
You scanned your blood work, saw BUN and creatinine sitting in the normal column, and relaxed. Then your eye caught a third line you do not remember ordering: the BUN/creatinine ratio. No units, just a single number like 18 or 24, and no clear sense of whether that is good or bad. Here is what almost no one explains. That little ratio is one of the smartest clues on a basic metabolic panel, because it can tell your clinician whether a kidney number is off because of the kidney itself, or because of something happening upstream like dehydration.
The BUN/creatinine ratio decides whether it’s dehydration or something more. See your full kidney panel for clarity. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Most explainers stop at “it checks your kidneys.” That undersells it. The ratio is really a tiny piece of detective work, and once you understand it, you read your own panel with sharper eyes.
What is bun/creatinine ratio in blood test?
The BUN/creatinine ratio in a blood test is simply your blood urea nitrogen (BUN) divided by your serum creatinine, two waste products your kidneys filter out of your blood. BUN is the nitrogen left over when your body breaks down protein, and creatinine is the leftover from normal muscle metabolism (MedlinePlus). Both are cleared by your kidneys, so when kidney function or blood flow changes, the two numbers move, and the relationship between them tells a story that neither number tells alone.
In plain terms: BUN is sensitive to your hydration and protein status, while creatinine is steadier and tracks the kidney filter itself. Dividing one by the other is a clever way to separate “a hydration or flow problem” from “a kidney tissue problem.” That is the whole point of the ratio, and it is why understanding what bun/creatinine ratio means in a blood test is worth more than memorizing a single cutoff.

What does bun creatinine ratio mean in a blood test?
When people ask what does bun creatinine ratio mean on a blood test, the honest answer is that it is a direction-finder, not a diagnosis. The ratio compares how fast urea is building up versus how fast creatinine is building up. Because your kidneys handle these two molecules slightly differently, the ratio shifts depending on what is going wrong.
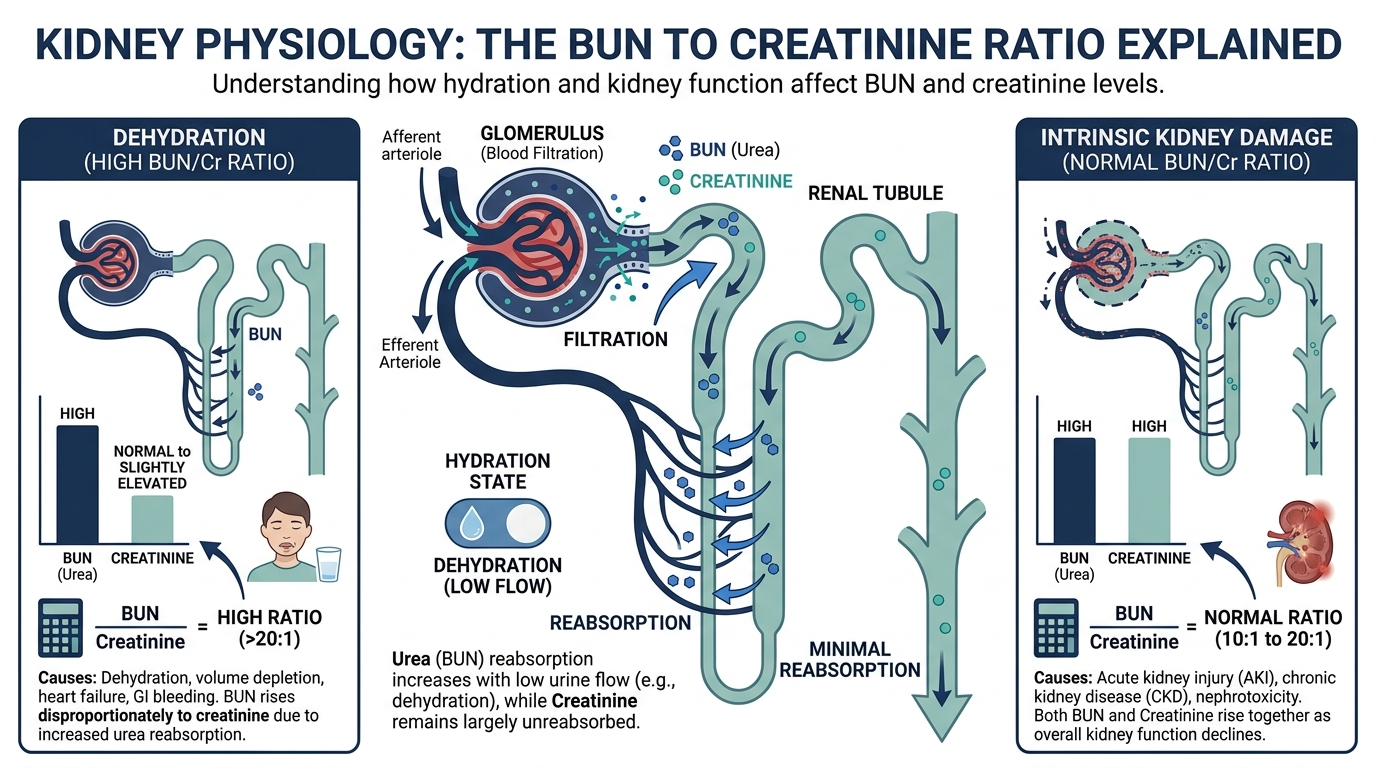
Here is the mechanism that makes it work. When blood flow to the kidneys drops, for example during dehydration, the tubules slow down and reabsorb extra water and sodium back into the body. Urea quietly hitches a ride and gets reabsorbed along with that water, while creatinine mostly does not (NCBI, Clinical Methods). So BUN climbs faster than creatinine, and the ratio rises. Knowing what bun/creatinine ratio means in a blood test really comes down to knowing that urea is the molecule that gets “stuck” when the kidneys are short on blood flow.
What is a normal BUN/creatinine ratio?
A normal BUN/creatinine ratio is generally considered to be in the neighborhood of 10:1 to 20:1, with a typical baseline sitting right around 10:1 (NCBI, Clinical Methods). The exact reference range can vary by lab, so the most reliable comparison is always the range printed next to your result.
