Last updated 18 June 2026. Educational content, not medical advice. TB-500 has not been FDA-approved for any indication. Speak with a licensed clinician before considering any peptide therapy.
Short answer: TB-500 is a synthetic 7-amino-acid fragment (Ac-LKKTETQ-OH) taken from the actin-binding region of thymosin beta-4, a naturally occurring 43-amino-acid protein found in nearly every human cell. It is studied for tissue repair, angiogenesis, and anti-inflammatory effects, mainly in animal models. As of June 2026, zero completed human efficacy trials exist for the TB-500 fragment specifically, and its regulatory status is in active flux: removed from the FDA’s Category 2 ban list in April 2026, but not yet formally permitted for compounding.
Thymosin beta-4 shows up in nearly every cell in your body. See what your own bloodwork says before experimenting with fragments. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
What exactly is thymosin beta-4, and why does TB-500 only cover part of it?
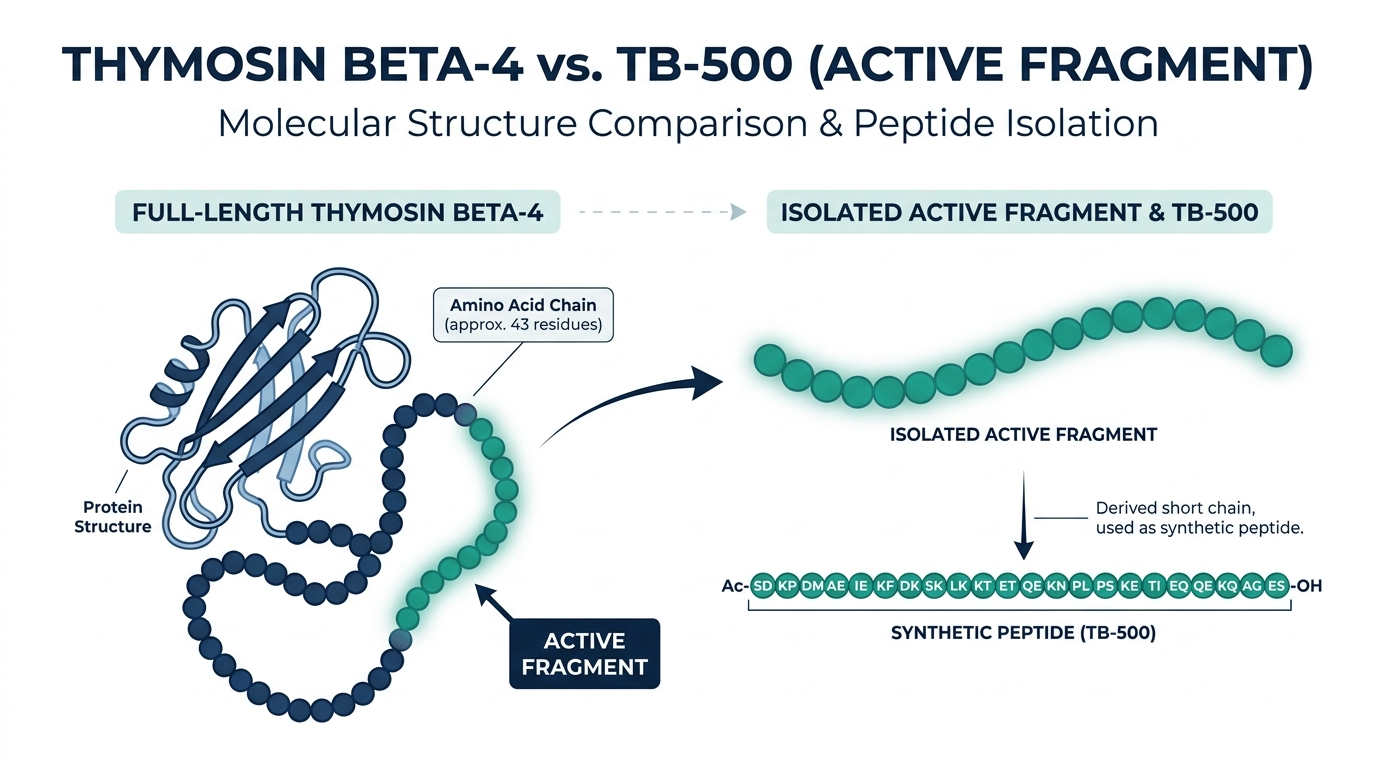
To understand TB-500 you have to start with the parent molecule. Thymosin beta-4 (Tβ4) is a 43-amino-acid protein the thymus gland produces in large quantities during fetal development, and that persists at lower concentrations in virtually every nucleated cell throughout life. Its main job is managing actin, the structural protein your cells use for movement, division, and shape-maintenance. Think of actin as a city’s road network: Tβ4 is the traffic controller that determines which roads get opened or closed.
