence of more efficacy. When ten peptides are each at 0.01% concentration, none of them is at a therapeutically meaningful dose. The brands that publish actual active concentrations (NIOD, The Ordinary, Skin Biology) are doing something the ingredient-collage brands are not: committing to a testable claim.
2. Peptide serum formulations with preservative systems using chelating agents (like EDTA) can bind the copper in GHK-Cu and reduce its activity. This is a known formulation challenge that very few brands acknowledge and even fewer solve. A formulator who has thought about this will tell you they use alternative preservation approaches; one who has not will tell you the product contains “multiple synergistic actives.”
3. Silk and plant-derived peptides are real but underused. Silk peptides from Bombyx mori fibroin capture roughly 80% of reactive oxygen species in vitro and inhibit collagen degradation. They appear mostly in premium Asian skincare formulations (Sulwhasoo, SK-II derivatives, some Tatcha products) and rarely in the peptide-forward Western serums that dominate search results. If you want enzyme-inhibitor coverage, these products are where to look.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
Turn what you just learned into action.
Superpower lets you test 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
FAQ: what do peptides do for skin?
Do peptides actually work, or is it marketing?
Some peptides have genuine clinical evidence. Palmitoyl Pentapeptide-4 (Matrixyl) has multiple placebo-controlled trials showing wrinkle reduction. GHK-Cu has published in vitro and clinical data on collagen synthesis and wound healing. Argireline has randomized trials showing 48.8% anti-wrinkle efficacy versus placebo. The category as a whole is not hype; specific peptides at meaningful concentrations in well-formulated products do produce measurable results.
How long does it take for peptides to work on skin?
Hydration improvements can appear in 1 to 2 weeks. Firmness, wrinkle depth, and structural changes build over 6 to 12 weeks with consistent twice-daily use. If you are evaluating a peptide product at 2 weeks, you are evaluating the wrong window.
Can peptides replace retinol?
No, not for treating established photodamage or significant wrinkle depth. Retinoids have the stronger evidence base for reversing sun damage and driving cell turnover. Peptides are better suited to: those with sensitive skin who cannot tolerate retinol, the eye and neck area, the morning routine, and as a complementary layer alongside retinol in the evening. The combination is meaningfully better than either alone.
Is GHK-Cu (copper peptide) safe?
A 2018 review in the peer-reviewed literature called it a “safe, inexpensive, extensively studied compound.” It is generally well-tolerated topically with minimal reported adverse events across decades of clinical use. Note that injectable GHK-Cu sold through research-chemical vendors is a different risk class entirely, involving reconstitution, dosing math, and zero clinical oversight.
Can I use peptides with vitamin C?
Yes, with timing. Apply vitamin C first in the morning, allow it to absorb, then apply the peptide serum. For copper peptides specifically, keep high-concentration vitamin C and GHK-Cu in separate AM and PM steps to prevent potential copper oxidation.
What is the best peptide for skin firmness?
GHK-Cu and signal peptides like Matrixyl 3000 have the strongest evidence for improving skin firmness and density. GHK-Cu also delivers copper to lysyl oxidase, which cross-links and stabilizes new collagen, making it particularly relevant for structural firmness rather than surface-level hydration.
Are oral collagen peptides better than topical?
The 2026 meta-analysis found oral peptides outperformed topical in pooled wrinkle reduction and hydration data, largely because oral studies dominated the evidence base. Practically, the two routes are complementary: oral collagen peptides at 2.5 to 10 g daily for systemic collagen support, topical peptides for targeted, site-specific signaling.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources:
- Frontiers in Medicine: Oral and topical peptides for skin aging: systematic review and meta-analysis of RCTs (2026)
- PMC: Peptides: Emerging Candidates for the Prevention and Treatment of Skin Senescence (2025)
- PMC: Low-molecular-weight collagen peptide supplementation in healthy adults, RCT (2025)
- PMC: Collagen peptides affect collagen synthesis and gene expression in fibroblasts (2024)
- Innerbody: GHK-Cu Peptide benefits, side effects, and more (2026)
- Asterwood: Copper Peptides (GHK-Cu) for Skin: Complete Guide 2026
- Peptide Journal: Matrixyl Clinical Studies Anti-Wrinkle Evidence
- City Skin Clinic: Peptides vs Retinoids
- Onekind: Retinol and Peptides: Can You Use Them Together?
- Grand Ingredients: Copper Peptides Clinical Evidence and Skin Benefits (2025)
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.