Last updated 18 June 2026. Educational content, not medical advice. Most peptides discussed here are not FDA-approved for muscle growth and many are sold under “research use only” labels not intended for human use. Speak with a licensed clinician before starting any peptide therapy.
Short answer: The CJC-1295 + Ipamorelin stack is the most clinically documented peptide combination for increasing growth hormone output and lean body mass, with a 2006 JCEM study showing 2 to 10-fold GH increases lasting up to six days per dose and IGF-1 elevation persisting 9 to 11 days. Sermorelin is the closest to a fully legal, telehealth-accessible prescription option at $175 to $225 per month. IGF-1 LR3 is the most mechanistically potent for direct muscle cell signaling but remains strictly a research compound. BPC-157 is the recovery workhorse that lets you train harder, not a hypertrophy agent itself.
CJC-1295 and Ipamorelin lead the growth hormone rankings. Curious what your own hormone panel actually shows? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
The honest setup: most content on this topic either oversells what peptides do to muscle or ignores the legal and practical realities. This article tries to do neither.
What do peptides actually do to muscle tissue?
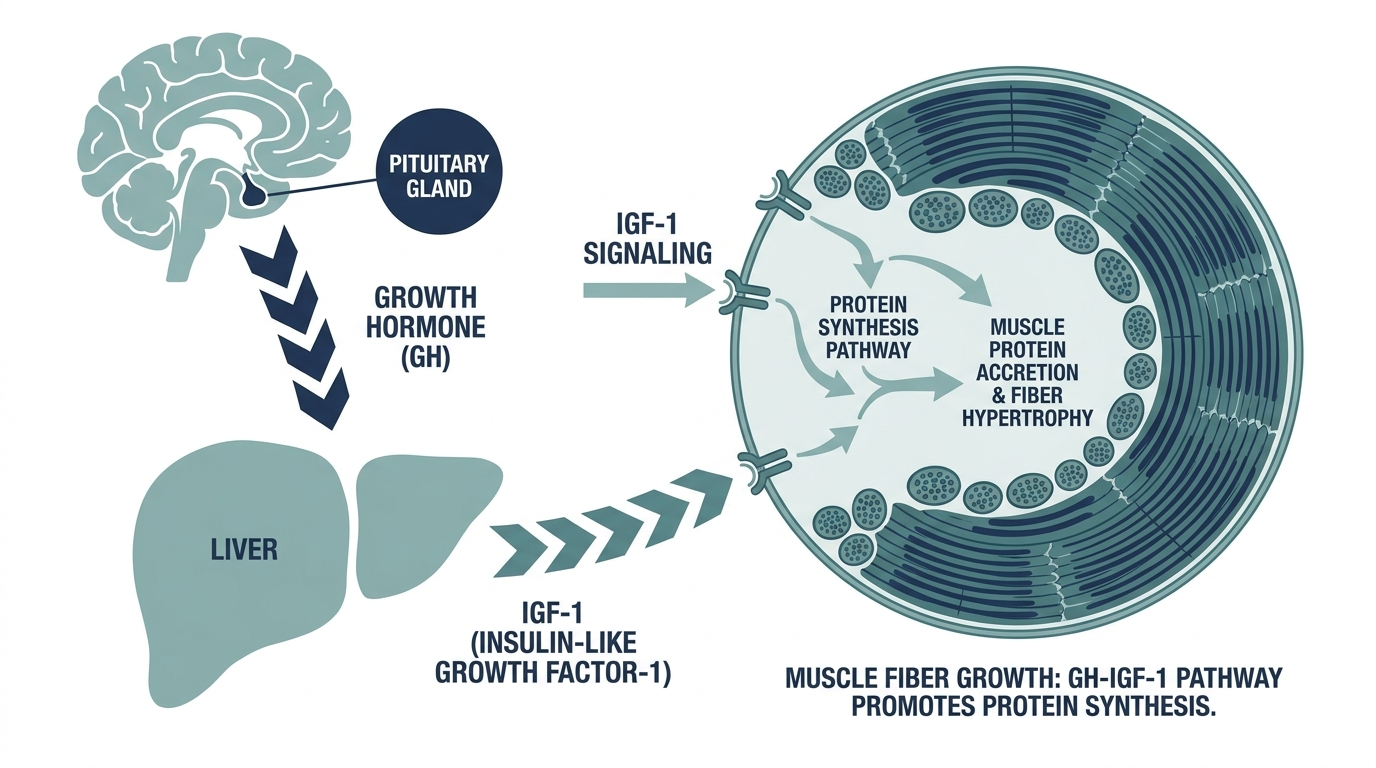
Before picking the “best” one, it helps to understand that no single peptide directly builds muscle the way a protein shake or progressive overload does. Peptides that target muscle growth work through the hypothalamic-pituitary axis, most of them by triggering the pituitary gland to release more growth hormone (GH), which then travels to the liver and stimulates production of IGF-1, and IGF-1 activates the PI3K/Akt/mTOR signaling pathway inside muscle cells that drives protein synthesis and fiber repair.