It helps to anchor the ratio to the raw numbers behind it. Cleveland Clinic lists a normal BUN of about 8 to 24 mg/dL for adult men, 6 to 21 mg/dL for adult women, and 7 to 20 mg/dL for children (Cleveland Clinic). Both BUN and creatinine can sit inside their own normal ranges while the ratio still drifts high or low, which is exactly why the ratio is reported as its own line. The practical takeaway: a ratio comfortably between roughly 10 and 20 is the boring, reassuring zone.
What does a high BUN/creatinine ratio mean?
A high BUN/creatinine ratio, generally above about 20:1, most often points to a prerenal problem, meaning the kidneys themselves are fine but they are not getting enough blood flow (StatPearls, Prerenal Kidney Failure). The kidney is structurally healthy; the issue is upstream. This is why a high ratio so often boils down to a short, common list:
- Dehydration. The single most common reason for a mildly elevated ratio. Low fluid volume means more urea gets reabsorbed, pushing BUN and the ratio up.
- Reduced blood flow to the kidneys, as in congestive heart failure or significant blood loss, which the body responds to the same way it responds to dehydration.
- Gastrointestinal bleeding. Blood in the gut is digested like a high-protein meal, generating a surge of urea and selectively raising BUN (NCBI, Clinical Methods).
- A high-protein diet or steroid medications, which increase urea production without touching creatinine much.
Here is the insider point that rarely reaches the patient version. Clinicians use the ratio as a first pass to tell a kidney that is merely thirsty from a kidney that may actually be damaged. The classic rule of thumb: a ratio above 20:1 leans prerenal, where blood flow is the problem, while a ratio closer to 15:1 is more typical of acute tubular necrosis, where the tubules are genuinely injured (StatPearls, Prerenal Kidney Failure). But here is the honest caveat most patient explainers skip. When researchers actually tested the BUN to creatinine ratio in emergency department patients, it did a poor job of separating prerenal from intrinsic acute kidney injury on its own (PMC, BUN to creatinine ratio in AKI). So the ratio is a useful nudge, not a verdict. It can hint at “drink more water and recheck” versus “we need to investigate the kidney itself,” but only alongside the rest of the picture.

What does a low BUN/creatinine ratio mean?
A low BUN/creatinine ratio, generally below about 10:1, usually reflects something reducing your urea levels rather than a kidney filter problem. Because creatinine stays relatively steady, the ratio drops when BUN falls for its own reasons (NCBI, Clinical Methods).
The common explanations are reassuring or, at most, point elsewhere in the body:
- Low protein intake or malnutrition, since less dietary protein means less urea to produce.
- Advanced liver disease, because the liver is where urea is made, so a struggling liver produces less of it (NCBI, Clinical Methods).
