
No single test shows all cancers, but see the tumor markers and full panel that can catch early signs. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
- No single blood test shows all cancers, but tumor marker tests measure cancer-related proteins like PSA for prostate cancer, CA-125 for ovarian cancer, CEA for colon cancer, and AFP for liver cancer (Cleveland Clinic).
- A complete blood count (CBC) can flag blood cancers such as leukemia and lymphoma, but it cannot detect solid tumors like lung, breast, or colon cancer (Cleveland Clinic).
- An elevated tumor marker raises suspicion but does not confirm cancer on its own, because noncancerous conditions, medications, and even stress can also raise these levels (MedlinePlus).
If you have been told to get blood work to “check for cancer,” it helps to know what these tests can and cannot reveal. Most routine blood panels were never designed to diagnose cancer. A handful of specific tests, however, can point a clinician toward a cancer diagnosis or help monitor a known cancer. Below is a plain-language guide to which blood tests are actually used, what numbers matter, and where they fall short.
What blood test shows cancer?
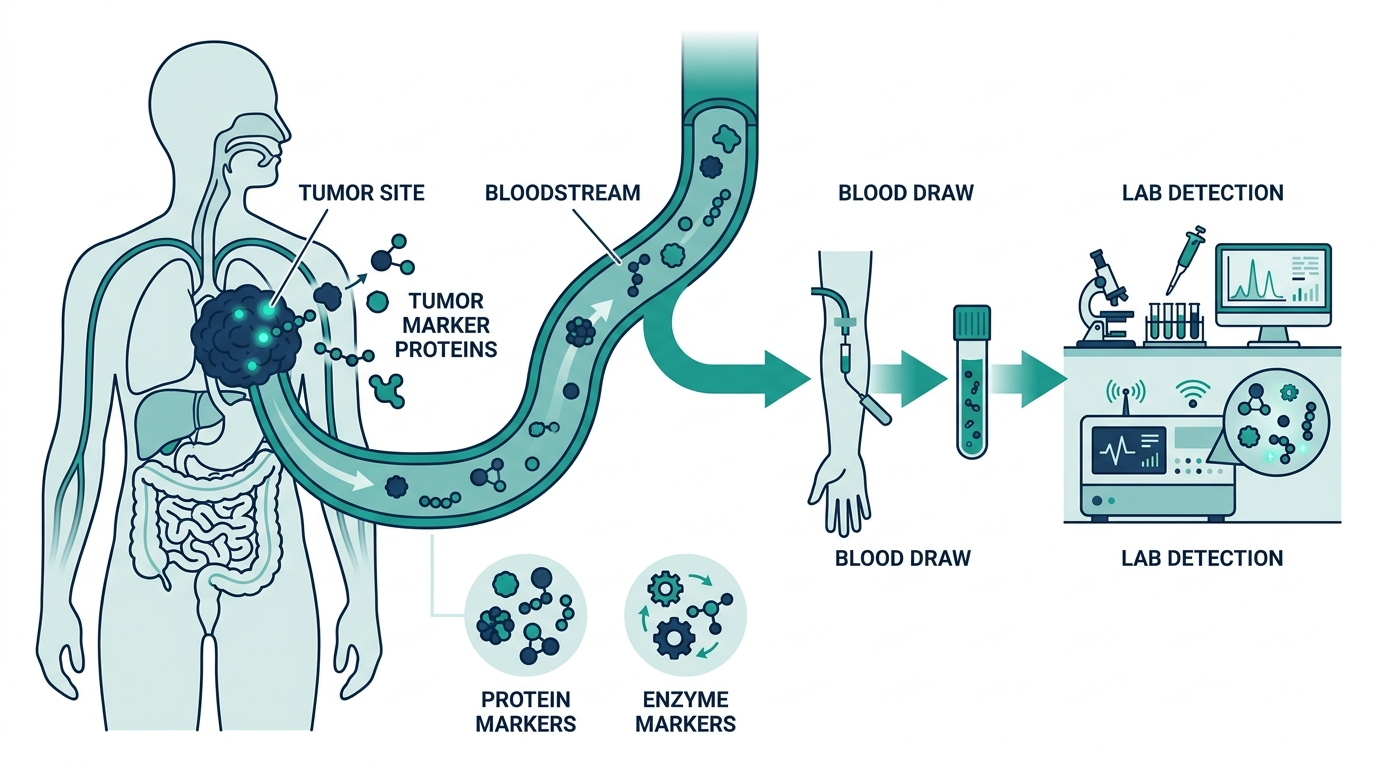
There is no single blood test that shows every cancer. The tests most directly tied to cancer are tumor marker tests, which measure substances that cancer cells (or the body in response to a tumor) release into the blood (Cleveland Clinic). Common examples include PSA, CEA, CA-125, AFP, CA 19-9, beta-hCG, and LDH. A complete blood count (CBC) can also reveal blood cancers like leukemia.