The key point, and one that gets glossed over in every forum thread: IGF-1 alone does not cause meaningful hypertrophy in vivo without a concurrent mechanical growth stimulus. A 2010 paper in the Journal of Cell Science demonstrated directly that IGF-1 infusion in mice produced little to no hypertrophy without the mechanical signal from resistance loading. The peptide amplifies the training response. It does not replace it.
That distinction matters enormously for setting expectations. A 40-year-old running CJC-1295 without a structured resistance program will see soft-tissue recovery benefits and maybe improved body composition from fat loss, but not the lean mass gains they saw in a gym at 25. The peptide and the training are the same system, not substitutes.
Which peptides are actually used for muscle growth?
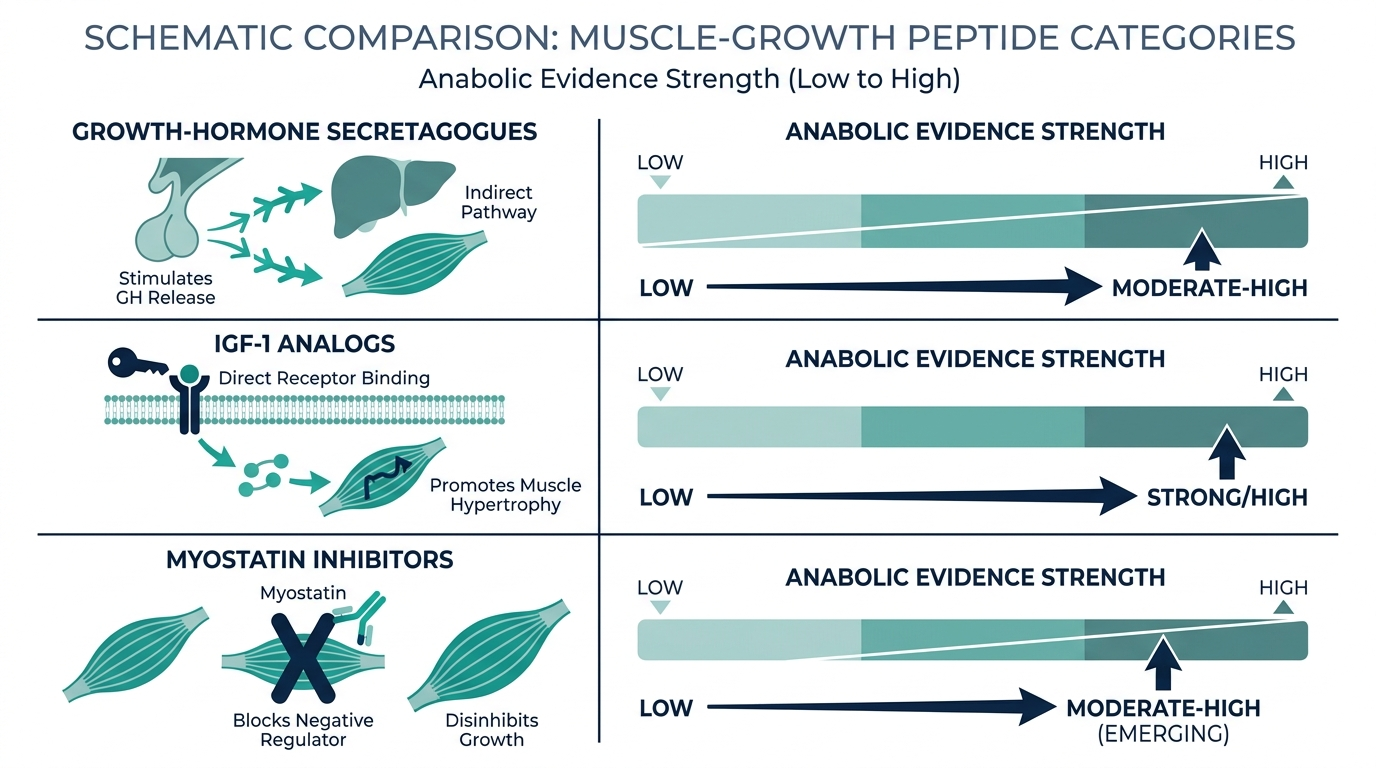
The market uses the phrase “peptides for muscle growth” to mean at least four completely different mechanisms and legal categories. Here is the honest map.
| Peptide | Primary mechanism | Legal lane in 2026 | Realistic muscle-growth use |
|---|---|---|---|
| CJC-1295 + Ipamorelin | GHRH + GHSR agonism, raises GH pulse | Research / grey (HHS thawing toward compounding) | GH elevation, lean mass over months of consistent use |
| Sermorelin | GHRH analog, mimics natural GHRH-1-29 | Prescription via telehealth | GH support, recovery, modest lean mass maintenance |
| Tesamorelin | Long-acting GHRH analog | FDA-approved (off-label for non-HIV use) | Visceral fat loss with lean mass preservation confirmed |
| IGF-1 LR3 | Direct IGF-1 receptor agonist | Research only | Most potent direct muscle signaling, highest risk profile |
| BPC-157 | Angiogenesis, collagen synthesis, tissue repair | Thawing grey zone (HHS Committee meeting July 2026) | Recovery enabler, not a hypertrophy agent |
| Hexarelin | GHSR agonist, potent GH pulses | Research only | Higher GH pulses than Ipamorelin, desensitizes with chronic use |
