
Educational content, not medical advice. Talk to a licensed clinician before starting any medication or peptide protocol.
Short answer: Yes, Ozempic is a peptide. Semaglutide, its active ingredient, is a 31-amino-acid engineered peptide that mimics the gut hormone GLP-1. But it is not the same category as the “peptide therapy” sold by wellness clinics and grey-market vendors. Ozempic is an FDA-approved prescription drug; most other weight-loss peptides are either investigational compounds or classified as “research use only.” The difference matters enormously for safety, legality, and what you actually get in the vial.
Ozempic is an FDA-approved peptide, but the weight-loss landscape is bigger than one drug. See where your own numbers stand. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
The word “peptides” has two different worlds colliding under one roof, and almost nobody explains the collision clearly. On one side: Ozempic, Wegovy, and the GLP-1 drug class, covered on the evening news, prescribed through licensed telehealth clinics, and backed by Phase 3 trials in tens of thousands of patients. On the other side: BPC-157, CJC-1295, retatrutide, sermorelin, and a dozen other compounds that circulate in longevity forums, recovery communities, and the grey-market vial economy.
Both sides use the word “peptide.” They are not the same thing. Here is a clear map of what each world contains, how Ozempic sits within it, and what to do with that information.
So, is Ozempic actually a peptide?
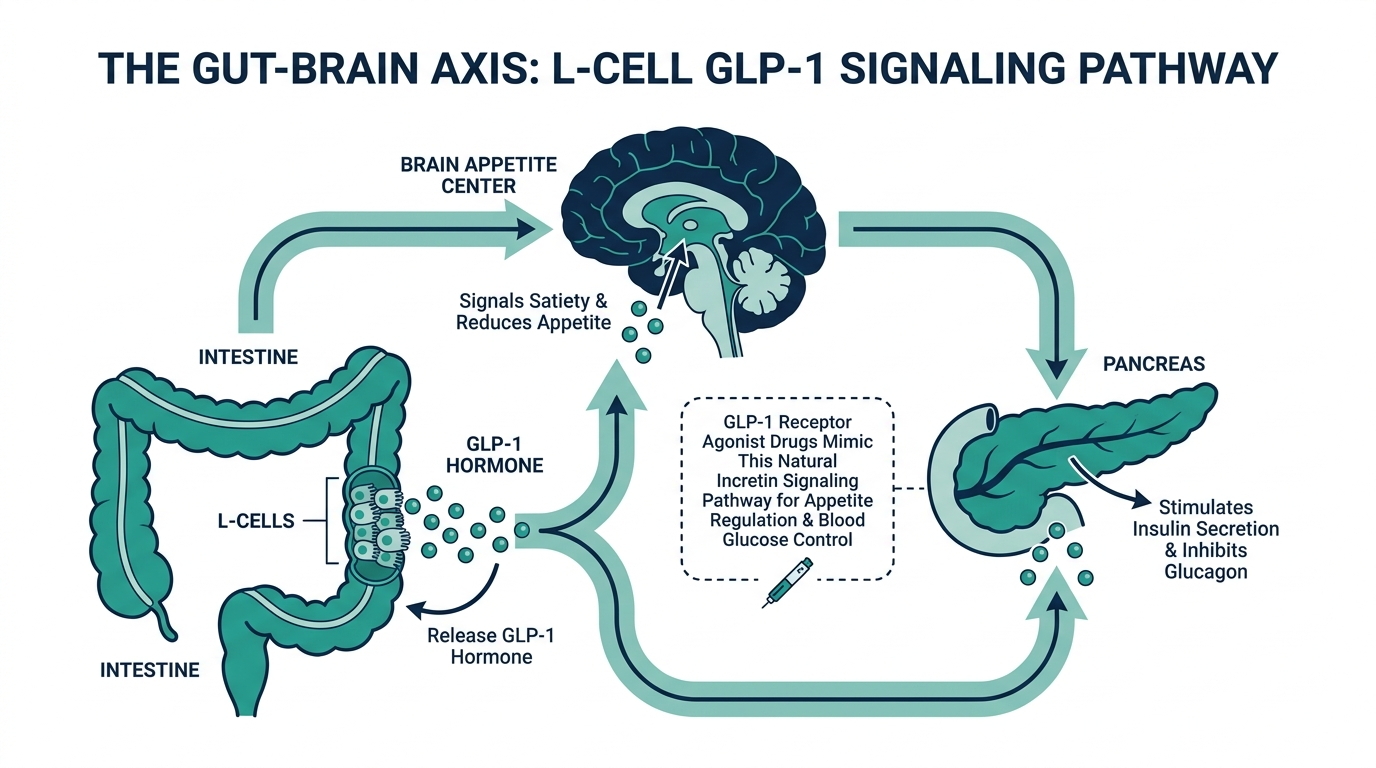
At the molecular level, yes. Semaglutide, the active drug in Ozempic and Wegovy, is a 31-amino-acid synthetic peptide, engineered from a blueprint provided by your own gut hormone GLP-1 (glucagon-like peptide-1). It shares 94% structural homology with native human GLP-1, meaning 29 of its 31 amino acid residues are identical to the hormone your intestines naturally release after a meal.