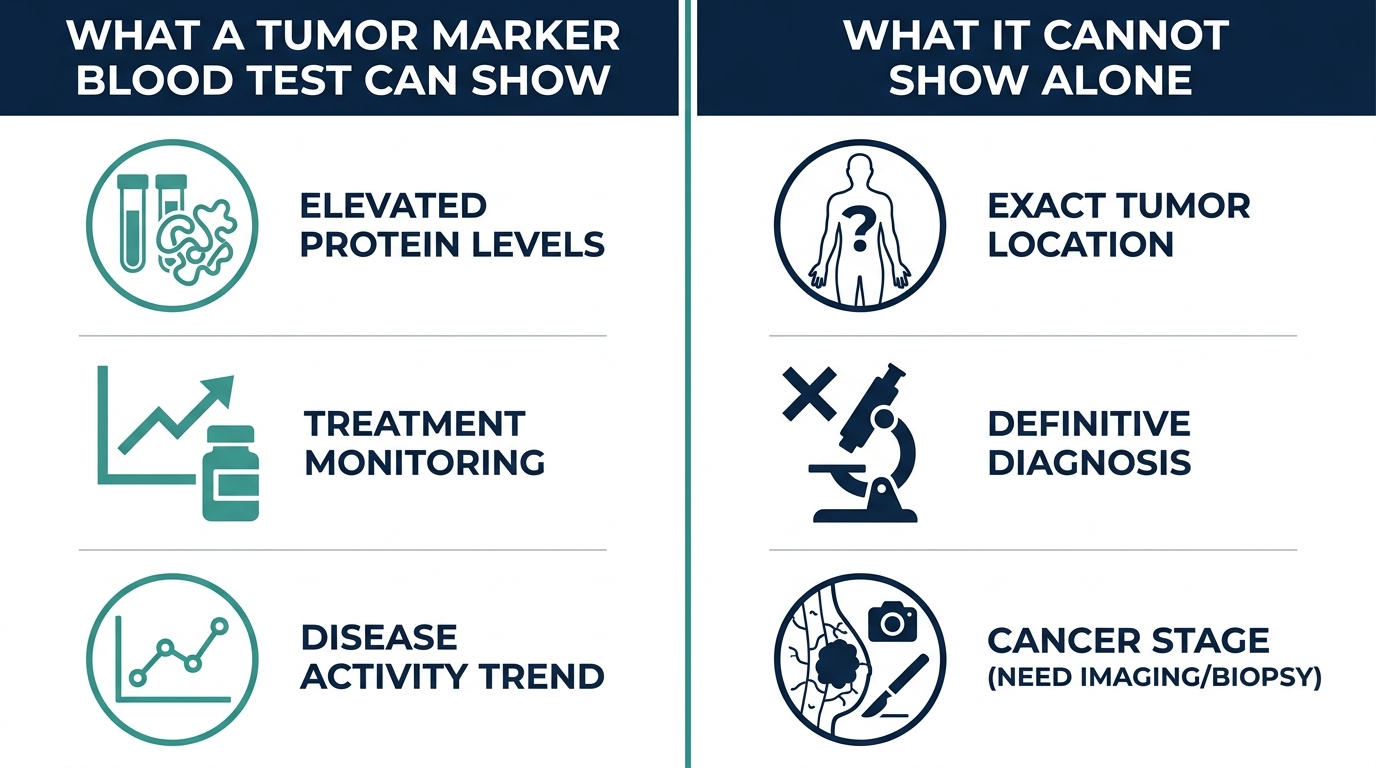
Importantly, these tests usually support a diagnosis rather than make it alone. Tissue biopsy and imaging remain the standard for confirming most cancers. Blood tests narrow the search and track how a known cancer responds to treatment.

