
You went to your doctor with months of joint aches, a stubborn rash, and a fatigue that sleep does not touch. Someone said the word lupus, ordered blood work, and now you are staring at an alphabet soup of acronyms wondering which line on the page actually answers the question. Here is the honest truth that gets buried in most explainers: there is no single blood test that says lupus on it. Lupus is diagnosed by a panel of tests read together, and knowing what each one is doing changes how you read your own results.
Chasing an answer on lupus markers? A full panel can show what else is happening alongside your antibody results. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
The good news is that the panel is logical once someone explains it. Let me walk you through it the way a rheumatologist actually thinks about it.
What blood test shows lupus?
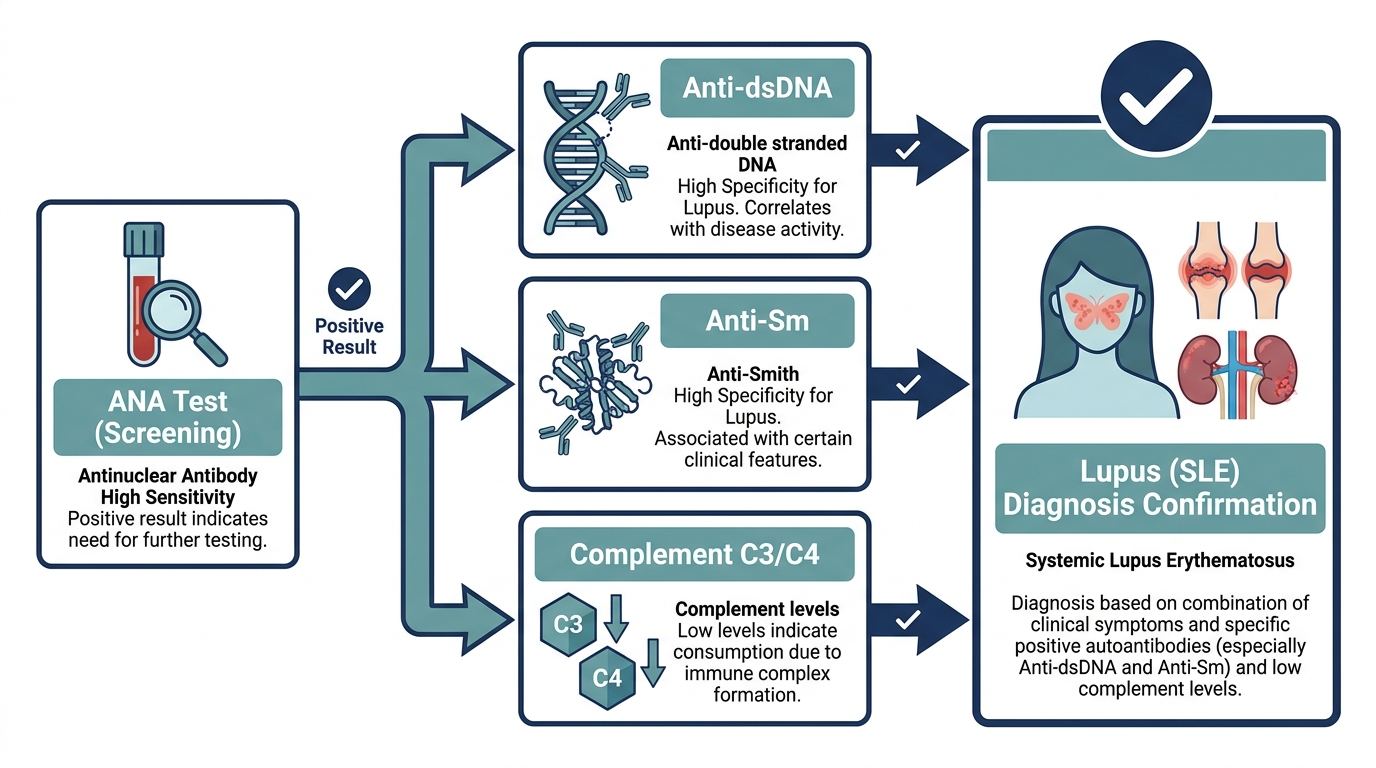
The blood test that shows lupus is not one test but a sequence. The screening test is the ANA (antinuclear antibody) test, and almost everyone with lupus tests positive on it. If the ANA is positive, doctors then run more specific antibody tests, the most telling being anti-dsDNA and anti-Smith, which are highly specific for lupus (PMC). Alongside those, complement tests (C3 and C4) and a complete blood count help confirm the picture and gauge how active the disease is.