| MK-677 (Ibutamoren) | Oral ghrelin mimetic, sustained GH elevation | Research only, not FDA-approved | Oral convenience, but water retention common, no approved human use |
| Collagen peptides | Connective tissue substrate | Over-the-counter supplement | Tendon and ECM support, not direct hypertrophy |
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
CJC-1295 + Ipamorelin: the most studied stack
If you read one fact from this article, make it this: the only randomized, placebo-controlled clinical study on CJC-1295 in humans was published in the Journal of Clinical Endocrinology and Metabolism in 2006 by Teichman et al., and it remains the foundational reference nearly 20 years later, because no large-scale clinical trials on CJC-1295 for body composition have been run since. The FDA drug pipeline simply never picked it up.
What Teichman’s study showed: subcutaneous CJC-1295 in healthy adults aged 21 to 61 produced dose-dependent GH increases of 2 to 10 times baseline lasting six or more days per injection, and IGF-1 elevation of 1.5 to 3 times baseline persisting for 9 to 11 days. Estimated half-life of 5.8 to 8.1 days. No serious adverse reactions.
The clinical significance for muscle: IGF-1 in that 1.5 to 3-fold range is physiologically meaningful. Chronically elevated IGF-1, as seen in acromegaly, is dangerous, but the pulsatile, modestly elevated range from a GHRH analog tracks much closer to what you see in well-rested, anabolically primed healthy young adults, not a pharmacological overdose.
Ipamorelin is layered on top of CJC-1295 because they work on different receptor classes. CJC-1295 is a GHRH analog, acting on GHRH receptors to amplify the signal. Ipamorelin is a ghrelin receptor agonist (GHSR agonist), providing a synergistic GH pulse without meaningfully elevating cortisol or prolactin, which hexarelin and GHRP-6 both do. The selectivity of Ipamorelin is its main clinical appeal: cleaner GH release without the cortisol co-secretion that would counteract the anabolic effect.