TB-500 is not thymosin beta-4. It is a synthetic heptapeptide covering only residues 17 through 23 of the full sequence, with an N-terminal acetyl group added to improve chemical stability. That seven-amino-acid stretch is the actin-binding domain, the single region researchers first identified as responsible for Tβ4’s cell-migration effects. The idea was to isolate the functional core, make it easier and cheaper to synthesize, and improve bioavailability compared to the full molecule.
The important caveat: a 2015 study on cardiac tissue identified the C-terminal AGES domain of Tβ4 as the primary driver of post-ischemic heart benefit, a region TB-500 does not contain at all (PubMed). This single finding explains why you cannot simply assume the fragment replicates the full molecule’s biology.
How does TB-500 work at the cellular level?
The simplest way to actually get this done
Superpower is a full-body lab membership that runs 100+ biomarkers, has each result reviewed by a doctor, and tracks your numbers year over year (about $199/year). It is what we point readers to when they would rather get one clean, complete draw than chase single tests one at a time. Here is superpower reviewed in full.
The mechanism starts with G-actin, the globular, unpolymerized form of actin that sits in reserve inside a resting cell. When a cell needs to move (toward a wound, an area of inflammation, or a site of new blood vessel formation) it polymerizes G-actin into F-actin filaments that push out the cell’s leading edge like a tiny locomotive.
TB-500 binds to G-actin and sequesters it, modulating the speed and direction of that polymerization process. The downstream effects observed in animal research include:
- Accelerated cell migration: endothelial cells and fibroblasts move faster toward injury sites, shortening the early inflammatory phase of healing.
- Angiogenesis: TB-500 directly upregulates vascular endothelial growth factor (VEGF) expression, promoting formation of new capillaries that bring oxygen and nutrients to damaged tissue (Peptidepedia).
- Reduced fibrous scar tissue: by accelerating the organized repair phase, animal models show less disorganized collagen deposition than untreated wounds.
- Anti-inflammatory signaling: systemic reduction in pro-inflammatory cytokines, though the exact pathways in humans remain unconfirmed.
- Stem cell mobilization: some in-vitro evidence suggests Tβ4 fragments can signal resident stem cells in muscle and cardiac tissue, though this is the least-understood mechanism.
The key word in all of that is “animal models.” The mechanism is plausible and internally consistent. The translation to humans using the isolated TB-500 fragment has not been demonstrated in a controlled trial as of April 2026.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
What does the research actually show, and what does it not?
This is where the community conversation and the actual science diverge most sharply, and it is worth being direct about the gap.
What the research shows:
Animal wound-healing studies are the strongest data. One oft-cited study found that TB-500-treated cutaneous wounds showed 42% improved healing status versus saline controls by day four, and 61% better healing by day seven (Medical Anti-Aging white paper, August 2024). Cardiac research in murine (mouse) models has shown Tβ4 reducing cardiomyocyte apoptosis and improving left ventricular function after induced myocardial infarction (PMC). Stroke models show improved long-term neurological functional recovery. Across all these models the safety profile in animals has been consistently unremarkable, meaning no notable adverse events.
The human data:
The only completed human trials used full-length thymosin beta-4, not the TB-500 fragment. A Phase 2 randomized controlled trial in dry-eye disease (2015, 9 patients) found 59.1% reduction in corneal staining with statistical significance (p = 0.0108). A Phase 3 follow-up in neurotrophic keratopathy (2022, 18 patients) missed its primary endpoint: 60% versus 12.5% responder rate produced a p-value of 0.0656, falling just short of significance. There are zero completed human efficacy trials for TB-500 (the 17-to-23 fragment) published as of April 2026, per a systematic review by Superpower. A trial is registered under NCT07487363 but has not yet reported results.
What that means practically:
Every claim you read about TB-500 healing tendons, accelerating surgery recovery, or repairing cardiac tissue in humans is extrapolated from animal data on a related but not identical molecule. That does not make the mechanism implausible. It means no one has yet done the controlled human trial to confirm the extrapolation holds. Personally, I think the actin-binding mechanism is one of the more convincing peptide rationales out there, but a convincing mechanism and a proven clinical outcome are not the same thing, and conflating them is how people make bad health decisions.