So when people ask what blood test for lupus they should request, the real answer is a workflow: ANA first as a wide net, then anti-dsDNA and anti-Smith to narrow it down, then complement and a CBC to round out the diagnosis. No single number diagnoses lupus on its own (MedlinePlus).

What is the ANA test, and why is it the starting point?
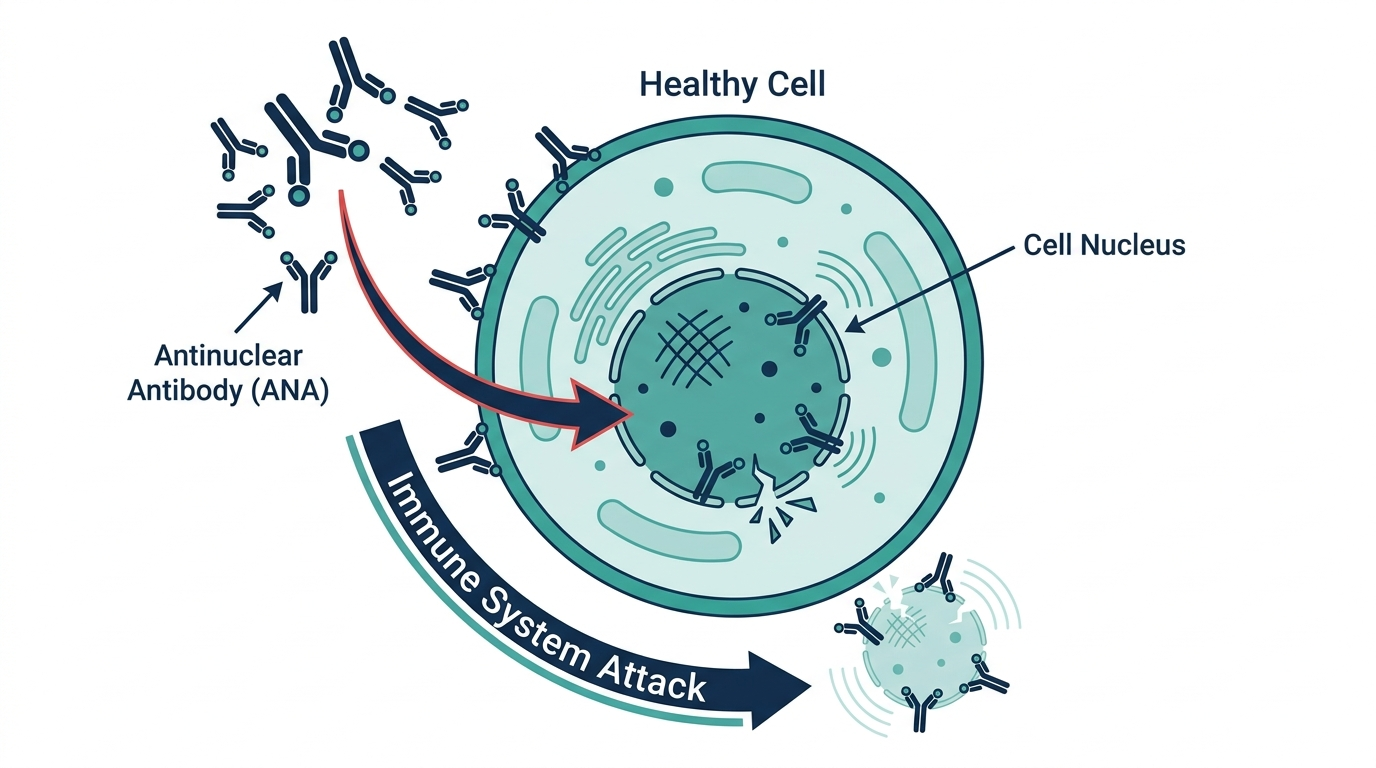
The ANA test is the front door to a lupus workup. It checks your blood for antinuclear antibodies, which are antibodies that mistakenly target the nucleus of your own cells, a hallmark of autoimmune disease (MedlinePlus). It is used to help diagnose systemic lupus erythematosus (SLE), the most common type of lupus.
