Last updated 18 June 2026. Educational content, not medical advice. Peptide therapy carries real risks; talk to a licensed clinician before starting anything.
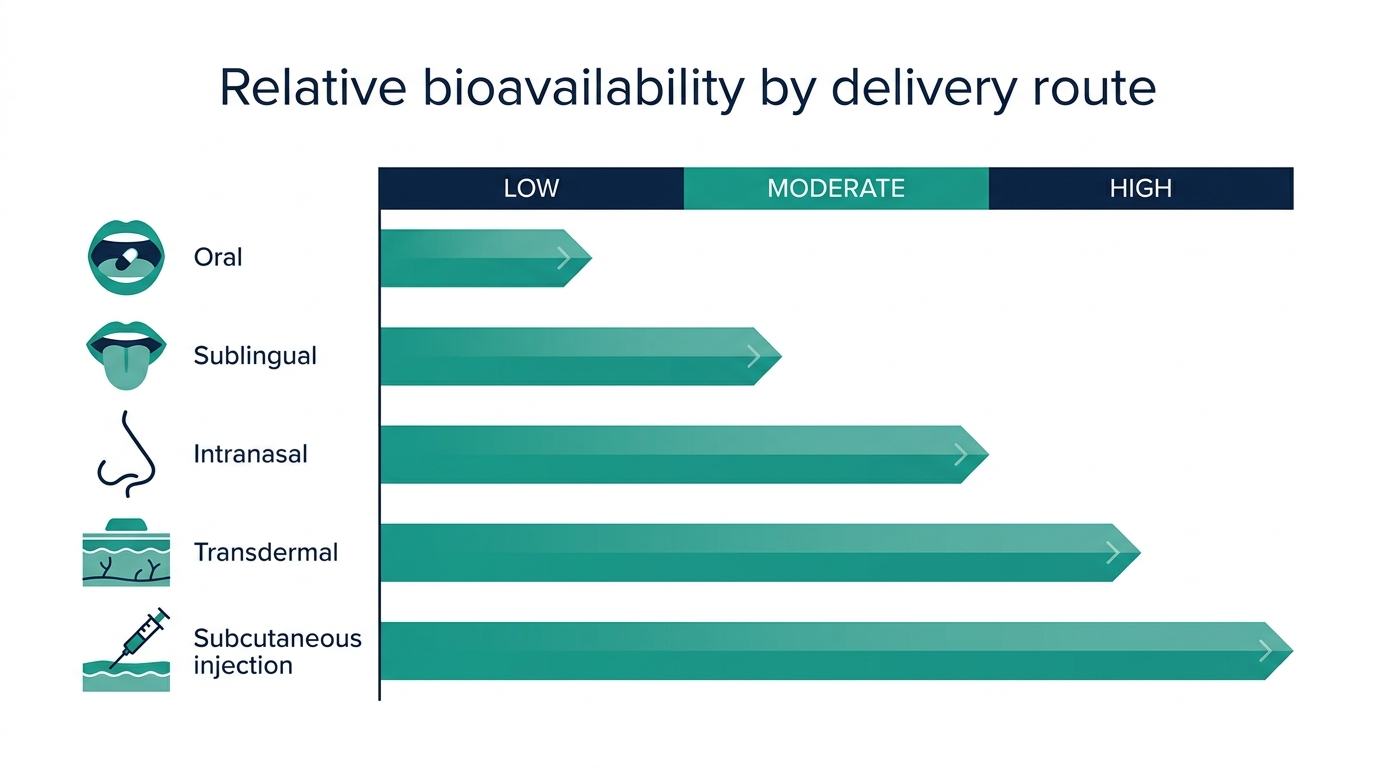
Short answer: Yes, several peptides work without a needle, and one of the biggest pharmaceutical approvals of 2025 proved it: the FDA greenlit the oral Wegovy pill (semaglutide 25 mg) on December 22, 2025, making injectable semaglutide optional for the first time. But the honest answer is more complicated. The route that lets you skip the syringe almost always comes with a bioavailability penalty, sometimes a severe one. A collagen peptide powder dissolves in your coffee and reaches your bloodstream at over 63% absorption. An oral dose of injectable-grade semaglutide reaches your bloodstream at 0.4 to 1%. The gap between those two numbers is the real story of needle-free peptide delivery.