- Overhydration, which dilutes BUN, and pregnancy, which increases urea clearance.
On its own, a low ratio is rarely an emergency, but it is a nudge to look at protein status and liver health rather than the kidneys.
Why is BUN read together with creatinine in the first place?
BUN and creatinine are paired because each one covers the other’s blind spot. Creatinine is the more dependable marker of the kidney filter itself, but it is slow to move and can stay normal until a fair amount of function is lost. BUN moves faster and is more sensitive, but it is also “noisy,” swinging with diet, hydration, bleeding, and liver function (NCBI, Clinical Methods).
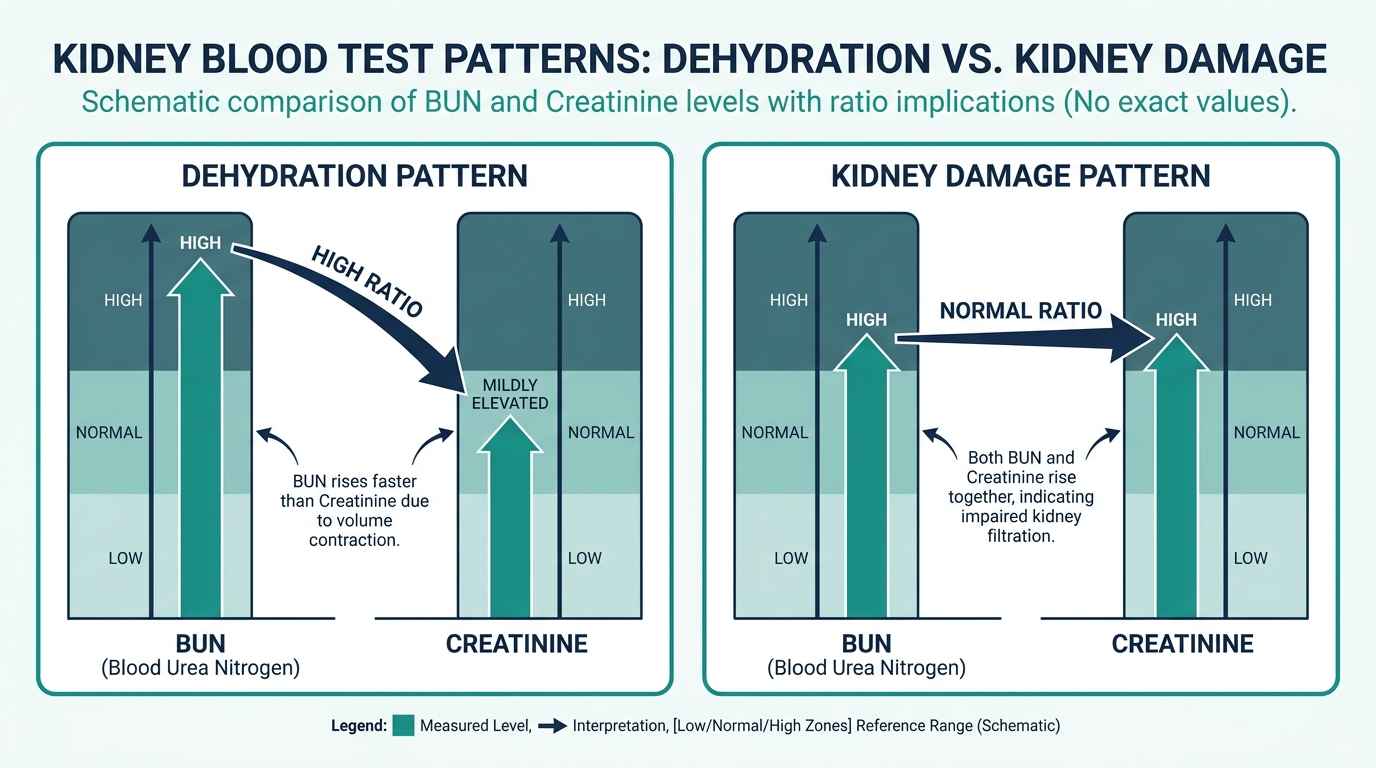
Reading them as a ratio turns that noise into signal. Think of creatinine as the steady anchor and BUN as the sensitive antenna. When the antenna jumps but the anchor barely moves, the cause is usually outside the kidney, such as dehydration or a high-protein load. When both rise together in proportion, the suspicion shifts toward the kidney tissue itself (Cleveland Clinic). That is the elegant trick of the ratio: it uses two imperfect numbers to triangulate a better answer than either could give alone.