The reason ANA is the screening test is its sensitivity. The vast majority of people with lupus have a positive ANA, so a negative result makes lupus much less likely. But the test is a wide net, not a precise hook. Up to 3 in 10 healthy people without any autoimmune disease will also have a positive ANA, and a positive result can show up with ordinary viral infections or certain medications (Cleveland Clinic). That is why a positive ANA alone never means you have lupus. It means the investigation continues.
So when someone asks what blood test is for lupus, the ANA is the one almost everyone gets first, but it is the beginning of the conversation rather than the verdict.
What do the lupus-specific antibody tests show?
The lupus-specific antibody tests are what turn a vague positive ANA into a real answer. After a positive ANA, doctors look for two antibodies in particular: anti-dsDNA (anti double-stranded DNA) and anti-Smith (anti-Sm). Both are highly specific for lupus, meaning they rarely appear in people who do not have it (Johns Hopkins Medicine).
Here is how they differ in practical terms:
- Anti-dsDNA. Found in a large share of people with lupus and considered highly specific for the diagnosis. Anti-dsDNA antibodies occur primarily, and possibly exclusively, in SLE (PMC). Levels can also rise and fall with disease activity, which makes this test useful for tracking, not just diagnosing.
- Anti-Smith (anti-Sm). Even more specific to lupus than anti-dsDNA, though it shows up in fewer patients. If you test positive for anti-Sm, it is a strong pointer toward lupus (Johns Hopkins Medicine).
- Other autoantibodies. A fuller lupus panel may include anti-RNP, anti-Ro (SSA), anti-La (SSB), and antiphospholipid antibodies, which help map the specific flavor of autoimmune disease and your risks (Johns Hopkins Medicine).
The trade-off built into these tests is worth understanding. ANA is sensitive but not specific. Anti-dsDNA and anti-Sm are specific but not sensitive, meaning plenty of people with lupus test negative on them. That is exactly why doctors run them as a set. One catches almost everyone, the others confirm the diagnosis in those who have them.
What does the complement test (C3 and C4) show?
The complement test measures proteins called C3 and C4 that are part of your immune system, and low levels can be a sign of lupus (MedlinePlus). In lupus, the immune system burns through complement proteins as it attacks the body, so the levels in your blood drop. A lower-than-normal C3 or C4 can therefore signal active autoimmune disease (Cleveland Clinic).
What makes complement genuinely useful is that it moves with the disease. As treatment works and inflammation settles, complement levels tend to rise back toward normal. If you are being treated for lupus, rising complement can mean your treatment is working (MedlinePlus). That is why rheumatologists often recheck C3 and C4 over time rather than just once. These are not only diagnostic tests, they are a dashboard for how loud the disease is right now.

What other blood and urine tests are part of a lupus workup?
Beyond antibodies and complement, a lupus workup includes general tests that reveal how the disease is affecting your body. Lupus is a whole-body condition, so doctors check the organs it tends to hit. Mayo Clinic notes that a complete blood count, an erythrocyte sedimentation rate (ESR), kidney and liver assessments, and a urinalysis are standard parts of the evaluation (Mayo Clinic).