Clinical timelines reported across telehealth programs using this stack: sleep quality and recovery improve within weeks one to four, visible body composition shifts appear at weeks six to twelve, and lean mass changes become measurable at months three to six of consistent use with resistance training. That is not a six-week transformation. It is a slow, compounding process.
Personally, the CJC-1295 + Ipamorelin combination is the one I would take most seriously of all the grey-market options, precisely because it has a named, peer-reviewed human study behind the core pharmacology. Most research peptides do not have that. It does not mean you should self-administer it outside of a clinical context, but it means the mechanism is not fiction.
IGF-1 LR3: the most potent, the most misunderstood
IGF-1 LR3 is a modified version of human IGF-1 with an arginine residue substituted at position 3 and a 13-amino acid N-terminal extension, which together prevent it from binding to IGF-binding proteins (IGFBPs) in the bloodstream. That structural trick extends its half-life from IGF-1’s roughly 12 to 15 minutes to approximately 20 to 30 hours, and it means the molecule stays free and active, not bound up in carrier proteins, for a sustained window.
The practical implication: IGF-1 LR3 does not need frequent redosing to maintain receptor activation, and it is estimated to be three times more potent than native IGF-1 at its receptor. In myocyte cell model research, EC50 values for mTOR activation and protein synthesis markers fall in the 0.1 to 10 nM range, and puromycin incorporation assays demonstrate protein synthesis enhancement with EC50 values of 3 to 7 nM.
What the forums often miss is the risk profile. Hypoglycemia is a real concern with IGF-1 LR3 above 50 mcg per day because IGF-1 shares structural similarity with insulin and has measurable insulin-like activity at higher concentrations. Theoretical long-term concerns include stimulation of IGF-1 receptors in non-muscle tissues, including cells with pre-existing oncogenic mutations. No long-term human safety data exists.
Do not believe the dosing protocols circulating on bodybuilding forums as if they are clinical guidance. They are not. They are crowd-sourced extrapolations from animal studies and anecdote. The absence of reported problems in a community that self-reports positive outcomes is not the same as safety data.
IGF-1 LR3 sits in a category where the mechanistic rationale is strong, the preclinical data is compelling, and the human safety evidence is essentially absent. That combination makes it interesting to researchers and high-risk for everyone else.
Sermorelin: the closest to a legitimate prescription path
Sermorelin is a synthetic 29-amino acid polypeptide matching the first 29 amino acids of human GHRH. The FDA approved the original sermorelin formulation (Geref) in 1997 for pediatric growth hormone deficiency diagnosis, but the manufacturer discontinued it in 2008 for commercial reasons unrelated to safety. All current adult sermorelin use is off-label, dispensed through licensed compounding pharmacies.
That history matters because it means sermorelin has a cleaner regulatory backstory than most peptides. It was never banned; it was discontinued. Compounding pharmacies can and do produce it legally, and telehealth platforms prescribing it are operating in a well-understood grey zone rather than an enforcement target zone.
The muscle-relevant mechanism: sermorelin stimulates the pituitary to release GH in a pulsatile pattern that mirrors the natural nocturnal GH surge. Unlike exogenous synthetic HGH, which raises GH continuously and suppresses the pituitary’s own output over time, sermorelin preserves the feedback loop. When you stop sermorelin, your own axis recovers normally. When you stop HGH, you may spend months waiting for pituitary function to normalize.
In practice, telehealth clinics using sermorelin for optimization report modest but measurable lean mass improvements over six to 12 months, usually in the range of 2 to 4 pounds of lean tissue alongside 4 to 8 pounds of fat loss in patients aged 40 to 65. The recovery benefits, particularly improved slow-wave sleep (where natural GH release peaks), are often the first thing patients notice.
Cost at major telehealth platforms in 2026: $175 to $225 per month at providers like Defy Medical and Ivy Rx, versus $1,000 to $3,000 monthly for synthetic HGH therapy. The math is not close. For someone whose primary goal is body composition and recovery rather than treating documented GH deficiency, sermorelin is the economically and legally sane choice.