The part most people never hear: the ratio is a snapshot, not a verdict
This is where the BUN/creatinine ratio earns both respect and caution. It is genuinely useful, but it is fragile, and that fragility is the most underappreciated thing about it. The ratio can swing simply because you skipped fluids before your draw, ate a steak the night before, or took a steroid that week. None of those mean your kidneys are failing.
That is why clinicians treat the ratio as a hypothesis generator rather than a diagnosis. Research on the BUN to creatinine ratio in acute kidney injury shows it performs best as part of a fuller picture, alongside the trend in your creatinine over time, your symptoms, and other tests, not as a single magic number (PMC, BUN to creatinine ratio in AKI). A one-time elevated ratio in an otherwise well person who came in dehydrated is a very different thing from a climbing ratio in someone with worsening creatinine. The smartest way to use your own result is to ask not just “is it high or low,” but “compared to what, and on what kind of day.” One number on one morning rarely tells the whole story, and that humility is exactly what separates a useful reading from an anxious one.

How to prepare, and what tilts the ratio on the day of your draw
Because the BUN half of this ratio is so sensitive to short-term factors, how you show up for the blood draw can move the number without anything being wrong with your kidneys. Understanding these levers is the difference between an anxious reading and a calm one.
- Hydration. The biggest single factor. Arriving dehydrated concentrates urea and pushes the ratio up, while being well hydrated keeps it in the reassuring middle. A high ratio in someone who skipped fluids on a hot morning often normalizes after they drink and get rechecked.
- Protein intake the day before. A large steak dinner or a high-protein regimen raises urea production and can nudge BUN and the ratio upward, since dietary protein is the raw material for urea.
- Certain medications. Corticosteroids and some other drugs increase urea production or shift kidney handling. Tell your clinician what you take, including supplements.
- Recent gastrointestinal bleeding. Blood in the gut is digested like a protein meal, generating a surge of urea that selectively raises BUN and the ratio.
Many BUN and creatinine draws come inside a metabolic panel that may require fasting for the glucose or lipid components, so follow whatever instruction your lab gives. The larger point is that a single out-of-range ratio in an otherwise well person deserves the question, was I dehydrated or did I eat a big protein meal, before it earns any worry.
The ratio inside the full kidney picture
The BUN/creatinine ratio is one clue among several the kidney workup provides. Reading it beside its companions is what turns a hint into a direction.
| Marker or test | What it adds |
|---|---|
| eGFR (estimated glomerular filtration rate) | The best everyday estimate of overall kidney filtering capacity, calculated from creatinine. |
| Creatinine trend over time | A rising creatinine across successive draws is a stronger signal of real kidney injury than any single ratio. |
| Electrolytes (sodium, potassium) | Shift with dehydration and kidney dysfunction, helping frame the cause. |
| Urinalysis | Protein, blood, or casts in the urine point toward intrinsic kidney disease rather than a flow problem. |
| Urine sodium and fractional excretion | Help separate a prerenal state from tubular injury more reliably than the blood ratio alone. |
The most important companion is the creatinine trend. A single elevated ratio in a well, dehydrated person is a very different situation from a ratio that is high while creatinine is climbing week over week. When the urinalysis is clean and eGFR is stable, a high ratio most often means a flow or hydration problem. When the urine shows protein or the eGFR is falling, attention shifts to the kidney tissue itself.
Worked examples: how clinicians reason through the ratio
The ratio only makes sense in context. These scenarios show why the same number can mean different things.
Scenario one: ratio of 25:1, normal creatinine, and you arrived thirsty. A classic prerenal pattern from dehydration. The kidney is fine, blood flow is low, and urea is being reabsorbed. Rehydrate, recheck, and it usually settles.
Scenario two: ratio around 12:1 but both BUN and creatinine rising together. The proportional rise points away from a pure flow problem and toward the kidney tissue itself, such as tubular injury. This calls for a closer look rather than reassurance.
Scenario three: ratio of 30:1 with black, tarry stools. A high ratio plus signs of gastrointestinal bleeding is a recognized combination, because digested blood floods the system with urea. The bleeding, not the kidney, is the headline.
Scenario four: ratio of 8:1 in someone eating very little protein. A low ratio from reduced urea production, not a kidney filter problem. Attention turns to nutrition, and sometimes to the liver where urea is made.
Scenario five: a normal ratio but a quietly falling eGFR over a year. The ratio reassures while the trend warns. This is why the ratio is never read alone, and why the creatinine and eGFR trajectory matter more for detecting slow kidney decline.