The three changes from natural GLP-1 are deliberate and surgical:
- Position 8: alanine is replaced with alpha-aminoisobutyric acid (Aib), which blocks the enzyme DPP-4 from degrading the molecule quickly. Natural GLP-1 is destroyed by DPP-4 within 1 to 2 minutes. Semaglutide survives it.
- Position 34: lysine is swapped for arginine, which limits where the fatty acid chain can attach.
- Position 26: a C-18 fatty diacid side chain is attached through a linker. This chain grabs onto albumin, a protein in your blood, which extends the drug’s circulating half-life to approximately 165 to 184 hours (roughly seven days).
Those three changes turn a 2-minute hormone into a once-weekly injection that suppresses appetite for the full week. That is not magic. It is deliberate chemical engineering, and it is why the “compounded semaglutide” market was legally precarious: any compound that is not that exact molecular structure is not semaglutide, regardless of what the label says.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
What is “peptide therapy” and how is it different from Ozempic?
The simplest way to actually get this done
Superpower is a full-body lab membership that runs 100+ biomarkers, has each result reviewed by a doctor, and tracks your numbers year over year (about $199/year). It is what we point readers to when they would rather get one clean, complete draw than chase single tests one at a time. Here is superpower reviewed in full.
When wellness clinics, longevity forums, and grey-market vendors say “peptides,” they typically mean a category of compounds that includes growth hormone secretagogues (CJC-1295, ipamorelin, sermorelin), tissue repair peptides (BPC-157, TB-500), and a loose collection of investigational or off-label molecules. These are often called “research peptides” or “therapeutic peptides.”
The key difference from Ozempic is regulatory status, not chemistry. Ozempic went through roughly 15 years of Phase 1, 2, and 3 clinical trials, including the STEP program, SUSTAIN trials, and SELECT cardiovascular outcomes trial, before FDA approval. Semaglutide’s SELECT trial alone enrolled 17,604 participants. The therapy-peptide world has a fraction of that evidence; BPC-157, for example, has no completed human Phase 2 or Phase 3 trials for any indication.
| Feature | Ozempic (semaglutide) | Research / therapy peptides (BPC-157, CJC-1295, etc.) |
|---|---|---|
| FDA approval | Yes (T2 diabetes 2017; weight 2021 as Wegovy) | No (investigational or research-use) |
| Human trial data | Phase 3, 10,000+ participants | Mostly animal models; no completed Phase 2/3 for weight |
| Dispensed through | Licensed physician + pharmacy | Compounding pharmacy (varies) or grey-market vendor |
| Legal to use on yourself | Yes, with prescription | Depends on compound and context |
| Insurance coverage | Sometimes (with obesity diagnosis) | No |
| Monthly cost | $149 to $599+ branded; compounded window largely closed | $40 to $250 per vial; telehealth peptide programs $199 to $399/mo |
Sermorelin is a partial exception: it is FDA-approved (as a diagnostic and as a treatment in pediatric GH deficiency), and it is now available through legitimate telehealth for off-label adult optimization at $175 to $225 per month.
Why do people mix Ozempic and “peptides” into the same conversation?