What are tumor markers and which cancers do they signal?
Tumor markers are proteins or other substances often made in larger amounts by cancer cells, and each is linked to certain cancers (Cleveland Clinic). They are useful for diagnosis support, treatment planning, and watching for recurrence, but a high result is not proof of cancer.
- PSA (prostate-specific antigen): prostate cancer. A level above 4.0 ng/mL is generally considered abnormal and may prompt a biopsy, though cutoffs vary by age (MedlinePlus).
- CA-125: ovarian cancer, used to plan treatment and check for recurrence (MedlinePlus).
- CEA (carcinoembryonic antigen): colon and pancreatic cancer (Cleveland Clinic).
- AFP (alpha-fetoprotein): liver, testicular, and germ cell tumors. Normal values in adults are typically below about 10 ng/mL (MedlinePlus).
- CA 19-9: pancreatic, gallbladder, bile duct, and stomach cancer (Cleveland Clinic).
- beta-hCG: testicular and ovarian (germ cell) cancers (Cleveland Clinic).
- LDH (lactate dehydrogenase): leukemia, lymphoma, melanoma, and germ cell tumors (Cleveland Clinic).
Can a complete blood count (CBC) detect cancer?
A CBC can detect some blood and immune system cancers, such as leukemia and lymphoma, but it cannot detect solid organ cancers like lung, breast, or colon cancer (Cleveland Clinic). It measures red cells, white cells, and platelets, and abnormal counts can be an early clue.
In leukemia, for example, the body often produces large numbers of abnormal white blood cells, so a very high white cell count can be a hallmark on a CBC. As leukemia progresses, it crowds out healthy cells in the bone marrow, which can lower red cells and platelets too. The catch is that a CBC is not cancer-specific. Infections, anemia, and many benign conditions cause the same patterns, so an abnormal CBC means “investigate further,” not “you have cancer.”
What does an abnormal tumor marker result actually mean?
An abnormal tumor marker means your level is higher than expected, which warrants further testing, not a diagnosis. As MedlinePlus notes, false positives are common with markers like CA-125 and PSA, which can rise for reasons unrelated to cancer.
Several everyday factors can elevate these markers without any tumor present. Noncancerous conditions (such as benign prostate enlargement for PSA, or endometriosis and menstruation for CA-125), recent medical procedures, certain medications, smoking, and even physical stress can all push numbers up (Cleveland Clinic). Just as importantly, some people with cancer have normal marker levels, which is why a normal result does not rule cancer out. Clinicians read these numbers alongside symptoms, imaging, and often a biopsy. Trends over time, a rising marker across repeated tests, frequently matter more than one single reading.

Is there a single blood test that screens for many cancers?
Multi-cancer early detection (MCED) blood tests are an emerging option that can flag a signal from as many as 50 cancers in one draw, but they are not yet FDA approved as of mid-2026. The most advanced, GRAIL’s Galleri test, analyzes DNA fragments shed by tumors into the blood and is designed to be added alongside standard screening, not to replace it.
GRAIL submitted the final module of its FDA premarket approval application on January 29, 2026, and the review remains pending. The supporting PATHFINDER 2 study enrolled more than 25,500 asymptomatic adults over age 50, and the large NHS-Galleri trial enrolled over 140,000 adults aged 50 to 77 to see whether the test reduces late-stage cancer diagnoses. Until results and approval are final, MCED tests should be discussed with a clinician and treated as a complement to proven screening like mammograms and colonoscopies.
