
You scanned your comprehensive metabolic panel, saw your cholesterol and glucose, and then near the bottom you hit a line that read something like “A/G ratio 1.6” with no flag next to it. Most people skip right over it. That is a mistake. The A/G ratio is one of the cheapest, most overlooked clues on your report, and it quietly tells your doctor how your liver, kidneys, immune system, and nutrition are doing all at once.
An A/G ratio without context is just a number. Want to see what’s actually driving it? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
The number itself is almost embarrassingly simple. It is one type of protein divided by another. But the story behind that simple division is where it gets interesting, and understanding it changes how you read the whole protein section of your bloodwork.
What is the a/g ratio blood test?
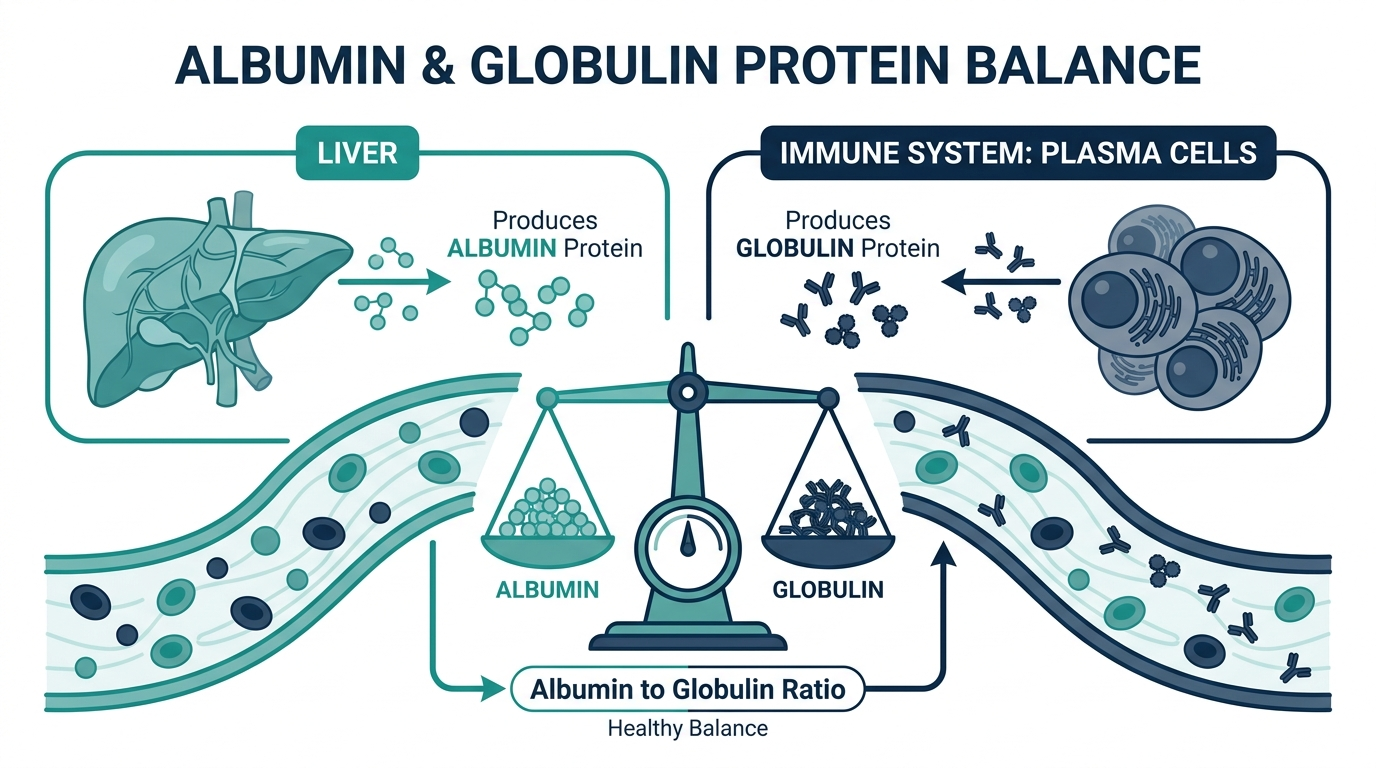
The a/g ratio blood test reports the ratio of albumin to globulin, the two main families of protein in your blood. It is not a separate blood draw. It is calculated automatically from a total protein test, usually part of a comprehensive metabolic panel, by dividing your albumin level by your globulin level (MedlinePlus). Albumin is made by your liver and is the most abundant protein in blood. Globulins are a mixed group made by your liver and immune system that fight infection, carry substances, and help blood clot (Cleveland Clinic).