Symptoms and red flags worth knowing
The ratio itself is silent, and mild kidney trouble often produces no symptoms at all, which is exactly why blood testing catches it. When symptoms do appear, they are worth recognizing.
- Signs of dehydration: intense thirst, dark and scanty urine, lightheadedness on standing, and a dry mouth. These fit a high, prerenal ratio.
- Signs that warrant prompt attention: markedly reduced urination, swelling in the legs or around the eyes, unusual fatigue or confusion, nausea, and shortness of breath, which can accompany failing kidney function.
- Signs of gastrointestinal bleeding: black tarry stools, vomiting blood, or new severe fatigue, which pair with a high ratio and need urgent evaluation.
A single abnormal ratio with none of these symptoms, in a person who was simply dehydrated, is usually low stakes. The same ratio alongside reduced urination, swelling, or bleeding is a reason to act quickly.
Who should track the ratio, and how often
BUN, creatinine, and their ratio arrive automatically on most basic and comprehensive metabolic panels, so the general population gets periodic exposure. Closer attention is warranted in specific groups.
- People with kidney disease or risk factors. Diabetes, high blood pressure, and heart failure raise kidney risk, so these numbers are followed on a schedule the clinician sets.
- People on medications that affect the kidneys or fluid balance. Diuretics, some blood pressure drugs, and certain painkillers can shift the ratio, warranting monitoring.
- Anyone acutely ill with vomiting, diarrhea, or poor intake. Here the ratio helps gauge dehydration and flow to the kidneys.
- Hospitalized patients. The ratio and the creatinine trend are watched closely to catch acute kidney injury early.
The right interval depends entirely on the reason. A one-off high ratio from dehydration needs only a hydrated repeat. A value tied to chronic kidney disease follows that condition’s monitoring cadence, with the creatinine trend carrying the most weight.
Common misconceptions about the BUN/creatinine ratio
This ratio is easy to over-read because it looks precise. Correcting the frequent errors makes it far more useful and far less frightening.
- “A high ratio means my kidneys are damaged.” Usually the opposite. A high ratio most often means the kidneys are healthy but under-perfused, classically from dehydration, and it resolves with fluids.
- “The ratio alone can diagnose the problem.” It cannot. Research shows the blood ratio does a poor job on its own of separating a flow problem from real kidney injury, so it is read with the creatinine trend, urinalysis, and eGFR.
- “A normal ratio means my kidneys are definitely fine.” Not necessarily. Kidney function can decline slowly with a normal ratio, which is why the creatinine and eGFR trajectory matter more for catching chronic decline.
- “My diet cannot affect a kidney test.” It can. A high-protein meal raises urea and nudges the ratio up, and low protein intake pulls it down, all without any change in kidney health.
- “One abnormal result means I need to worry.” Rarely, on its own. The ratio is a snapshot sensitive to the kind of day you had, so the trend and the surrounding picture matter far more than a single morning’s number.
Curious where your bun/creatinine ratio really sits?
Baseline bun/creatinine ratio and 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
What is a normal BUN/creatinine ratio?
A normal BUN/creatinine ratio generally falls in the range of about 10:1 to 20:1, with a typical baseline near 10:1 (NCBI, Clinical Methods). Ranges vary slightly by lab, so compare your result to the reference range printed on your own report.
What does a high BUN/creatinine ratio mean?
A ratio above about 20:1 most often points to a prerenal cause, meaning the kidneys are healthy but not getting enough blood flow, classically from dehydration, heart failure, or gastrointestinal bleeding (StatPearls, Prerenal Kidney Failure). It is a clue, not a diagnosis.
What does a low BUN/creatinine ratio mean?
A ratio below about 10:1 usually reflects low urea production rather than a kidney filter problem, often from low protein intake, malnutrition, overhydration, or advanced liver disease (NCBI, Clinical Methods).
Can the BUN/creatinine ratio be off if my kidneys are fine?
Yes. Dehydration, a high-protein meal, certain medications, and GI bleeding can all raise the ratio even when the kidneys are structurally healthy, which is exactly why a prerenal pattern is so common (NCBI, Clinical Methods).
Should I worry if my BUN/creatinine ratio is abnormal?
Not from one result alone. The ratio is best read alongside your creatinine trend, hydration status, symptoms, and other tests, not as a standalone verdict (PMC, BUN to creatinine ratio in AKI). Discuss any abnormal result with your clinician.
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