Needle-free peptide options are expanding fast. Before you choose one, see what your own bloodwork actually needs. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Why do most peptides even require a needle?
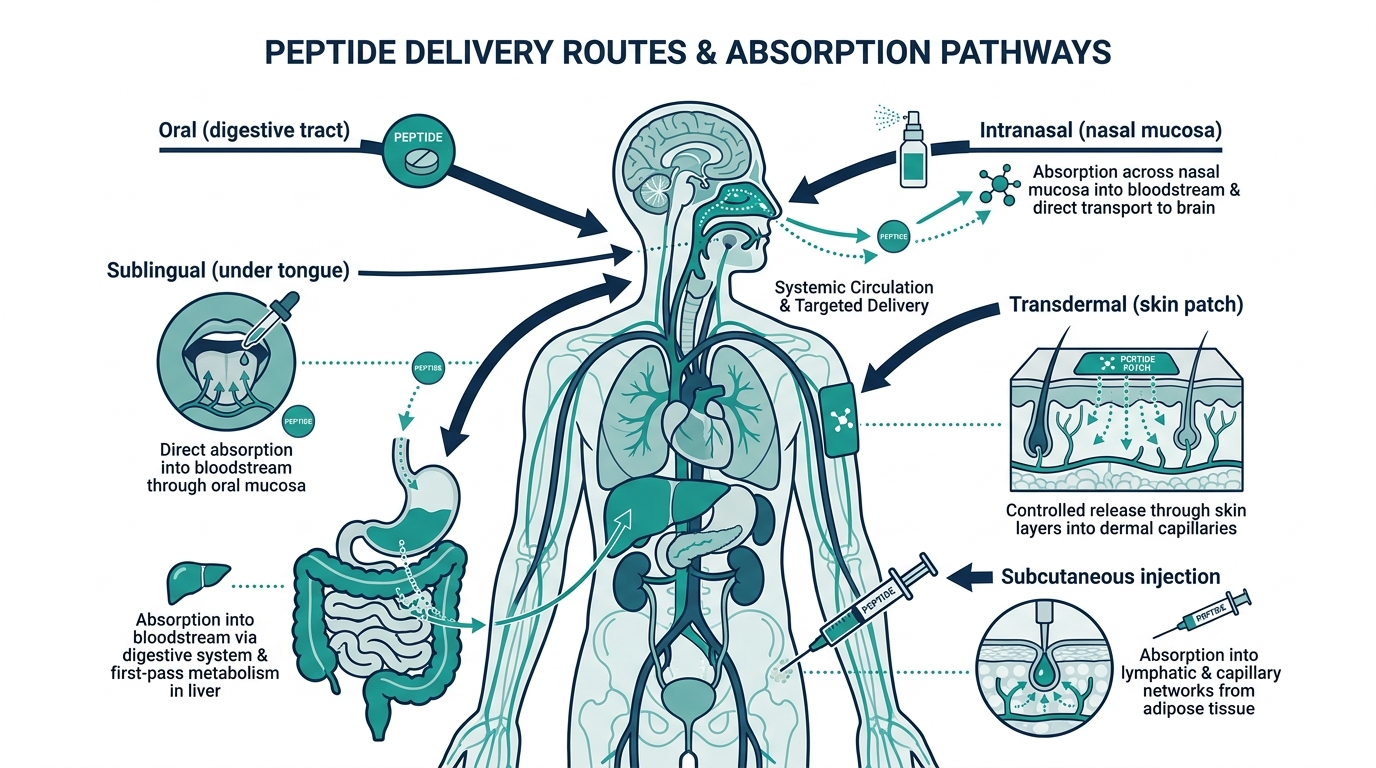
Peptides are short chains of amino acids. The digestive system is extraordinarily good at breaking them apart, because breaking peptide bonds is exactly what digestion is designed to do. Stomach acid, pancreatic proteases, and intestinal brush border enzymes collectively dismantle most therapeutic peptides before they reach the bloodstream, reducing bioavailability to single-digit percentages or less.