BPC-157: the recovery peptide that makes everything else work better
BPC-157 (Body Protection Compound-157) is a 15-amino acid pentadecapeptide derived from a protective gastric protein sequence. It does not raise GH. It does not directly signal mTOR. Its value for a muscle-growth program is entirely indirect: it is the compound that keeps the connective tissue, tendons, and gut healthy enough to handle the training load that actually builds muscle.
The preclinical evidence is unusually consistent. A 2026 narrative review published in PMC covering three decades of BPC-157 research summarized accelerated tendon, bone, ligament, and muscle healing across experimental animal models, driven by VEGFR2 and nitric oxide signaling through the Akt-eNOS pathway, ERK1/2 activation, and a macrophage shift from pro-inflammatory to reparative phenotype.
The human data, though, is thin to a degree most promoters do not acknowledge. The same 2026 review found only three published human studies total: a 2021 retrospective of 16 knee pain patients (14 of 16 reported significant relief), a 2024 case series in interstitial cystitis patients, and a 2025 intravenous safety pilot in two healthy adults tolerating up to 20 mg IV with no adverse events. That is not a clinical trial. That is three small observational reports.
Three human studies across three decades of animal research is not a buried finding. It is the actual state of the science, and most BPC-157 content online treats it as established human medicine rather than what it is: a compelling preclinical compound awaiting real clinical development.
The regulatory situation is shifting. The FDA removed BPC-157 from its 503A Category 2 prohibited list on 22 April 2026, and HHS has signaled BPC-157 may return to Category 1 (permitted for compounding) status pending the Pharmacy Compounding Advisory Committee meeting set for 23 to 24 July 2026. If that happens, legally compounded injectable BPC-157 with physician oversight becomes possible, which would be a significant change from the grey-market-or-nothing situation of 2023 to 2025.
For now, WADA has banned it under the unapproved substances category since 2022, so any competitive athlete considering BPC-157 for tendon recovery is looking at a potential suspension, not just a health risk.
Tesamorelin: the only fully FDA-approved anabolic GHRH in the US
This one surprises people. Tesamorelin (brand name Egrifta) is FDA-approved for reducing visceral adipose tissue in HIV-associated lipodystrophy, and it is the most rigorously studied GHRH analog in humans because it went through the full Phase III clinical trial process.
In those trials, tesamorelin produced visceral fat reductions of approximately 15 to 18 percent over 26 weeks while preserving lean body mass (no significant LBM loss in treated subjects). A 2023 meta-analysis of randomized controlled trials confirmed it improves body composition, hepatic fat, lean body mass, and IGF-1 levels without serious safety signals or meaningful glucose perturbation in the HIV population.
The off-label extension of that finding to healthy adults wanting muscle growth is a significant leap that the data does not fully support. Tesamorelin preserves lean mass and reduces fat in a population with metabolic disease. It is a reasonable hypothesis that it produces similar body composition benefits in healthy aging adults, and some telehealth clinics prescribe it off-label for that purpose. But “preserves muscle in a diseased population” and “builds meaningful new muscle in a trained athlete” are different claims with different evidence requirements.
What tesamorelin does offer that the research compounds do not: a named manufacturer, consistent pharmacy-grade dosing, and a regulatory file. For someone who wants a GHRH analog with the cleanest legal and quality profile available, tesamorelin is the answer, at a higher cost than sermorelin.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Which peptide fits which goal? A decision guide
No single peptide is “the best” across all goals, and the right answer depends on your age, training status, health profile, and risk tolerance.
If you are over 40 and want sustainable body composition improvement with a clinical safety net: Sermorelin through a telehealth provider is the best risk-adjusted choice. Legal, monitored, $175 to $225 a month, and has supported the framework for compounded adult GHRH therapy for over 20 years.
If you are primarily dealing with nagging injuries that are limiting your training: BPC-157, once the July 2026 regulatory committee meeting clears it for compounding, will be the sensible licensed path. Until then, the grey-market route carries the usual caveats about purity and legality.