Here is what each one is looking for:
- Complete blood count (CBC). Lupus often lowers red blood cells, white blood cells, or platelets, so a CBC can reveal anemia or low cell counts that fit the picture (Mayo Clinic).
- ESR. This inflammation marker is often elevated when lupus is active, although it is not specific to lupus on its own (Mayo Clinic).
- Kidney and liver tests. A chemistry panel checks how well these organs are working, because lupus can quietly damage the kidneys (Johns Hopkins Medicine).
- Urinalysis. A urine sample can show protein or blood, an early flag for lupus affecting the kidneys, which is one of the most serious complications to catch early (Mayo Clinic).
None of these tests are lupus-specific by themselves. Their job is to assemble a body of evidence. A rheumatologist weighs them together with your symptoms and the antibody results to reach a diagnosis, because lupus is fundamentally a clinical diagnosis supported by labs, not a single lab value.
The insider truth: a negative ANA does not always rule out lupus
This is the part that surprises even many patients who have done their homework. For decades the teaching was that lupus without a positive ANA was so rare it barely existed. That is no longer holding up. Research has found that as many as 30 percent of patients with SLE who are screened for clinical trials test ANA negative, which puts the real-world sensitivity of the test closer to 70 percent than the near-100 percent figure often quoted (PMC).
Why the gap? A big driver is the test method. The most reliable ANA test is done by indirect immunofluorescence, which a human reads under a microscope. Many labs have switched to faster automated assays that can miss certain patterns, and assay variability between platforms is significant (PMC). Two labs can test the same blood and disagree.
The practical lesson is this. If your symptoms strongly suggest lupus but your ANA came back negative, that is not always the end of the story. It can be worth asking which method the lab used, and whether a rheumatologist thinks the clinical picture warrants looking further regardless of that one result. This is exactly the kind of nuance that disappears when a report just prints negative and everyone moves on.
Why lupus is never diagnosed on blood alone
The most important thing to understand about lupus testing is that no antibody, and no combination of antibodies, is enough by itself. Lupus is a clinical diagnosis in which the labs are supporting evidence. The current classification framework used by researchers, the 2019 EULAR/ACR criteria, makes this explicit. It treats a positive ANA (at a titer of at least 1:80) as an obligatory entry requirement, then adds up weighted points across clinical and immunological categories, and classifies someone only when they reach a threshold of 10 points. The categories span constitutional symptoms, blood cell abnormalities, skin and mouth findings, joint involvement, kidney involvement, and the immunological markers like low complement and lupus-specific antibodies.
The practical message for a patient reading their own results is reassuring: a single positive line does not make lupus, and a single negative line does not unmake it. The diagnosis is a picture assembled from your symptoms over time plus a spread of tests, which is exactly why a rheumatologist, not a lab printout, makes the call.
The symptoms the panel is trying to explain
Blood tests for lupus are ordered to make sense of a pattern of symptoms, and knowing that pattern helps you understand why a doctor reached for the panel in the first place. Lupus is a systemic disease, so its features touch many organs.
- A butterfly-shaped rash across the cheeks and bridge of the nose, often worsened by sunlight, is one of the most recognizable signs.
- Joint pain and swelling, frequently in the hands, wrists, and knees, that can move around and come in flares.
- Profound fatigue that rest does not resolve, one of the most common and most disabling features.
- Photosensitivity, where sun exposure triggers rashes or a general worsening of symptoms.
- Mouth or nose ulcers, often painless, which patients may not even notice.
- Fingers that turn white or blue in the cold (Raynaud phenomenon), and unexplained fevers or hair loss.
When several of these appear together, especially in a woman of childbearing age (the group most affected), the panel becomes the tool for confirming or ruling out an autoimmune cause.
How the same tests track a flare, not just a diagnosis
One feature that sets lupus labs apart from most diagnostic tests is that a few of them keep working after the diagnosis is made. They become a dashboard for disease activity, which changes how often they are drawn.