Injectable delivery bypasses this entirely. A subcutaneous injection deposits the peptide directly into tissue where it absorbs into capillaries without running the enzymatic gauntlet. The needle is inconvenient, not arbitrary.
This is the challenge every needle-free formulation is trying to solve: how do you get a molecule that the body is designed to destroy in the gut into the bloodstream intact?
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Which peptides actually work without a needle?
The answer depends almost entirely on the peptide’s molecular weight, stability in stomach acid, and intended target (gut vs. systemic vs. skin vs. brain). Here is a reality-checked breakdown of every mainstream needle-free route.
Oral pills and capsules
The only FDA-approved oral peptide for weight management as of mid-2026 is oral semaglutide, sold as Rybelsus (diabetes) and now the Wegovy pill (obesity). Novo Nordisk’s approach uses a co-formulation with SNAC (sodium N-[8-(2-hydroxybenzoyl) amino caprylate]), a permeation enhancer that transiently opens tight junctions in the stomach lining.
Even with SNAC, oral bioavailability sits at roughly 0.4 to 1%. The reason oral semaglutide works despite that number is semaglutide’s unusually long plasma half-life of approximately 168 hours, which allows enough accumulation from tiny daily doses to produce a therapeutic effect. The OASIS 4 Phase 3 trial showed oral semaglutide 25 mg once daily produced 16.6% mean weight loss over the trial period, and about one in three participants lost 20% or more of their body weight.
Do not assume this trick generalizes. BPC-157, sermorelin, and ipamorelin have half-lives measured in minutes, not hours. An oral capsule form delivers a fraction of a fraction, with no time to accumulate. Oral BPC-157 capsules likely achieve less than 10% systemic bioavailability, and the honest guidance from researchers who have followed this closely is that oral BPC-157 is best suited for local gut and GI applications, not systemic tendon or muscle repair.
Personally, if someone tells you oral BPC-157 capsules are equivalent to injectable BPC-157 for a shoulder injury, they are either misinformed or selling you the easier option. The local gut effect is plausible and has some support. The systemic injury recovery claim does not.
Nasal sprays
Intranasal delivery is genuinely underrated, but only for the right peptides. The nasal mucosa is highly vascularized, and the olfactory epithelium provides a direct anatomical route to the central nervous system via axonal transport along cranial nerve I, bypassing the blood-brain barrier.
Molecular weight is the critical filter. Research published in Expert Opinion on Drug Delivery puts general peptide nasal bioavailability below 5% for most compounds. But smaller peptides with CNS targets are a different category:
- Selank (751 daltons): intranasal bioavailability reported at approximately 92.8%, with detectable blood levels within 30 seconds of administration.
- Semax (similar molecular profile to Selank): high CNS bioavailability intranasally; developed at the Russian Academy of Sciences specifically for intranasal use.
- GHRP-2: roughly 50% nasal bioavailability.
- Ipamorelin: approximately 20% nasal bioavailability.
PT-141 (bremelanotide) is an instructive cautionary case. It was originally developed as a nasal spray, but clinical trials found the intranasal formulation caused significant nausea, flushing, and headaches. The FDA ultimately approved it in 2019 as Vyleesi, a subcutaneous injection, not a spray. The nasal route was real, the side effect profile was not acceptable.
For neurological and anxiolytic peptides like Selank and Semax, intranasal is arguably the superior route, not a compromise. For large peptides targeting peripheral tissue, it is a step down from injection without the absorption upside.
Sublingual troches and oral films
Sublingual troches are compounded lozenges that dissolve under the tongue, absorbing directly into the sublingual vasculature and bypassing first-pass liver metabolism. Dissolvable oral strips work the same way.