If you want the most clinically documented non-prescription option: CJC-1295 + Ipamorelin, purchased from a vendor with a verifiable third-party COA from labs like Janoshik, MZ Biolabs, or Colmaric, cross-checked against Finnrick’s independent vendor database. This is still the grey-market lane with all its risks, but it has more human pharmacokinetic data behind it than almost any alternative.
If you want to optimize connective tissue and joint health without injections: Collagen peptide supplementation combined with resistance training has a genuine evidence base. A 2015 randomized controlled trial in 53 elderly sarcopenic men demonstrated improved body composition and muscle strength versus placebo, and a 2024 Frontiers study confirmed reductions in exercise-induced muscle stress markers with specific collagen peptide use. It is not the same class of intervention as a GH secretagogue, but it is legal, inexpensive, and well-tolerated.
If you are a competitive athlete: Nearly every GH secretagogue and many connective tissue peptides appear on the WADA 2026 Prohibited List under Category S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics), banned at all times in and out of competition. Non-compliance carries strict sanctions because these substances are “non-specified,” meaning there is no reduced-sanction pathway for contamination claims. WADA also added semaglutide and tirzepatide to the monitoring program as of January 2026. Do not self-administer any injectable peptide in this category without a granted Therapeutic Use Exemption.
The myth that peptides replace training and sleep
The single most damaging misconception in this space: people hear “growth hormone” and assume peptides are a shortcut around the effort. They are not. A 2010 Journal of Cell Science study demonstrated directly that IGF-1 infusion in mice produced no significant hypertrophy without the mechanical signal from resistance loading. The pathway exists. The amplification requires the stimulus.
More to the point: the biggest natural GH pulse you get every 24 hours is the surge during slow-wave sleep, typically between 11 PM and 2 AM if you go to bed before midnight. That pulse drives the majority of overnight tissue repair and lean mass maintenance. A peptide that costs $225 per month will not compensate for six hours of fragmented sleep and no structured training program. Get those two right first, and the peptide is an accelerant applied to an engine that is already running.
A patient sleeping seven to eight hours, training four times a week with a high-protein diet, and optimizing testosterone and cortisol balance will see far more muscle growth than someone running CJC-1295 with poor sleep and no structured program. The peptide community rarely leads with this, because it is not a compelling sales narrative.
What does working with a telehealth clinic actually look like?
Entering the licensed route is less complicated than the forums make it seem. Most platforms that prescribe peptide therapy follow a standard intake model:
- Online consultation with a licensed physician, NP, or PA, usually 30 to 60 minutes.
- Required baseline labs, at minimum: IGF-1, testosterone (total and free), cortisol, CBC, CMP, and a lipid panel. Some platforms also require a thyroid panel.
- Protocol design based on labs and goals. A 45-year-old male with low-normal IGF-1 and poor sleep gets a different protocol than a 35-year-old with normal GH axis function and tendon issues.
- Medication dispensed from a named 503A or 503B compounding pharmacy with correct labeling, sterile preparation, and a pharmacist’s signature on every fill.
- Quarterly follow-up labs with protocol adjustments.
The red flags to walk away from: same-day prescriptions with no clinical review, “no labs required” messaging, pricing that is dramatically below market with no explanation, platforms that openly advertise grey-market compounds as if they are pharmacy products, and any “patient materials” that still carry “research use only” language.
Don’t just read about your health, track it.
A single result is a snapshot. Superpower re-tests 100+ markers over time so you can watch them move as you change sleep, food, and training.
Frequently asked questions
What is the best peptide for muscle growth overall?
The most clinically documented combination is CJC-1295 + Ipamorelin, with a randomized, placebo-controlled human trial in the Journal of Clinical Endocrinology and Metabolism (2006) showing 2 to 10-fold GH elevation and sustained IGF-1 increases. For a fully legal, prescription-accessible option, sermorelin through a telehealth provider is the safest choice. IGF-1 LR3 has the strongest direct mechanism but the thinnest human safety record.
Do peptides actually build muscle or just support GH?