In plain terms: the lab measures your total protein, splits it into albumin and globulin, and the A/G ratio tells you which side is winning. A healthy body keeps slightly more albumin than globulin, so a normal ratio sits a little above 1.

What is the a/g ratio in a blood test actually measuring?
It is measuring the balance between your “housekeeping” protein and your “defense and transport” proteins. Albumin is the workhorse that keeps fluid inside your blood vessels and ferries hormones, vitamins, and enzymes around the body (MedlinePlus). Globulins, which make up roughly 40 percent of your blood protein, include the antibodies and clotting factors your immune system relies on (Cleveland Clinic).
When you understand that the A/G ratio is a balance, the rest falls into place. The ratio can shift because albumin dropped, because globulin rose, or because both moved at once. That is exactly why doctors do not read the ratio alone. They read it alongside the individual albumin and globulin values and your total protein, because a ratio of 1.0 caused by low albumin is a very different problem from a ratio of 1.0 caused by high globulin.
What is a normal a/g ratio in a blood test?
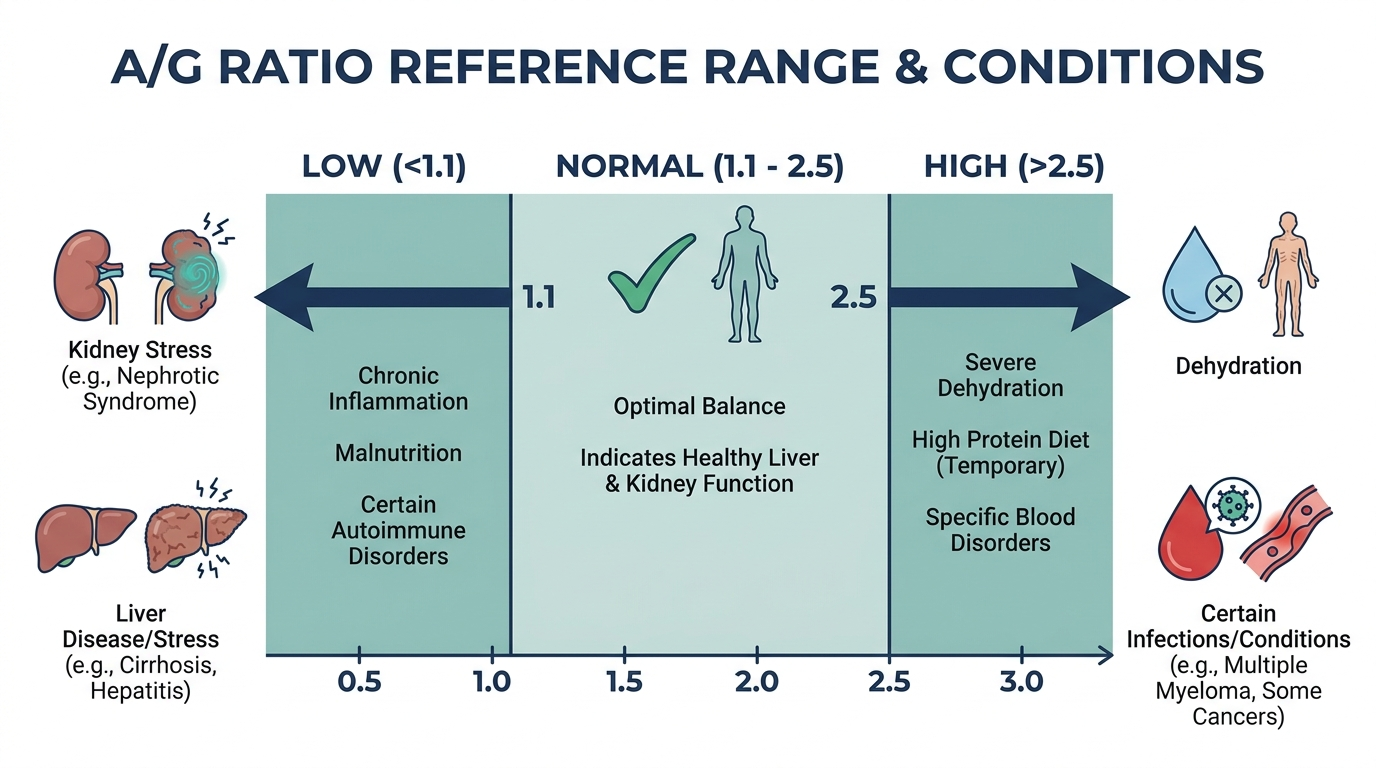
A normal A/G ratio is slightly more than 1, which simply means you have a bit more albumin than globulin in your blood (Cleveland Clinic). The ratio is built from these typical adult component ranges reported by Cleveland Clinic: total protein 6.3 to 8.0 g/dL, albumin 3.9 to 4.9 g/dL, and globulin 2.0 to 3.5 g/dL (Cleveland Clinic).