Partly chemistry, partly marketing. Since GLP-1 drugs are technically peptides, and since peptide clinics have been growing at the same time GLP-1 awareness exploded, the two concepts bleed together in search queries and forum threads. There is also an audience overlap: people investigating peptide therapy for longevity and recovery often stumble into the GLP-1 question, because weight loss is almost always part of the goal.
The marketing blur is real. Some wellness clinics now offer “GLP-1 peptide programs” that bundle semaglutide or tirzepatide prescriptions with other peptide protocols, presenting the whole stack under one “peptide therapy” umbrella. That framing is not wrong, exactly. But it papers over a crucial distinction: the GLP-1 part of the stack has a drug approval, a pharmacist, and a physician behind it. The other peptides in the bundle may or may not.
Personally, I find the bundling confusing at best and misleading at worst, especially when the “peptide program” price obscures what percentage of the cost is the regulated drug and what percentage is the grey-area add-ons.
What peptides, besides Ozempic, actually help with weight loss?
This is where the evidence gets stratified quickly. Here is an honest accounting:
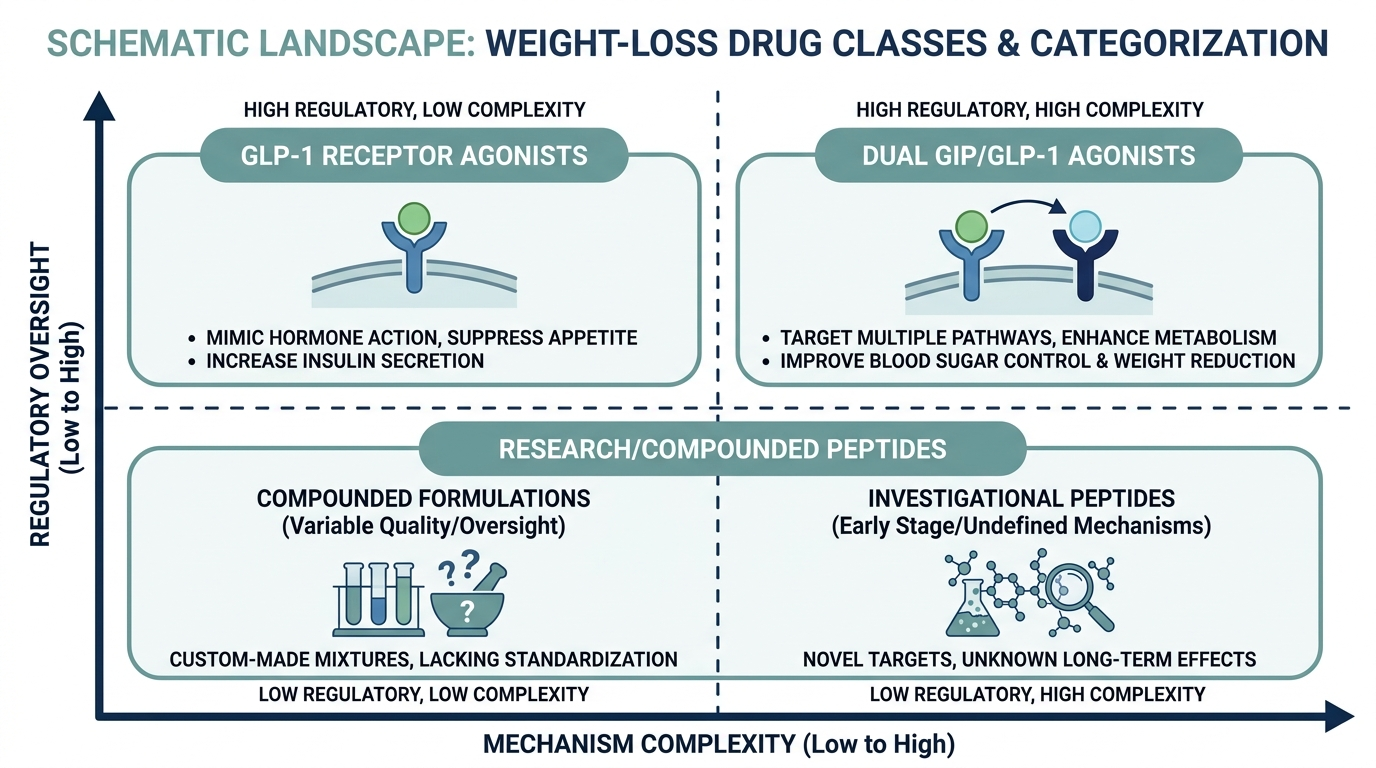
FDA-approved GLP-1 class (prescription only):
- Semaglutide (Ozempic for T2D, Wegovy for weight): The STEP 2 trial found 14.9% mean body weight reduction at 68 weeks. The STEP UP trial published in 2025 showed the higher 7.2 mg dose delivering 20.7% weight loss at 72 weeks. This is the benchmark.