The gap matters more than usual here for two reasons that rarely make it into the marketing. First, this is a fragment, not the parent protein, and the cardiac data specifically pins the biggest benefit on a region the fragment does not contain. So even a perfect translation of the animal work would not necessarily carry over to the seven-amino-acid version people actually buy. Second, animal healing studies use controlled doses, defined purity, and a known route of delivery. A grey-market vial gives you none of those, so you are not even reproducing the conditions that produced the encouraging rodent results. Extrapolating from a clean lab study to a mystery vial in your fridge is two leaps, not one.
What do people actually use TB-500 for?
In practice, the community uses TB-500 primarily as a recovery accelerant for soft-tissue injuries. The target conditions that come up most consistently in clinical discussions and community reports include:
| Injury Type | Animal Evidence | Human Evidence |
|---|---|---|
| Cutaneous wounds | Strong (42% faster healing day 4) | None for fragment |
| Tendon and ligament tears | Moderate (rodent models) | None |
| Muscle strain/tears | Moderate (actin mechanism plausible) | None |
| Cardiac tissue post-MI | Moderate (Tβ4 in porcine model) | Phase 2 mixed (full molecule) |
| Corneal / dry-eye disease | Moderate | Phase 2/3 (full molecule, mixed results) |
| Neurological recovery | Early-stage animal data | None |
The most common real-world use is stacking TB-500 with BPC-157, the combination sometimes marketed as the “Wolverine Blend.” The rationale is that BPC-157 supports local tissue repair via growth-factor modulation, while TB-500 provides the systemic angiogenesis and cell-migration signal. Whether that synergy holds in humans is, again, unproven, but the combination has the deepest community history of the popular research-peptide stacks.
Do not believe the marketing framing that TB-500 is “what athletes use.” It is banned under the WADA Prohibited List, Section S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics), both in-competition and out-of-competition, and has been explicitly prohibited since the 2018 update to the List (BSCG). Any professional athlete using it is violating anti-doping rules.
Is TB-500 legal in 2026?
The regulatory picture for TB-500 is genuinely complicated right now, and it changed three times in eighteen months.
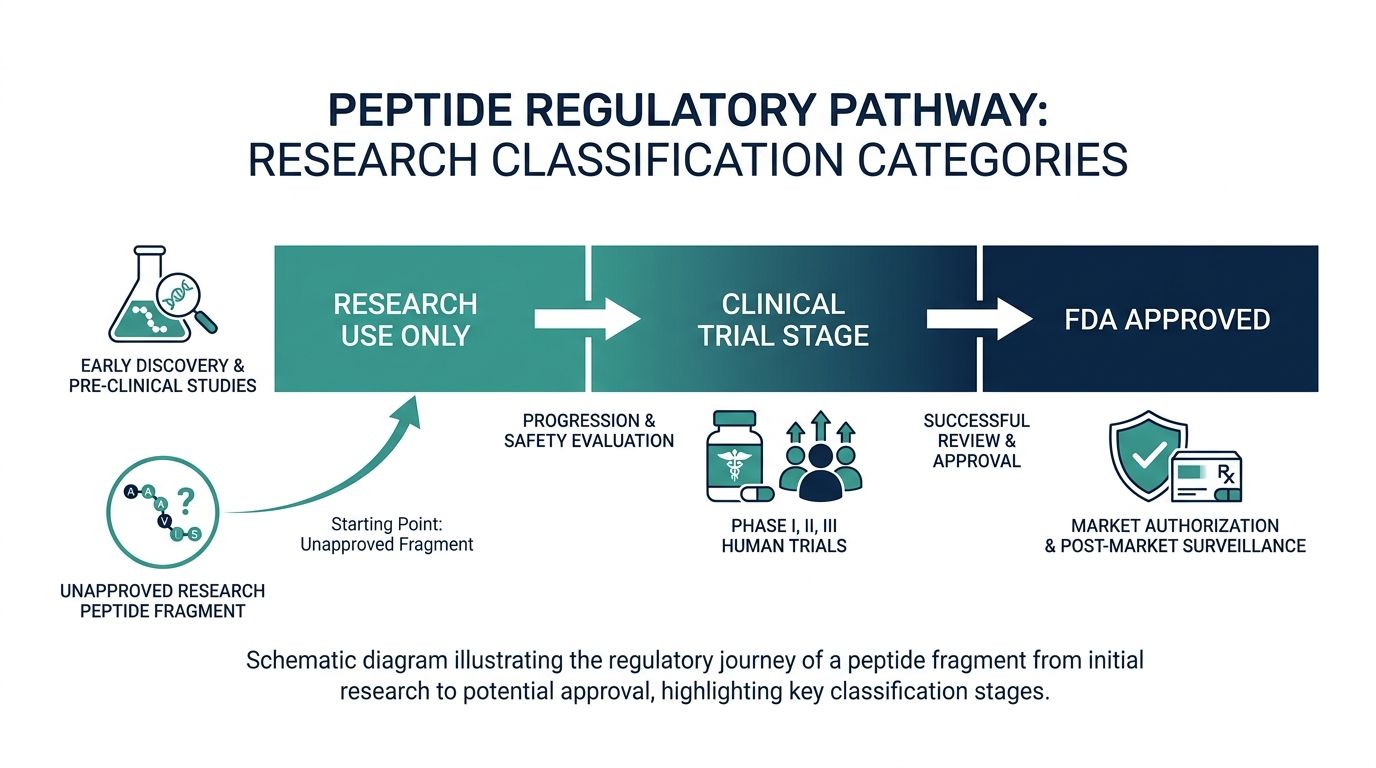
November 2023: The FDA placed TB-500 on its 503A Category 2 list, designating it as a bulk drug substance that “may present significant safety risks.” This effectively prohibited U.S. compounding pharmacies from including it in preparations for patients.