- Anti-dsDNA levels tend to rise as the disease becomes more active and fall as it quiets, so a climbing anti-dsDNA can be an early warning of a flare, particularly one involving the kidneys.
- Complement (C3 and C4) moves in the opposite direction: it drops when the disease is consuming these proteins during a flare and recovers as treatment works. A falling complement alongside a rising anti-dsDNA is a classic active-disease signature.
- Urinalysis is rechecked because new protein or blood in the urine is one of the earliest signs that lupus is affecting the kidneys, a complication where early detection genuinely changes outcomes.
- CBC is followed because active lupus, and some of the medications used to treat it, can lower blood counts.
This is why a rheumatologist does not just test once and file the result. The same panel, repeated over time, tells the story of whether the disease is calm or stirring.
Drug-induced lupus: a different pattern worth knowing
Not all lupus-like blood results come from lupus itself. A distinct condition called drug-induced lupus can develop in some people taking certain long-term medications, and it has its own antibody fingerprint. The vast majority of people with drug-induced lupus have anti-histone antibodies, which is why that test is specifically checked when this cause is suspected. Classic triggers include the blood pressure medication hydralazine and the heart rhythm drug procainamide, along with others such as isoniazid, minocycline, and some biologic drugs. The important and hopeful distinction is that drug-induced lupus usually improves after the offending medication is stopped, often within weeks, whereas systemic lupus is a chronic condition. Anyone who develops lupus-like symptoms after starting a new long-term medication should raise this possibility with their clinician rather than assuming the worst, and should never stop a prescribed drug on their own.

Preparing for a lupus panel and what can affect results
Lupus blood tests do not usually require fasting, but a few practical points help you read your results accurately.
- Timing relative to symptoms matters. Because markers like anti-dsDNA and complement track disease activity, results drawn during a flare can look very different from results drawn during a calm period. This is a feature, not an error, and it is part of why serial testing is more informative than a single draw.
- Infections and other conditions can raise ANA. A positive ANA can appear transiently during a viral illness or with other autoimmune conditions, so timing and context are read alongside the number.
- Lab method affects the ANA result. The most reliable ANA method is indirect immunofluorescence read by a human, and automated platforms can disagree. If a result is surprising given the clinical picture, the testing method is a fair thing to ask about.
- Medications should be disclosed. Because certain drugs can trigger lupus-like antibodies, a complete medication and supplement history is part of interpreting the panel correctly.
Who should be tested, and what the results steer next
Lupus testing is not a screen for the general population. Ordering ANA and its follow-up antibodies makes sense when there is a real clinical suspicion, a cluster of the symptoms above, rather than as a routine wellness check, because a positive ANA in a symptom-free person is common and usually means nothing. When testing is appropriate, the results steer a clear set of next steps: a positive ANA with lupus-specific antibodies and supporting findings leads to a rheumatology diagnosis and a treatment plan; a positive ANA without specific antibodies or symptoms often leads to watchful follow-up rather than a label; and a strongly suggestive clinical picture with a negative ANA can still warrant specialist review, given the known limits of the test. In every path, the blood work narrows the possibilities, and a specialist integrates it with the rest of the story.
Common misunderstandings about lupus blood tests
- “A positive ANA means I have lupus.” No. A large share of healthy people have a positive ANA, and it also appears with infections and other conditions. It opens an investigation; it does not close one.
- “A negative ANA rules lupus out completely.” Usually it makes lupus much less likely, but a meaningful share of people with lupus can test ANA negative depending on the method, so a strong clinical picture may justify further evaluation.
- “One blood test can confirm lupus.” It cannot. Lupus is diagnosed from a pattern of symptoms plus several tests read together, not from any single value.
- “My antibody levels should never change.” For lupus they are expected to change. Anti-dsDNA and complement move with disease activity, which is precisely what makes them useful for monitoring.