- Tirzepatide (Mounjaro, Zepbound): A dual GIP/GLP-1 agonist. The SURMOUNT-1 trial showed 22.5% mean body weight reduction at 72 weeks on the 15 mg dose, currently the highest Phase 3 result for any approved weight drug.
- Orforglipron (Foundayo): FDA-approved May 2026. An oral, small-molecule GLP-1 receptor agonist from Eli Lilly. Not technically a peptide because it does not have an amino acid chain. Phase 3 data showed 9 to 10% weight loss, less than injectable semaglutide but significant for a daily pill with no injection.
Pipeline GLP-1 class (not yet approved):
- Retatrutide: A GIP/GLP-1/glucagon triple agonist. Phase 2 data from Eli Lilly showed 24.2% mean weight reduction at 48 weeks on 12 mg weekly, the highest recorded pharmacological weight loss in human trials. Phase 3 trials are ongoing as of mid-2026; approval is not expected before late 2026 at earliest. It is frequently sold as a “research peptide” and was the exact compound that failed independent lab testing at Peptide Sciences before its March 2026 closure.
- CagriSema (cagrilintide + semaglutide): Novo Nordisk combination showing approximately 22.7% weight loss in Phase 2; NDA submitted December 2025.
Therapy peptides with indirect weight effects (research use / compounding):
- Sermorelin and CJC-1295/Ipamorelin: These are growth hormone secretagogues. They increase the pulse of natural GH release, which supports lean mass and can contribute to fat loss over months. Neither is directly suppressing appetite the way GLP-1 drugs do. Sermorelin is the only one in this category with an FDA approval (for pediatric use), and it is now prescribed off-label through telehealth.
- BPC-157: Primarily associated with tissue repair and gut health. No direct weight-loss mechanism backed by human trials. But it is the most-bought research peptide in the US, and the February 2026 HHS signal that it may return to Category 1 compounding status (with a Pharmacy Compounding Advisory Committee meeting on 23 to 24 July 2026) means the legal route is opening up through pharmacies rather than grey-market vendors.
The myth worth busting directly: No research peptide has clinical trial data remotely comparable to the GLP-1 drug class for weight loss. Anyone who tells you BPC-157 or CJC-1295 will produce 15 to 22% body weight loss is extrapolating from rodent studies or from the anecdote pile. The numbers are not there.
What happened to compounded semaglutide in 2026?
This is the question underneath most GLP-1 searches in 2026, because millions of patients were using it. The short version:
The FDA removed semaglutide from the drug shortage list on 21 February 2025, which ended the legal basis for 503A and 503B compounding pharmacies to mass-produce compounded semaglutide. Enforcement deadlines hit in April and May 2025. Then on 30 April 2026, the FDA proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B Bulk Drug Substances List entirely, with a public comment period running through 29 June 2026. The FDA also issued 58 warning letters to telehealth companies and compounders in September 2025, and another 30 in March 2026, for misleading marketing.
The platforms that had built their business on $99 compounded semaglutide took two paths: exit (Ro, several others) or pivot to FDA-approved branded product at higher prices (Hims partnered with Novo Nordisk in March 2026 to offer Wegovy starting at $149/month orally, $599/month injectable). The cheap compounded window for most patients is effectively closed.
Do not believe any telehealth site still advertising injectable compounded semaglutide at $99 to $150 per month as a compliant, long-term option. Either they are running on borrowed time, sourcing outside the rules, or both.
Telehealth GLP-1 program with provider visits and pharmacy coordination.
How does Ozempic compare to natural GLP-1 boosters?