What blood tests are NOT a substitute for?
Blood tests do not replace established cancer screening or biopsy. For most solid tumors, a tissue biopsy confirms the diagnosis, and imaging shows location and spread (Cleveland Clinic).
Standard screening tests catch cancers that blood tests often miss. Mammograms screen for breast cancer, colonoscopy and stool tests for colorectal cancer, Pap and HPV tests for cervical cancer, and low-dose CT scans for lung cancer in high-risk people. These have decades of evidence behind them. One known limit of any screening, including blood-based tests, is that very aggressive cancers can grow fast enough to cause symptoms between tests. If you have persistent symptoms such as unexplained weight loss, lumps, unusual bleeding, or lasting fatigue, see a clinician regardless of what a blood test shows.
Tumor marker quick reference: what each test is used for
Because tumor markers are the blood tests most people mean when they ask about cancer, it helps to see them side by side with what they point to and how they are actually used. Note that these are used mostly to support diagnosis and monitor known cancer, not to screen healthy people.
| Marker | Most associated cancers | Main clinical use |
|---|---|---|
| PSA | Prostate | Screening discussion, diagnosis support, monitoring after treatment |
| CA-125 | Ovarian | Treatment planning and watching for recurrence, not general screening |
| CEA | Colorectal, some others | Monitoring response and recurrence in known colorectal cancer |
| AFP | Liver, testicular, germ cell | Diagnosis support and monitoring, often with imaging |
| CA 19-9 | Pancreatic, biliary | Tracking treatment response in known disease |
| beta-hCG | Testicular, germ cell | Diagnosis support and monitoring in germ cell tumors |
| LDH | Lymphoma, melanoma, germ cell | A general marker of disease burden, not cancer-specific |

How tumor markers are used across the cancer journey
A single number in isolation is the least useful way to read a tumor marker. Their real value comes at specific points in a patient’s course, and understanding those stages explains why your clinician may order the same test repeatedly.
- Supporting a diagnosis. When symptoms or imaging already raise suspicion, a marker can add weight to the picture. It rarely stands alone, and a biopsy usually confirms.
- Establishing a baseline. Once cancer is diagnosed, an initial marker level sets a reference point that later readings are compared against.
- Tracking treatment response. A marker that falls during chemotherapy or after surgery suggests the treatment is working. A marker that stops falling or rises can signal the opposite.
- Watching for recurrence. After treatment, a marker that had normalized and then begins climbing across repeated tests can be an early sign of return, often before symptoms.
This is why clinicians emphasize the trend over any one value. A rising line across three tests carries more meaning than a single number just above a cutoff.
Why false positives and false negatives both happen
Tumor markers are imperfect in both directions, and knowing why prevents needless panic or false reassurance.
Why a marker can be high without cancer:
- PSA rises with benign prostate enlargement, prostate inflammation, recent ejaculation, or even a recent digital rectal exam.
- CA-125 climbs with menstruation, endometriosis, pelvic inflammation, pregnancy, and other benign conditions, which is why it is a poor general screening test.
- CEA can rise in smokers and in benign liver or bowel conditions.
- CA 19-9 increases with bile duct blockage and other noncancerous problems.
Why a marker can be normal with cancer: Not every tumor produces its associated marker, and early or small cancers may not shed enough to move the number. Some people simply do not express a given marker even with advanced disease. This is exactly why a normal marker does not rule cancer out, especially when symptoms are present.
Blood cancers and what the CBC and smear reveal
The complete blood count is the blood test most likely to catch a cancer by accident, because blood and bone marrow cancers directly change the cells it counts. A few patterns clinicians look for:
- Very high or very abnormal white cell count. Leukemia often floods the blood with abnormal white cells, which can show as a strikingly high count.
- Low red cells and platelets together. As abnormal cells crowd the bone marrow, they squeeze out normal production, causing anemia and low platelets alongside the white cell changes.