Peptides work by raising GH and IGF-1, which in turn activate the PI3K/Akt/mTOR signaling pathway in muscle cells, driving protein synthesis and fiber repair. A mechanical training stimulus is required for meaningful hypertrophy. Peptides amplify the response to training; they do not substitute for it.
Are muscle growth peptides legal in 2026?
It depends on the compound and your intent. Sermorelin and tesamorelin are available by prescription through licensed telehealth. CJC-1295, Ipamorelin, and IGF-1 LR3 are not FDA-approved and are sold as “research use only,” meaning they are legal to possess but not labeled for human use. BPC-157 is in a regulatory transition, with an FDA committee meeting on 23 to 24 July 2026 that may return it to permitted compounding status. Competitive athletes should check the WADA 2026 Prohibited List before using any of these.
How much do peptide therapy programs cost for muscle growth?
Sermorelin via telehealth runs $175 to $225 per month, with labs and monitoring included at most reputable providers. Broader peptide therapy programs with CJC-1295 / Ipamorelin or tesamorelin run $199 to $399 per month. Grey-market research vials of CJC-1295 or BPC-157 cost $40 to $120 per vial, but include no clinical oversight, verified purity, or correct dosing. Insurance does not cover any of this.
How long before peptides show results for muscle growth?
Expect three phases: weeks one to four bring sleep and recovery improvements, weeks four to eight bring subtle energy and training capacity gains, and visible body composition changes require six to twelve months of consistent use with structured resistance training. Anyone promising visible muscle gains in four to six weeks from a GH secretagogue is selling a timeline that the pharmacokinetics do not support.
Is IGF-1 LR3 safe?
There is no long-term human safety data for IGF-1 LR3. The theoretical concerns include hypoglycemia (it shares insulin-like activity at higher doses), potential stimulation of IGF-1 receptors in non-muscle tissues, and growth-promoting effects in cells with pre-existing mutations. It remains strictly a research compound with no approved human use. The absence of large-scale reported harms in the bodybuilding community is not safety data.
What is the difference between peptides and HGH for muscle growth?
Synthetic HGH injects the hormone directly, providing constant elevation that suppresses the pituitary’s own GH production over time. Peptide GH secretagogues (CJC-1295, sermorelin, tesamorelin) stimulate the pituitary to produce GH in pulsatile bursts that preserve the natural feedback loop. Peptides cost far less ($175 to $225 per month versus $1,000 to $3,000 for HGH therapy) and do not suppress endogenous GH axis function. The tradeoff is lower peak GH levels.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources (verify live before publish):
– Teichman SL et al. “Prolonged Stimulation of Growth Hormone and IGF-I Secretion by CJC-1295.” JCEM 2006. https://pubmed.ncbi.nlm.nih.gov/16352683/
– PMC Narrative Review of BPC-157 for Musculoskeletal Healing (PMID 12446177, 2026). https://pmc.ncbi.nlm.nih.gov/articles/PMC12446177/
– Journal of Cell Science: “A growth stimulus is needed for IGF-1 to induce skeletal muscle hypertrophy in vivo.” 2010. https://journals.biologists.com/jcs/article/123/6/960/31470
– PubMed meta-analysis: Tesamorelin body composition in HIV-associated lipodystrophy. https://pubmed.ncbi.nlm.nih.gov/41545261/
– WADA 2026 Prohibited List. https://www.wada-ama.org/en/prohibited-list
– FDA bulk drug substances under 503A. https://www.fda.gov/drugs/human-drug-compounding/bulk-drug-substances-used-compounding-under-section-503a-fdc-act
– Frontiers in Physiology: Collagen type I in skeletal muscle after resistance training (2026). https://www.frontiersin.org/journals/physiology/articles/10.3389/fphys.2026.1839695/full
– Sermorelin cost guide, Ivy Rx. https://www.ivyrx.com/blog/sermorelin-cost
– Defy Medical peptide therapy. https://www.defymedical.com/peptide-therapy
– Innerbody CJC-1295 + Ipamorelin guide 2026. https://www.innerbody.com/cjc-1295-and-ipamorelin
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.