Your gut naturally releases GLP-1 after every meal. The volume is modest, the signal lasts minutes, and it degrades almost immediately via DPP-4. Semaglutide delivers a pharmacological amplification of that signal at roughly 200 to 300 times the exposure of endogenous GLP-1, held in the bloodstream for a week at a time.
Natural GLP-1 secretion can be nudged upward by dietary choices, but the word “nudge” is doing a lot of work there. Foods that genuinely stimulate GLP-1 release include soluble fiber sources (oats, barley, legumes, via short-chain fatty acids from gut fermentation), whey protein (one of the stronger nutritional GLP-1 stimuli, with acute responses seen in controlled feeding studies), and fermented foods that support microbiome diversity. Berberine, a plant alkaloid, has some human data showing modest GLP-1 pathway activity.
None of these produce the sustained, pharmacological appetite suppression of semaglutide. In April 2026, Stanford researchers published findings identifying a naturally occurring molecule in animal models that reduced appetite and body weight with fewer GI side effects than semaglutide. The mechanism is promising, the jump to human clinical use is years away, and the breathless “natural Ozempic” headlines that followed overstated the findings significantly.
The gap between “foods that boost GLP-1 a little” and “prescription semaglutide” is not a gap you close with a supplement stack.
What are the actual side effects of Ozempic, and do they apply to other peptides?
Ozempic carries an FDA boxed warning for thyroid C-cell tumors, based on rodent studies. It was not observed in the human trials, but rodent carcinogenicity data triggers the black box regardless. Its prescribing label also lists a real risk of pancreatitis, acute kidney injury (primarily through dehydration from nausea), and gastrointestinal effects (nausea affects roughly 20% of new users, usually peaking at dose escalation and declining over weeks). A 2024 JAMA Ophthalmology study reported elevated risk of non-arteritic anterior ischemic optic neuropathy (NAION) in patients with type 2 diabetes or overweight who were taking semaglutide, a rare but serious vision condition. FDA’s adverse event monitoring system showed 659 reports of alopecia and 389 of suicidal ideation linked to semaglutide as of May 2026, with investigations ongoing.
For research/therapy peptides, the side-effect profile is largely unknown for humans because the human trials do not exist at scale. The absence of documented side effects is not safety. It is silence. A compound with no human trial data has no human adverse event database, not because nothing goes wrong, but because no one is systematically collecting it.
What is the smartest way to use peptides for weight loss in 2026?
Start with the layer that has clinical evidence and legal clarity, and work outward from there.
The GLP-1 drug class (semaglutide, tirzepatide) has the deepest weight-loss evidence of any pharmacological class in history. That is the first and most important tier. Access it through a licensed telehealth provider who requires baseline labs, prescribes through a named pharmacy, and schedules clinical follow-up. The FDA’s compounding crackdown removed the $99 shortcut, but legitimate programs from platforms like Mochi Health, Trimi Health, MEDVi, Defy Medical, and Marek Health are available, with prices ranging from $99 to $599 per month depending on the drug, dose, and services included.
The therapy peptide tier (sermorelin, CJC-1295/ipamorelin, BPC-157 once the PCAC ruling happens in July 2026) can be added through the same type of licensed provider, layered onto a GLP-1 protocol or used independently for body composition and recovery goals. The key word is “through a licensed provider” because the grey-market vendor landscape collapsed significantly in 2025 and 2026, with the Peptide Sciences closure (March 2026) and Amino Asylum raid (June 2025) as the most visible casualties.
The research peptide tier (retatrutide, unproven injectables) is where the risk-to-evidence ratio is worst. Retatrutide is promising in Phase 2 data and actively being studied, but it is not approved, grey-market vials have failed independent lab testing, and the legal exposure for vendors is high enough that reliable supply is not guaranteed. Waiting for FDA approval is a defensible strategy here.
Personally, I would run the math differently than most people do: the $99 compounded-vial era trained buyers to think the drug is the expensive part and the clinical layer is optional overhead. In reality, the drug molecule is the cheap part. The clinician, the lab baseline, the pharmacy accountability, and the dose monitoring are what convert a molecule into a result you can actually measure.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Is Ozempic a peptide or a drug?