- “Lupus-like symptoms always mean lifelong lupus.” Not always. Drug-induced lupus can mimic the disease and often resolves once the responsible medication is stopped.
How to read an ANA titer and pattern on your report
When an ANA comes back positive, the report rarely just says positive. It usually gives two extra pieces of information, the titer and the pattern, and knowing what they mean takes a lot of the mystery out of the page in front of you.
The titer describes how much the blood had to be diluted before the antibodies could no longer be detected. It is written as a ratio such as 1:80, 1:160, 1:320, and so on. Each step represents a further doubling of the dilution, so a higher second number means the antibodies were still detectable even in a more diluted sample, which generally suggests a stronger signal. A low-positive titer like 1:80 is common in the healthy population and often means little on its own, whereas higher titers are more likely to accompany a genuine autoimmune process. The titer is a clue to strength, not a severity score for any particular disease.
The pattern describes how the antibodies light up the cell nucleus under the microscope, with names like homogeneous, speckled, or nucleolar. Certain patterns are more often associated with particular antibodies and conditions, which is why a rheumatologist pays attention to them. The key thing for a patient to understand is that neither the titer nor the pattern diagnoses lupus by itself. They refine the picture and help the specialist decide which follow-up antibody tests are worth running, but the diagnosis still comes from the whole panel plus your symptoms.
Telling lupus apart from look-alike conditions
One reason the lupus panel casts such a wide net is that several other autoimmune conditions share overlapping symptoms and even some of the same antibodies. Part of the workup is not just confirming lupus but distinguishing it from these relatives, because the treatment and outlook differ.
- Sjogren’s syndrome often features prominent dry eyes and dry mouth and is frequently linked with anti-Ro (SSA) and anti-La (SSB) antibodies, which is why those are included in a fuller panel.
- Mixed connective tissue disease blends features of lupus, scleroderma, and myositis, and is strongly associated with high levels of anti-RNP antibodies, so that marker helps flag it.
- Rheumatoid arthritis can cause joint pain that overlaps with lupus, but it has its own markers such as rheumatoid factor and anti-CCP antibodies, which help separate the two.
- Drug-induced lupus, covered above, is set apart by anti-histone antibodies and its tendency to resolve after the triggering medication is stopped.
This is why a positive ANA leads to a spread of specific antibody tests rather than a single confirmatory one. The pattern of which antibodies are present and which are absent, read together with the clinical picture, is what lets a rheumatologist land on lupus rather than one of its look-alikes, or recognize that two conditions coexist.
Don’t just read about your health, track it.
A single result is a snapshot. Superpower re-tests 100+ markers over time so you can watch them move as you change sleep, food, and training.
Frequently asked questions
What blood test for lupus is done first?
The ANA (antinuclear antibody) test is almost always first. It is a sensitive screening test, so a negative result usually makes lupus much less likely, while a positive result leads to more specific follow-up tests (MedlinePlus).
Does a positive ANA mean I have lupus?
No. A positive ANA only means the test detected antinuclear antibodies. Up to 3 in 10 healthy people test positive, and so do people with infections or on certain medications, so a positive ANA is interpreted alongside your symptoms and other tests (Cleveland Clinic).
What blood test is most specific for lupus?
Anti-dsDNA and anti-Smith (anti-Sm) antibodies are the most specific. They appear primarily, and possibly only, in lupus, so a positive result strongly supports the diagnosis, though many people with lupus still test negative on them (PMC).
What do low complement (C3, C4) levels mean in lupus?
Low C3 and C4 can be a sign of active lupus, because the immune system uses up these proteins as it attacks the body. Levels rising back toward normal during treatment can suggest the therapy is working (MedlinePlus).
Can you have lupus with a negative ANA?
It is possible, though uncommon. Research suggests up to 30 percent of people with SLE in some studies test ANA negative, partly due to differences in lab testing methods. If symptoms point to lupus despite a negative ANA, further evaluation by a rheumatologist may be warranted (PMC).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