- Abnormal cells on a smear. When counts look off, a peripheral blood smear lets a specialist look at the cells directly under a microscope, and immature or abnormal forms can point toward a blood cancer.
Even so, the CBC is not cancer-specific. Infection, iron deficiency, and many benign conditions produce overlapping patterns. An abnormal CBC means look closer, often with a smear, flow cytometry, or a bone marrow evaluation, not that cancer is confirmed.

Liquid biopsy and circulating tumor DNA
Beyond classic protein markers, a newer category of blood test looks for genetic material that tumors shed into the bloodstream, sometimes called a liquid biopsy. In people already diagnosed with cancer, these tests can detect circulating tumor DNA to help identify mutations that guide targeted therapy or to monitor for residual disease after treatment.
Multi-cancer early detection tests apply a similar idea to screening. They scan for DNA fragments and chemical patterns that many tumor types share, aiming to flag a cancer signal from a single blood draw. As covered above, the most advanced of these remains in FDA review as of mid-2026 and is designed to add to, not replace, proven screening. The honest framing is that liquid biopsy is powerful for managing known cancer and promising for early detection, but it is still maturing as a screening tool.
Symptoms that warrant evaluation regardless of blood results
Because blood tests can miss cancer, certain persistent symptoms deserve a clinician’s attention on their own, whatever a lab number shows:
- Unexplained weight loss without trying.
- A new lump or swelling anywhere.
- Unusual bleeding, such as blood in stool or urine, or bleeding between periods.
- A sore, cough, or change in bowel or bladder habits that does not resolve.
- Persistent, unexplained fatigue or night sweats.
- Difficulty swallowing or persistent indigestion that is new for you.
A normal tumor marker or CBC should never override symptoms like these. The right response is evaluation, which may include imaging or biopsy, rather than relying on a reassuring blood number to explain them away.
Where blood tests fit alongside imaging and biopsy
It helps to see blood tests as one instrument in a larger diagnostic toolkit rather than the star of the show. Each tool answers a different question, and cancer diagnosis usually combines several.
- Blood tests raise or lower suspicion, establish baselines, and track known disease over time. They are convenient and repeatable but rarely definitive on their own.
- Imaging, such as ultrasound, CT, MRI, or mammography, shows where an abnormality is, how large it is, and whether it has spread. It answers the “where and how much” question a blood test cannot.
- Biopsy, taking a tissue sample to examine under a microscope, remains the standard for confirming most solid cancers. It answers the “is this actually cancer, and what type” question definitively.
A typical path might be a suspicious symptom or an abnormal marker, then imaging to locate a concern, then a biopsy to confirm. The blood test is often the first thread, not the final verdict.
The PSA screening debate, in plain terms
PSA is the tumor marker most often used in something close to screening, and it illustrates why even a useful test is not a simple yes or no. A PSA above about 4.0 ng/mL is generally treated as abnormal, but the cutoff is not absolute. Some clinicians adjust it by age, and a raised PSA frequently reflects benign prostate enlargement rather than cancer.
The nuance that trips people up is the balance of benefits and harms. PSA screening can catch prostate cancer early, but it can also flag slow-growing cancers that would never have caused harm, leading to biopsies and treatments with their own risks. This is why major guidelines frame PSA screening as a shared decision between a man and his clinician, weighing age, family history, and personal preference, rather than a test everyone should automatically get. A single PSA number is a starting point for that conversation, not a diagnosis, and a rising trend across repeated tests usually carries more weight than one isolated reading just above the cutoff.
Common misunderstandings about blood tests and cancer
- “A blood test can screen me for all cancers today.” No single approved test does this. Multi-cancer detection tests are emerging but remain under review and are meant to complement standard screening.
- “A high tumor marker means I have cancer.” It means further testing is warranted. Benign conditions, medications, and everyday factors can raise these markers.
- “A normal blood test rules out cancer.” It does not. Some cancers do not raise markers, and a CBC can look normal in many cancers. Symptoms still matter.