Run the math on those numbers and you can see why most healthy people land somewhere in the range of about 1.1 to 2.2. The exact cutoff varies slightly by laboratory and instrument, and hydration can nudge it, so the single most useful habit is to read your result against the reference range printed on your own report. That is the range your lab actually calibrated for the way it runs the test.
What does a low a/g ratio mean?
A low A/G ratio most often reflects low albumin, high globulin, or both, and it is the side of the ratio that tends to matter more clinically (MedlinePlus). A low ratio can point to a short list of recognizable patterns:
- Liver disease. A damaged liver makes less albumin, which drags the ratio down. Cirrhosis is a classic cause of a low A/G ratio (MedlinePlus).
- Kidney disease. Damaged kidneys can leak albumin into the urine, lowering blood albumin and the ratio with it (MedlinePlus).
- Autoimmune disease such as lupus. Chronic immune activation raises globulin, which pushes the ratio down (MedlinePlus).
- Multiple myeloma. This blood cancer floods the blood with abnormal globulin proteins, a high total protein with a low A/G ratio that often prompts further testing (Cleveland Clinic).
- Malnutrition, malabsorption, or inflammation, all of which can lower albumin (MedlinePlus).
None of these is diagnosed by the ratio alone. A low A/G ratio is a tripwire that tells your clinician where to look next, not a verdict.

What does a high a/g ratio mean?
A high A/G ratio most often reflects low globulin rather than unusually high albumin (MedlinePlus). It is generally a less common finding than a low ratio, and it can point to certain genetic disorders that affect how the body makes immune proteins, or to some forms of leukemia, a cancer of the blood cells (Cleveland Clinic).
Because a high ratio usually traces back to low globulin, the follow-up question your doctor asks is why globulin is low. That can mean reduced antibody production or an underlying immune issue. As with a low ratio, a single high A/G value is a reason to look closer, not a reason to panic.
Why is the a/g ratio reported with total protein and albumin?
Because the ratio is meaningless without the parts that build it. The A/G ratio is calculated from total protein and albumin, with globulin derived by subtracting albumin from total protein, so the three numbers are read as a set (MedlinePlus). Total protein tells you the overall amount, albumin tells you the liver and nutrition side, and the ratio tells you the balance.
Here is a simplified version of how clinicians combine them:
- Low A/G with high total protein: raises suspicion of excess globulin, which can occur in multiple myeloma or chronic inflammation (Cleveland Clinic).
- Low A/G with low total protein: points more toward low albumin from liver disease, kidney loss, or malnutrition (MedlinePlus).
- High A/G ratio: usually reflects low globulin, prompting questions about immune protein production (Cleveland Clinic).
- Normal A/G with normal total protein: the reassuring baseline most people see.
This is why the ratio earns its place on the panel. One cheap division flags whether the imbalance is coming from the albumin side or the globulin side, and that fork sends your workup down two very different paths.
The part most people never hear: a low A/G ratio and long-term risk
This is where the A/G ratio quietly graduates from a routine line item to something worth tracking over the years. Beyond diagnosing a specific illness, a persistently low albumin-to-globulin ratio has emerged in research as an independent prognostic marker, meaning it predicts outcomes even after accounting for other factors.
The signal shows up across very different cancers. In patients with metastatic non-small-cell lung cancer, a low A/G ratio below 1.12 was an independent predictor of shorter progression-free and overall survival (PubMed, A/G ratio in metastatic NSCLC). In gastric cancer patients treated with curative surgery, a low preoperative A/G ratio tracked with worse five-year survival, 64.8 percent versus 84.0 percent for the high-ratio group, and a higher recurrence rate (PMC, A/G ratio in gastric cancer).
Why would one protein ratio carry that kind of weight? The leading explanation is that a low A/G ratio is a quiet readout of two bad things happening together: chronic inflammation drives globulin up while poor nutrition and illness drive albumin down. The ratio captures both in a single inexpensive number. To be clear, your A/G ratio is not a cancer screening test, and an isolated low value in an otherwise healthy person usually traces back to something benign like mild inflammation or hydration. But it explains why a doctor reading your panel does not just glance at this line and move on. It is a sensitive, cheap mirror of how much background stress your body is carrying.