Multiple compounding pharmacies currently produce sublingual formulations for sermorelin, BPC-157, PT-141, NAD+, and thymosin alpha-1. Sermorelin troche bioavailability runs in the 15 to 30% range, compared to near-100% for subcutaneous injection. To compensate, a typical sublingual dose of sermorelin is 500 to 1,000 mcg versus the 200 to 500 mcg injectable dose.
The troche is a real, clinically used delivery format, not a marketing workaround. Strive Pharmacy, Restorative Compounding, and FormulaRx all offer licensed compounded sermorelin troches as of 2026. The catch: they still require a prescription, because they are still prescription drugs. You are skipping the needle, not the clinician.
There is a version of this conversation where “no needles” becomes “no oversight,” and that is the path to a different set of problems entirely.
Topical application (skincare peptides)
For cosmetic peptides, topical application is not a workaround. It is the correct route. Collagen peptides applied topically, GHK-Cu (copper peptide) serums, and signal peptides like Matrixyl (palmitoyl pentapeptide-4) are all designed to act at or near the skin surface, or to penetrate into the dermis where they stimulate fibroblast activity.
GHK-Cu is the clearest example. The Leyden 2002 photoaging trial established topical GHK-Cu’s clinical effects on wrinkle depth, and a 2023 IRB-approved study of 21 women using topical GHK-Cu gel reported an average 28% increase in skin collagen density at 3 months. An ongoing clinical trial (NCT07437586) is currently evaluating topical GHK-Cu gel for wound healing outcomes.
That said, skin barrier penetration limits topical absorption compared to injectable routes. Advanced delivery systems including liposomal encapsulation, microneedle-assisted application, and iontophoresis can raise absorption meaningfully. Iontophoresis uses a mild electrical current to drive charged peptide molecules through the skin without a needle and without degrading the molecule’s structure. Clinics like Hope Brain and Body Recovery Center are using this technique for localized application of NAD+, GHK-Cu, and BPC-157 as of 2026.
Oral collagen peptides (the category that just works)
Hydrolyzed collagen is the most successful oral peptide story in existence, and it does not get enough credit in the therapeutic peptide conversation. A 2024 randomized crossover trial published in Frontiers in Nutrition found that collagen hydrolysates from fish, porcine, and bovine sources all yielded clinically relevant plasma concentrations of hydroxyproline-containing di- and tripeptides after a single oral dose, regardless of molecular weight (2,000 to 5,000 Da) or source. More than 63.4% of collagen was absorbed from the intestine in the form of peptide.
Why does collagen work orally when semaglutide barely survives? Collagen peptides are processed from a food protein, not a therapeutic hormone. The fragments that survive digestion, particularly the Gly-Pro-Hyp tripeptide, are small and stable enough to pass through intestinal membranes and reach skin, cartilage, and connective tissue at measurable concentrations. The mechanism is fundamentally different from trying to get a GLP-1 molecule through the gut intact.
Do not conflate the oral success of collagen peptides with evidence that oral versions of therapeutic peptides work just as well.
Route-by-route comparison table
| Delivery route | Best peptides | Bioavailability (approx.) | Legal status | Requires prescription? | Real-world notes |
|---|---|---|---|---|---|
| Subcutaneous injection | All therapeutic peptides | Near 100% | Varies (Rx or research) | For Rx peptides yes | Gold standard; most research conducted here |
| Oral pill/capsule | Semaglutide (Wegovy/Rybelsus); collagen | 0.4-1% (semaglutide); 63%+ (collagen) | FDA-approved (sema); supplement (collagen) | Yes (semaglutide) | Only works for long-half-life peptides or food-derived fragments |
| Nasal spray | Selank, Semax, GHRP-2, Ipamorelin | 5-93% depending on peptide | Research / grey zone | No (research); yes (compounded) | Excellent for CNS-targeted peptides under 6,000 Da |
| Sublingual troche | Sermorelin, BPC-157, PT-141, NAD+ | 15-30% | Compounded Rx (licensed pharmacy) | Yes | Real clinical format; prescription still required |
| Topical serum/cream | GHK-Cu, Matrixyl, signal peptides | Low without enhancement; moderate with iontophoresis | Cosmetic OTC | No | Correct route for skin targets; not systemic |
| Microneedle patch | Semaglutide (research stage) | Under development | Investigational | N/A | PharmaTher patch in development as of January 2026; no FDA approval yet |
| Oral collagen powder | Collagen hydrolysates | 63%+ (peptide fragments) | Dietary supplement | No | Excellent absorption; different mechanism than therapeutic peptides |
What about GLP-1 patches?