February 27, 2026: HHS Secretary Robert F. Kennedy Jr. announced that approximately 14 peptides would be moved from Category 2 back toward Category 1 permitted status. TB-500 was explicitly named among the 14 (Meto.co). Kennedy stated the original Category 2 classifications “were made without legitimate safety signals.”
April 2026: The FDA formally withdrew TB-500 from Category 2, removing the explicit prohibition. However, removal from Category 2 is not the same as placement on Category 1. TB-500 currently sits in a regulatory grey zone: no longer banned from compounding, but not yet explicitly permitted.
July 23 to 24, 2026: The Pharmacy Compounding Advisory Committee (PCAC) has a scheduled meeting to review TB-500 (free base) and TB-500 acetate as bulk drug substances nominated for the 503A Bulks List (FDA advisory committee calendar). The PCAC meeting is the formal step before a final Category 1 ruling.
The bottom line for 2026: TB-500 is not FDA-approved as a finished drug for any indication. Under WADA rules it is prohibited for athletes. For civilians, the research-chemical route remains in the same legal limbo as most grey-market peptides, and the licensed compounding route is pending the July PCAC decision. The safe lane is opening; it just has not fully opened yet.
Telehealth GLP-1 program with provider visits and pharmacy coordination.
How is TB-500 different from BPC-157?
These two peptides dominate the soft-tissue recovery conversation, and they are commonly stacked, so the comparison is worth making clearly.
| Feature | TB-500 | BPC-157 |
|---|---|---|
| Origin | Synthetic fragment of endogenous Tβ4 | Synthetic fragment of gastric juice protein BPC |
| Size | 7 amino acids (Ac-LKKTETQ-OH) | 15 amino acids |
| Primary mechanism | Actin sequestration, VEGF upregulation | Nitric oxide pathway, growth factor interaction |
| Main research indication | Systemic tissue repair, angiogenesis | Local tissue repair, gut healing |
| Human trial data | None for fragment | None for injectable systemic use |
| WADA status | Banned (Section S2) | Banned (Section S2) |
| 2026 FDA Category | Removed from Cat. 2; pending Cat. 1 | Removed from Cat. 2 on April 22, 2026 |
| Stack compatibility | Frequently combined with BPC-157 | Frequently combined with TB-500 |
The practical difference is about scope: BPC-157 is described as more locally acting, with particular affinity for connective tissue and gut lining repair. TB-500’s mechanism is more systemic, affecting cell migration and vessel growth across a broader tissue range. Neither claim has been rigorously confirmed in human trials.
What is the TB-500 experience timeline in the community?
This section describes what researchers and community members report, not a clinical protocol. No injection protocol information is provided here.