Globulins are not one protein: the fractions behind the number
Part of why the A/G ratio can point to so many different problems is that “globulin” is not a single molecule. It is an umbrella covering several protein families with very different jobs. When a doctor needs to know which globulins are driving an abnormal ratio, a follow-up test called serum protein electrophoresis (SPEP) separates them into bands, and understanding those bands demystifies the whole panel (American Family Physician).
- Alpha-1 and alpha-2 globulins are largely acute phase reactants, proteins that rise with inflammation, infection, or malignancy. A jump in these fractions is a signal of active inflammation somewhere in the body (American Family Physician).
- Beta globulins include transferrin, the iron-carrying protein, so this fraction connects your protein panel to your iron status.
- Gamma globulins are predominantly your antibodies, the immunoglobulins. A broad, diffuse rise here suggests chronic inflammation or infection, while a single sharp spike, called a monoclonal spike, is the pattern that raises concern for multiple myeloma (American Family Physician).
This is the mechanism behind the earlier warning that a low A/G ratio with high total protein deserves a closer look. The electrophoresis distinguishes a benign, broad increase in antibodies from a worrisome single-clone spike. The A/G ratio flags that something is off in the protein balance, and SPEP tells you which fraction is responsible.
Why albumin falls: the four mechanisms worth knowing
Because the albumin side of the ratio is usually the more clinically important one, it helps to understand the small number of ways albumin actually drops. Nearly every cause fits into one of four buckets, and matching your situation to a bucket makes an abnormal result far less mysterious.
- The liver makes less of it. Albumin is manufactured entirely by the liver, so chronic liver disease like cirrhosis reduces production and lowers the ratio (MedlinePlus).
- The kidneys leak it out. Healthy kidneys keep albumin in the blood. When the filtering units are damaged, albumin spills into the urine, a hallmark of nephrotic syndrome, and blood levels fall (MedlinePlus).
- You are not building it. Poor protein intake, malabsorption in the gut, or severe illness leaves the body short on the raw material to make albumin.
- Inflammation redirects it. Albumin behaves as a negative acute phase reactant, meaning its level dips during significant inflammation while other proteins rise. This is why a sick, hospitalized patient often shows a low albumin that recovers as they heal.
When you can name which bucket applies, an isolated low albumin stops being frightening and becomes a question with a short list of answers your clinician can work through.
What raises globulin, and why it matters for your ratio
The other way the ratio drops is when globulin climbs. Globulin rises for reasons that are usually about the immune system working hard, whether appropriately or abnormally.
- Chronic infection or inflammation. Long-running immune stimulation prompts a broad, polyclonal rise in antibodies, lifting total globulin (Cleveland Clinic).
- Autoimmune disease. Conditions like lupus or rheumatoid arthritis keep the immune system chronically activated, which raises globulin and lowers the ratio (MedlinePlus).
- Monoclonal disorders. In multiple myeloma and related conditions, a single clone of plasma cells overproduces one abnormal antibody, driving total protein up while the A/G ratio falls (Cleveland Clinic).
The clinical fork is whether the rise is polyclonal, meaning many antibody types went up together in a reaction to inflammation, or monoclonal, meaning one abnormal clone took over. The first is common and often benign. The second warrants prompt investigation, which is exactly what SPEP is designed to separate.

Can you improve a low A/G ratio?
People often want to know if they can move the number, and the honest answer is that it depends entirely on the cause, because the ratio is a reflection of underlying processes rather than a target to chase directly.
- If low albumin comes from inadequate nutrition, improving protein intake and treating any malabsorption can help the liver rebuild albumin over time. Albumin has a half-life of roughly three weeks, so changes are gradual, not overnight.
- If it comes from inflammation, the ratio tends to normalize as the underlying inflammatory condition is treated and resolves.
- If it comes from organ disease, such as liver or kidney disease, the ratio improves only when that condition is managed, which is why the number is a monitoring tool rather than something to fix in isolation.
The key mindset shift is this: you do not treat a ratio, you treat the reason behind it. Trying to nudge the number without understanding its cause is chasing a shadow. The value of the A/G ratio is that it tells you where to point your attention.
Things that skew the ratio without any disease
Before assuming an out-of-range value means illness, it is worth knowing the everyday factors that can nudge the ratio in a perfectly healthy person. These are the benign explanations a good clinician considers first.
- Dehydration. When you are low on fluid, the blood is more concentrated, which can push total protein and albumin up and shift the ratio. A repeat test taken while well hydrated often looks different.
- Recent illness. A cold or minor infection in the days before your draw can transiently raise globulin as the immune system responds, temporarily lowering the ratio.
- Pregnancy. Normal physiological changes in pregnancy shift plasma volume and protein levels, so reference expectations differ.