Both, and that is not a contradiction. Semaglutide is a 31-amino-acid peptide at the molecular level. It is also an FDA-approved prescription drug. The two categories are not mutually exclusive: many drugs are peptides, including insulin, liraglutide, and tesamorelin. “Peptide” describes the chemical structure; “drug” describes the regulatory status.
What is the difference between Ozempic and peptide therapy?
Ozempic (semaglutide) is FDA-approved with Phase 3 trial data in tens of thousands of patients. “Peptide therapy” typically refers to off-label or research-use compounds like BPC-157, CJC-1295, ipamorelin, and sermorelin, dispensed through compounding pharmacies or purchased from research vendors. These compounds are chemically peptides but lack Ozempic’s clinical evidence base and regulatory approval for weight loss.
Are there peptides that work like Ozempic for weight loss?
The GLP-1 drug class is the strongest tier. Tirzepatide (Zepbound) currently surpasses semaglutide in Phase 3 weight-loss results (22.5% vs. up to 20.7%). Retatrutide showed 24.2% in Phase 2 trials but is not yet approved. Growth hormone secretagogues (sermorelin, CJC-1295/ipamorelin) support body composition indirectly but do not produce the direct appetite suppression that GLP-1 agonists do, and their weight effects are smaller and slower.
Can you still get compounded semaglutide in 2026?
The widely available compounded semaglutide market is largely gone. The FDA removed semaglutide from the shortage list in February 2025, triggering enforcement deadlines in April and May 2025. A further proposal in April 2026 would exclude it from the 503B Bulks List entirely. Some 503A pharmacies may still compound for individual patients with documented need, but the $99 to $150 per month mass-market programs are not compliant options in 2026.
Is retatrutide available as a peptide now?
Retatrutide is available from research-use-only vendors in the US, but it is not FDA-approved. Phase 2 data showed 24.2% weight loss, and Phase 3 trials are ongoing. Independent lab testing by Finnrick failed retatrutide across 37 batches from Peptide Sciences before its March 2026 closure. Buying it from a grey-market vendor carries real purity and identity risk, with no prescriber, pharmacist, or accountable third party in the chain.
Do peptides work for weight loss without Ozempic?
Some do, modestly and indirectly. Growth hormone secretagogues improve body composition over months. BPC-157 may support gut function, which can affect metabolic health. But no research peptide has produced GLP-1-class weight loss numbers in human trials, and comparison claims that circulate in forums are almost always based on animal studies or anecdote. For clinically meaningful weight loss, the GLP-1 drug class has no peer in the peptide world as of mid-2026.
What is the safest peptide route for weight loss in 2026?
A licensed telehealth provider prescribing FDA-approved semaglutide or tirzepatide, through a named pharmacy, with baseline labs. That path has the best evidence, the clearest legal standing, and the most accountability. Oral semaglutide (Rybelsus) and oral tirzepatide (Foundayo/orforglipron) also now provide alternatives for injection-averse patients.
Telehealth GLP-1 program with provider visits and pharmacy coordination.
Author: [CAN XAC NHAN: ten + credential]. Educational content only, not medical advice. Sources linked inline.
Primary sources:
– Semaglutide Wikipedia / molecular structure
– PMC semaglutide GLP-1 receptor agonist review
– STEP UP trial semaglutide 7.2 mg weight loss data
– SURMOUNT-1 tirzepatide trial, NEJM
– FDA clarification on GLP-1 compounding / shortage resolution
– FDA proposal to exclude semaglutide from 503B Bulks List, April 2026
– JAMA Ophthalmology NAION and semaglutide
– Stanford natural GLP-1 molecule research, April 2026
– GoodRx: new weight loss drugs pipeline 2026
– Telehealth GLP-1 program pricing comparison 2026
– FDA peptide reclassification 2026 (BPC-157, compounding)
Want a real clinician to run the numbers, not a guess?
Joi + Blokes is a telehealth clinic that prescribes GLP-1 medication (Zepbound, compounded semaglutide and tirzepatide), hormone therapy (TRT, HRT), thyroid care, and peptides after a real lab panel and clinician review, with no membership or consult fee (prescriptions from about $59/month, lab panels from $149). If the scale will not budge, this is where you find out whether insulin, thyroid, or hormones are the real reason. Here is Joi + Blokes reviewed in full.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