The most consistent pattern in community self-reports describes effects arriving in two phases. Inflammatory symptoms around an injury (swelling, heat, restricted range of motion) are often the first thing to shift, typically within the first two to three weeks of use. The structural repair signal, meaning actual tendon or ligament function improvement, is reported later, around weeks six to ten, which aligns with the biological timeline of collagen remodeling in soft tissue.
The reason TB-500 is almost never used alone is precisely this timeline. BPC-157 is perceived to have a faster local effect, while TB-500 is viewed as the systemic amplifier. Cycles of three months on, followed by a break of four to six weeks, are the most common pattern discussed. Personally, the fact that the community has converged on longer cycles and lower frequency suggests the more credible reports come from people who understood it is not a rapid-result compound.
What are the real risks of TB-500?
The risk conversation for TB-500 breaks into two separate issues that tend to get conflated.
Risk from the molecule itself: Animal safety data has been consistently clean. No serious adverse events attributable to TB4 or the fragment have been reported in the Phase 2 trials using the full molecule. The most commonly reported side effects in self-reporting communities are transient fatigue and injection-site irritation. Because no completed human trials exist for the fragment, longer-term or dose-dependent effects are genuinely unknown.
Risk from the supply chain: This is larger and more immediate than the molecular risk. TB-500 sold as “research use only” comes without a prescribing physician, without a licensed pharmacy, without batch-specific purity verification by a third party you can trust, and without any accountability if the vial contains something other than what the label says. Finnrick’s independent testing database, which as of mid-2026 spans more than 8,000 tests across 225 vendors, has found research peptides testing as low as 75% purity and occasionally confirmed as entirely mislabeled compounds (Finnrick). The molecule has a good safety record. The supply chain does not.
One genuine myth worth busting: TB-500 is not a steroid, it does not affect testosterone or estrogen, and it does not trigger the hormonal suppression effects associated with anabolic steroids. People conflate “injectable peptide” with “steroid” constantly. The biology is completely different.
Telehealth GLP-1 program with provider visits and pharmacy coordination.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
What TB-500 will not do
A lot of the disappointment around TB-500 comes from expectations the biology never supported. Being clear about the ceiling is as useful as describing the promise.
- It will not rebuild a fully torn tendon or ligament. A complete rupture is a structural problem, and no injectable peptide re-attaches torn tissue. If an orthopedist says you need repair, a peptide is not an alternative to that repair.
- It is not a painkiller. Any perceived pain relief is downstream of reduced inflammation, not a direct analgesic effect. Masking pain enough to train through a real injury is how a minor problem becomes a major one.
- It does not replace rehab. Tissue remodels along the lines of the load you place on it. Skipping the boring progressive loading and expecting a vial to do the work is the single most common way people waste both the money and the recovery window.
- It will not build muscle. TB-500 is a repair and migration signal, not an anabolic. It does not act like testosterone or a growth-hormone drug on muscle protein synthesis.
- It is not proven in humans. This is the honest ceiling on every claim above: the fragment has no completed human efficacy trial, so anyone using it is running an experiment on themselves.
If you are considering TB-500, what should you actually do?
This is educational, not a recommendation to use an unapproved compound. But if you are weighing it, the sensible sequence is not “find a vendor.” It is closer to this.
- Get a real diagnosis first. A nagging shoulder or knee deserves imaging and a clinician’s read before any peptide enters the picture. You cannot pick the right tool if you do not know whether the problem is a strain, tendinopathy, or a tear that needs surgery.
- Wait for the legal lane to actually open. TB-500 sits between Category 2 and Category 1, with a PCAC review scheduled. The difference between a licensed compounding pharmacy product and a grey-market research vial is verified identity, purity, and sterility. That gap is the whole safety story, so patience here is not caution for its own sake.
- Establish a baseline you can compare against. Before changing anything, a broad panel of your own bloodwork gives you a reference point. Without a baseline you cannot tell whether anything actually shifted, and self-reported “I feel better” is the weakest data there is.
- Insist on third-party testing. Independent databases have found research peptides testing well under label purity and occasionally mislabeled entirely. If a product has no batch-specific certificate of analysis from a lab you can verify, treat the contents as unknown.
- Bring a clinician into the decision. A sports-medicine or functional-medicine physician can weigh it against your actual injury, your history, and safer proven options like structured rehab, and can monitor you if you proceed.
The theme running through all five steps is the same one that runs through the whole article: the molecule has a reasonable safety record and a plausible mechanism, and the danger sits almost entirely in the unregulated supply chain and in skipping the diagnosis. Slowing down is the highest-leverage thing you can do.