- “Tumor markers are for screening healthy people.” Most are used to support diagnosis and monitor known cancer, not to screen the general population, precisely because false positives are common.
How to prepare for a tumor marker test and what to ask
Because tumor markers are so easily nudged by everyday factors, a little preparation and a few pointed questions can keep you from misreading the result. The goal is a clean number and a clear understanding of what it does and does not mean for you.
- Mention recent procedures and activities: a recent prostate exam or ejaculation can raise PSA, and menstruation or a pelvic condition can lift CA-125. Timing the draw away from these gives a truer reading.
- List every medication and supplement: some products can influence results, so a complete list helps your clinician interpret the number correctly.
- Ask why the test is being ordered: is it to support a diagnosis, set a baseline, track treatment, or watch for recurrence? The purpose shapes how the result should be read.
- Ask what an abnormal result would trigger: knowing in advance whether a high value leads to a repeat test, imaging, or a biopsy takes the fear out of an unexpected flag.
Framing the test as one step in a plan, rather than a verdict, is the single most useful mindset. It turns an anxious wait for a number into an informed conversation about next steps.
How often are tumor markers repeated?
Tumor markers earn most of their value through repetition, not a single reading, so the schedule of retesting is part of how they work. The frequency depends entirely on why the test is being used.
- During active treatment: a marker may be checked at regular intervals to see whether it is falling, which suggests the therapy is working.
- After treatment: a marker that normalized is often rechecked periodically during follow-up, since a rising trend can be an early clue of recurrence before symptoms appear.
- When investigating a symptom: a single abnormal value is commonly repeated to confirm it is real and not a one-off fluctuation before further testing is arranged.
Across all of these, the pattern matters more than any one point. A marker drifting steadily upward across several draws tells a very different story than a lone value sitting just above a cutoff, which is exactly why clinicians plot the trend rather than react to a single number.
Turn what you just learned into action.
Superpower lets you test 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
Can a routine blood test detect cancer?
A routine panel like a CBC or metabolic panel is not designed to detect cancer. A CBC can occasionally flag blood cancers such as leukemia through abnormal cell counts, but it cannot find solid tumors. Specific tumor marker tests are ordered separately when cancer is suspected (Cleveland Clinic).
What is the most common blood test for cancer?
Tumor marker tests are the most common cancer-specific blood tests. Examples include PSA for prostate cancer, CA-125 for ovarian cancer, CEA for colon cancer, and AFP for liver cancer. They are used to support diagnosis, plan treatment, and check for recurrence (MedlinePlus).
Does a normal blood test mean I do not have cancer?
No. Some cancers do not raise tumor markers, and a CBC can look normal in many cancers. A normal result is reassuring but does not rule cancer out, especially if you have symptoms. Imaging and biopsy may still be needed (MedlinePlus).
How accurate are tumor marker tests?
They are useful but imperfect. False positives are common with markers like CA-125 and PSA, since benign conditions can raise them. False negatives also occur. Clinicians interpret markers alongside imaging, symptoms, and biopsy rather than relying on one number (MedlinePlus).
What PSA level is concerning for cancer?
A PSA above 4.0 ng/mL is generally considered abnormal and may prompt a prostate biopsy, though some doctors use age-based cutoffs, lower for younger men and higher for older men. A high PSA can also come from benign prostate enlargement, not cancer (MedlinePlus).
Sources
- Cleveland Clinic, Tumor Markers Tests
- Cleveland Clinic, Blood Tests for Cancer: Diagnosis and Screening
- MedlinePlus, Tumor Marker Tests
- MedlinePlus, CA-125 Blood Test (Ovarian Cancer)
- MedlinePlus, Prostate-Specific Antigen (PSA) Blood Test
- MedlinePlus, Alpha-Fetoprotein (AFP) Tumor Marker Test
- GRAIL, FDA Premarket Approval Application for the Galleri Test
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Related: best at-home biomarker tests of 2026.
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