Since Novo Nordisk’s Wegovy pill approval in December 2025, a parallel wave of interest has hit transdermal GLP-1 patches. The honest 2026 answer: no FDA-approved GLP-1 patch exists for weight management or diabetes. Products marketed as “semaglutide patches” or “Ozempic patches” sold over the counter are not regulated pharmaceuticals and have no verified active ingredient.
What does exist in the research pipeline is genuinely interesting. A 2024 PMC-published study (PMC11486425) demonstrated a self-boosting microneedle patch delivering semaglutide every 7 days for up to one month in animal models, using programmable core-shell microneedle architecture. PharmaTher launched development of their PharmaPatch microneedle system targeting obesity in January 2026. These are early-stage medical devices navigating both drug and device regulatory pathways, with no clinical approval timeline confirmed.
Buying a “GLP-1 patch” from a supplement vendor right now is buying a sticker with health claims, not a drug delivery system.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
The myth worth busting
The most persistent myth in this space is that sublingual and oral peptide formulations are “just as effective” as injectable versions and that choosing them is simply a lifestyle preference. It is not. The bioavailability numbers are not small print. They are the entire story.
Do not believe any vendor or clinic that markets oral or sublingual BPC-157 as equivalent to injectable BPC-157 for systemic recovery, injury healing, or muscle repair, without providing clinical human bioavailability data. That data does not currently exist in the peer-reviewed literature. The preclinical evidence for BPC-157’s injectable effects is real and substantial. The evidence that oral or sublingual versions replicate those effects systemically is, as of 2026, largely absent.
The gut-specific applications of oral BPC-157 are a different story. BPC-157 was originally discovered and researched as a stomach-protective compound. A 2026 Frontiers in Drug Delivery review explicitly notes that local luminal exposure, not systemic absorption, is what oral peptides reliably deliver. For gastric ulcers, leaky gut, and GI inflammation, the oral capsule may actually be the correct route, precisely because it stays local.
What a licensed telehealth clinic actually offers needle-averse patients
Clinics including Defy Medical, Marek Health, and Hone Health now routinely discuss delivery alternatives during intake. The conversation has shifted considerably since 2024. Sermorelin troches from compounded pharmacies are prescribed by these platforms as a legitimate non-injectable option for patients who cannot or will not self-inject. The doses are higher than injectable equivalents, the cost is comparable, and the clinical monitoring structure is identical.
The insider piece that most people miss: when a telehealth platform is still prescribing injectable-only protocols without even mentioning troche or nasal alternatives for appropriate patients, it is often because the prescribing clinician has not updated their protocol in two years, not because alternatives do not exist. Asking the question directly at intake will get a different answer at most modern longevity clinics.
For GLP-1 therapy specifically, the oral Wegovy pill is now the cleaner choice for most new patients who are needle-averse. It avoids injection entirely, comes with full pharmacy dispensing and labeling, and has the strongest bioavailability data of any oral peptide currently approved.
Needle-free does not mean risk-free
Two things are true simultaneously. First, needle-free peptide delivery is real and expanding fast. Second, the marketing around it is running well ahead of the clinical evidence.
The risks of needle-free peptide products are different from injectable risks, not zero. Oral and sublingual peptides can still cause systemic effects, still interact with hormone systems, and still carry the same sourcing risks if bought from grey-market vendors. A sublingual BPC-157 troche from a licensed pharmacy is not the same product as a “sublingual BPC-157 strip” from a research-chemical website with no prescribing clinician involved. The format changed. The accountability question did not.