- Prolonged tourniquet time or a difficult draw. Technical factors during collection can slightly alter measured protein, another reason a single borderline value is often rechecked.
This is why clinicians rarely act on one isolated reading. A ratio that is mildly off in a healthy, recently unwell, or dehydrated person is usually confirmed on a repeat draw before anyone reads more into it.
When a low or high ratio should prompt a doctor visit
Most A/G ratio results that sit just inside or barely outside the reference range in an otherwise well person do not require alarm. But some patterns deserve a conversation with your clinician rather than a wait-and-see approach.
- A low ratio paired with a high total protein, which can prompt further testing for a monoclonal process (Cleveland Clinic).
- A persistently low ratio across repeated panels, especially with symptoms like unexplained fatigue, swelling, or weight loss.
- An abnormal ratio alongside other red flags on the same panel, such as abnormal liver enzymes or kidney markers.
- Any ratio result your provider has specifically asked you to recheck.
Remember the framing from the start: the A/G ratio is a tripwire, not a verdict. Its whole purpose is to tell you and your clinician where to look next, and pairing it with the individual albumin, globulin, and total protein values is what turns a single number into a meaningful picture.
How the A/G ratio is followed over time
A single A/G ratio is a screening clue, not a diagnosis, and its real value often shows up when it is tracked across repeat panels. Because the ratio is derived from albumin and total protein, both of which move slowly, a one-time figure at the low or high edge of normal usually calls for a repeat rather than immediate alarm. Watching whether the ratio holds steady, drifts down, or recovers over weeks to months tells you far more than any single reading.
The direction of change is what clinicians care about. A ratio that stays stable within the reference range is reassuring even if it sits toward one end. A ratio that keeps falling on successive tests, driven either by dropping albumin or rising globulin, is a stronger signal that something is worth investigating than a one-time low value. If a cause has already been found and treated, for example inflammation that is settling or nutrition that is improving, a ratio trending back toward normal is a practical sign the situation is moving in the right direction. Because different labs can report slightly different albumin and total protein values, comparing your own results measured the same way over time is more reliable than comparing a single figure against a generic range. Trending turns a vague borderline number into something you can actually act on.
How age, sex, and pregnancy shift the A/G ratio
The A/G ratio does not read the same across every group, and a value that looks slightly off may simply reflect a normal life stage. Both albumin and globulin levels change with age, and the reference range used by a lab is usually built for adults, so results in children and older adults can differ from that template. Reading a ratio without that context risks calling normal variation a problem.
Pregnancy is a clear example of a physiological, non-disease shift. Blood volume expands during pregnancy, which dilutes albumin and can lower the A/G ratio without any underlying illness, so a mildly low ratio in a pregnant person is often expected rather than concerning. Sex differences are generally small, but combined with age they contribute to why a fixed cutoff does not fit everyone equally. Chronic conditions that become more common with age, such as ongoing low-grade inflammation, can also push the ratio down over years, which is one more reason the number is best interpreted against the person’s age, sex, and circumstances rather than in isolation. When a low or high ratio lines up with a recognized life stage, it usually deserves monitoring and context before it deserves worry.
Curious where your a/g ratio really sits?
Baseline a/g ratio and 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
What is the a/g ratio in a blood test?
It is the ratio of albumin to globulin, the two main proteins in your blood, calculated from a total protein test by dividing albumin by globulin (MedlinePlus). A normal ratio is slightly more than 1, reflecting a bit more albumin than globulin (Cleveland Clinic).
What is a normal a/g ratio?
A normal A/G ratio is slightly above 1, typically landing in the range of about 1.1 to 2.2 based on usual albumin and globulin values, though the exact cutoff varies by lab (Cleveland Clinic). Always compare your result to the reference range printed on your own report.
What does a low a/g ratio mean?
A low ratio most often reflects low albumin, high globulin, or both, and can point to liver disease, kidney disease, autoimmune conditions such as lupus, or certain cancers like multiple myeloma (MedlinePlus). It is a clue that guides further testing, not a diagnosis on its own.
What does a high a/g ratio mean?
A high A/G ratio usually reflects low globulin and is less common than a low ratio. It can be associated with some genetic disorders or with leukemia, so your clinician will look at why globulin is low (Cleveland Clinic).
Do I need to fast for an a/g ratio blood test?
The A/G ratio comes from a total protein test that is usually part of a comprehensive metabolic panel, and your provider may ask you to fast for the broader panel (MedlinePlus). Follow the specific instructions your lab or doctor gives you, since other tests drawn at the same time may have their own requirements.
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