Frequently asked questions
Is TB-500 the same as thymosin beta-4?
No. Thymosin beta-4 (Tβ4) is a naturally occurring 43-amino-acid protein. TB-500 is a synthetic 7-amino-acid fragment covering residues 17 to 23 of Tβ4, specifically its actin-binding domain. The two share a mechanism, but TB-500 is missing the C-terminal region of Tβ4 that animal studies suggest drives cardiac benefits.
Has TB-500 been tested in human clinical trials?
Not as the isolated fragment. The full-length thymosin beta-4 molecule has been studied in Phase 2 and Phase 3 trials for dry-eye disease and neurotrophic keratopathy. A trial registered for TB-500 (NCT07487363) has not yet published results. There are zero completed human efficacy trials for the TB-500 fragment specifically as of April 2026.
Is TB-500 legal to buy in the US in 2026?
It depends on the route. TB-500 was removed from the FDA’s Category 2 compounding ban in April 2026, but is not yet on the Category 1 permitted list. The PCAC meeting on July 23 to 24, 2026 is expected to address that. Buying it as a “research chemical” is legally ambiguous: legal to sell, not legal to use on yourself. It is banned under WADA for competitive athletes regardless of legal status.
What is TB-500 used for in research?
Wound healing, soft-tissue repair, angiogenesis, and anti-inflammatory effects are the core research areas. Cardiac repair was a significant area of interest but human trials of full-length Tβ4 in that indication produced mixed results. Neurological recovery is an earlier-stage research area.
Why is TB-500 always stacked with BPC-157?
The two compounds are believed to act on different parts of the repair process: BPC-157 through nitric oxide and local growth-factor pathways, TB-500 through systemic actin regulation and VEGF-driven angiogenesis. Stacking them is thought to provide broader coverage for soft-tissue recovery. The synergy is empirical, not studied in controlled trials.
Can athletes use TB-500?
No. Thymosin beta-4 and its derivatives, including TB-500, are explicitly named under Section S2 of the WADA Prohibited List and have been banned both in-competition and out-of-competition since the 2018 update. They are classified as non-Specified Substances, meaning there is no reduced sanction for inadvertent exposure.
How does TB-500 compare to a telehealth peptide prescription?
A research-chemical vial of TB-500 provides the molecule with no verification of purity, identity, sterility, or appropriate dose. A licensed telehealth clinic provides a physician’s assessment, a compounding pharmacy’s quality controls, baseline lab work, and structured follow-up. The telehealth route costs more, typically $199 to $399 a month for peptide therapy programs. It also includes everything the vial does not.
Does TB-500 build muscle?
No. TB-500 is studied as a tissue-repair and cell-migration signal, not an anabolic agent. It does not raise testosterone, does not directly stimulate muscle protein synthesis, and should not be thought of as a bodybuilding compound. Any strength benefit people attribute to it would come indirectly from recovering faster from an injury, not from the peptide building tissue on its own.
Will TB-500 show up on a drug test?
For athletes subject to anti-doping testing, yes, it is a prohibited substance under Section S2 of the WADA list and modern testing methods can detect peptide hormones and their markers. Standard employment drug screens do not look for it, but that is not the point. If you compete under any anti-doping code, using it is a violation regardless of whether a given test happens to catch it.
Is TB-500 safe?
The molecule itself has a clean animal safety record and no serious adverse events reported in the human trials of the full-length parent protein, with the most common complaints being mild fatigue and injection-site irritation. The larger and more immediate risk is the supply chain: an unregulated vial can be underdosed, mislabeled, or non-sterile. Long-term effects of the fragment in humans are simply unknown because the trials have not been done.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources:
– FDA Advisory Committee Calendar, PCAC July 23-24 2026
– FDA Bulk Drug Substances: 503A Category 2 List
– Superpower TB-500 Research Guide (April 2026)
– PubMed: Cardiac repair with thymosin β4 and cardiac reprogramming factors
– PMC: Thymosin beta-4 increases cardiac cell proliferation in porcine AMI model
– Medical Anti-Aging TB-500 Medical Evidence White Paper, August 2024
– BSCG: TB-500 Status, Risks, and Bans in Sport and Military
– Innerbody: TB4 and TB-500 Peptide Therapy (2026)
– Meto.co: 14 Peptides Legal Again 2026
– Finnrick Independent Testing Database
– ClinicalTrials.gov NCT07487363
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.