And for topical peptides sold OTC, the risk profile is genuinely low, which is why they are sold as cosmetics. If you are looking for the peptide-adjacent option with the best combination of evidence, accessibility, zero regulatory friction, and no syringe, hydrolyzed collagen powder and GHK-Cu serum are the honest answer. They do what they say. They are absorbed. The clinical evidence is real. They just do not give you the systemic therapeutic effects that the injectable peptide community is chasing.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Can you take peptides orally instead of injecting?
Some peptides work orally. Oral semaglutide (Wegovy pill, FDA-approved December 2025) achieves 16.6% mean weight loss in the OASIS 4 trial despite only 0.4 to 1% bioavailability, because semaglutide has a 168-hour half-life that allows accumulation. Hydrolyzed collagen peptides absorb at over 63%. Most short-half-life injectable peptides like sermorelin, BPC-157, and ipamorelin do not accumulate meaningfully from oral dosing. Oral forms may still have local gut effects, but systemic effects are not reliably replicated.
Do peptide nasal sprays actually work?
For the right peptides, yes. Selank reaches approximately 92.8% intranasal bioavailability and is detected in the bloodstream within 30 seconds. Semax was specifically engineered for nasal delivery. GHRP-2 achieves roughly 50% nasal bioavailability. For peptides over 6,000 daltons, or peptides targeting peripheral rather than CNS tissue, nasal bioavailability drops below 5% and injection remains the superior route.
Are sublingual peptide troches real medicine or a marketing workaround?
Sublingual troches are a real, compounded delivery format dispensed by licensed pharmacies under prescription. They achieve 15 to 30% bioavailability for sermorelin compared to near-100% for injection, requiring proportionally higher nominal doses. They are not equivalent to injection, but they are a clinically legitimate alternative for patients who cannot self-inject, prescribed through the same licensed telehealth channels.
Do GLP-1 patches work?
No FDA-approved GLP-1 patch for weight loss or diabetes exists as of June 2026. Products sold OTC as “semaglutide patches” are not pharmaceutical products. Microneedle research platforms including PharmaTher’s PharmaPatch are in development as of 2026 but have no confirmed clinical approval timeline. The approved needle-free GLP-1 option is the oral Wegovy pill (semaglutide 25 mg), available by prescription since January 2026.
Is topical BPC-157 effective?
Topical BPC-157 may have localized effects at or near the application site, especially with enhanced delivery systems like iontophoresis. Systemic bioavailability through intact skin is limited without assistance. Topical GHK-Cu has considerably stronger clinical evidence for skin applications, including a 2023 study showing 28% collagen density increase at 3 months, and an ongoing FDA-registered trial (NCT07437586).
What peptides work best without a needle?
Three categories stand out. Hydrolyzed collagen peptides orally (over 63% absorption, excellent safety, OTC, strong clinical evidence). GHK-Cu topically (cosmetic, evidenced, no prescription). And Selank or Semax intranasally (high bioavailability for CNS applications, research-grade). For GLP-1 therapy, oral semaglutide via prescription is now the cleanest needle-free option.
Does needle-free mean the peptide is safer?
No. Needle-free delivery reduces injection-site risks like bruising, infection, and sterile technique errors. It does not eliminate the systemic risks of the peptide itself, and it does not solve the sourcing and purity problem if buying from grey-market vendors. A sublingual strip from a research-chemical site with no prescribing clinician carries the same accountability gap as a vial from the same site, just dissolved differently.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources:
– FDA approves oral Wegovy pill, December 22, 2025 (PR Newswire)
– Frontiers in Drug Delivery, oral peptide bioavailability review, March 2026
– Frontiers in Nutrition, collagen hydrolysate absorption RCT, 2024
– PeptideDeck, BPC-157 oral vs injectable bioavailability
– SeekPeptides, sublingual peptide delivery guide
– Jay Campbell, peptide nasal spray vs injection bioavailability data
– OASIS 4 trial results, oral semaglutide 25 mg, AJMC
– ClinicalTrials.gov NCT07437586, topical GHK-Cu wound healing trial
– PubMed PMC11486425, microneedle semaglutide patch research
– Novo Nordisk oral Wegovy press release
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.