Last updated 18 June 2026. Educational content only, not medical advice. Talk to a licensed dermatologist or telehealth clinician before starting any hair loss treatment.
Short answer: The best-evidenced peptide you can buy and apply today is GHK-Cu (copper peptide), with 10% topical formulations showing a mean gain of +12 hairs per cm² over 150 days and a 93% reduction in shedding in double-blind testing. If you are looking at the pipeline, PP405 produced a 20%-plus density increase in 31% of treated men in Phase 2a trials after just 4 weeks, but it is not available yet and will not be until at least 2027.
GHK-Cu shows strong regrowth data for men. Before you start, see what’s actually behind your hair loss. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Approximately 40% of men show significant hair loss by age 35. By 50, that figure climbs past half. By 70, roughly 80% of Caucasian men have lost meaningful density, all driven by the same underlying mechanism: dihydrotestosterone (DHT) binding to androgen receptors in scalp follicles and triggering progressive miniaturization until the follicle simply stops producing visible hair (NCBI/NIH).
Minoxidil and finasteride work. That is not the question. The question most men are actually asking in 2026 is whether there is something that works without the scalp itch, the sexual side-effect profile of oral finasteride, and the “you have to do this forever or lose everything you gained” commitment that both drugs require. Peptides are not a replacement for those tools. But for the right person at the right stage of loss, the copper peptide class in particular offers a genuinely different mechanism and a side-effect profile that is almost completely clean.
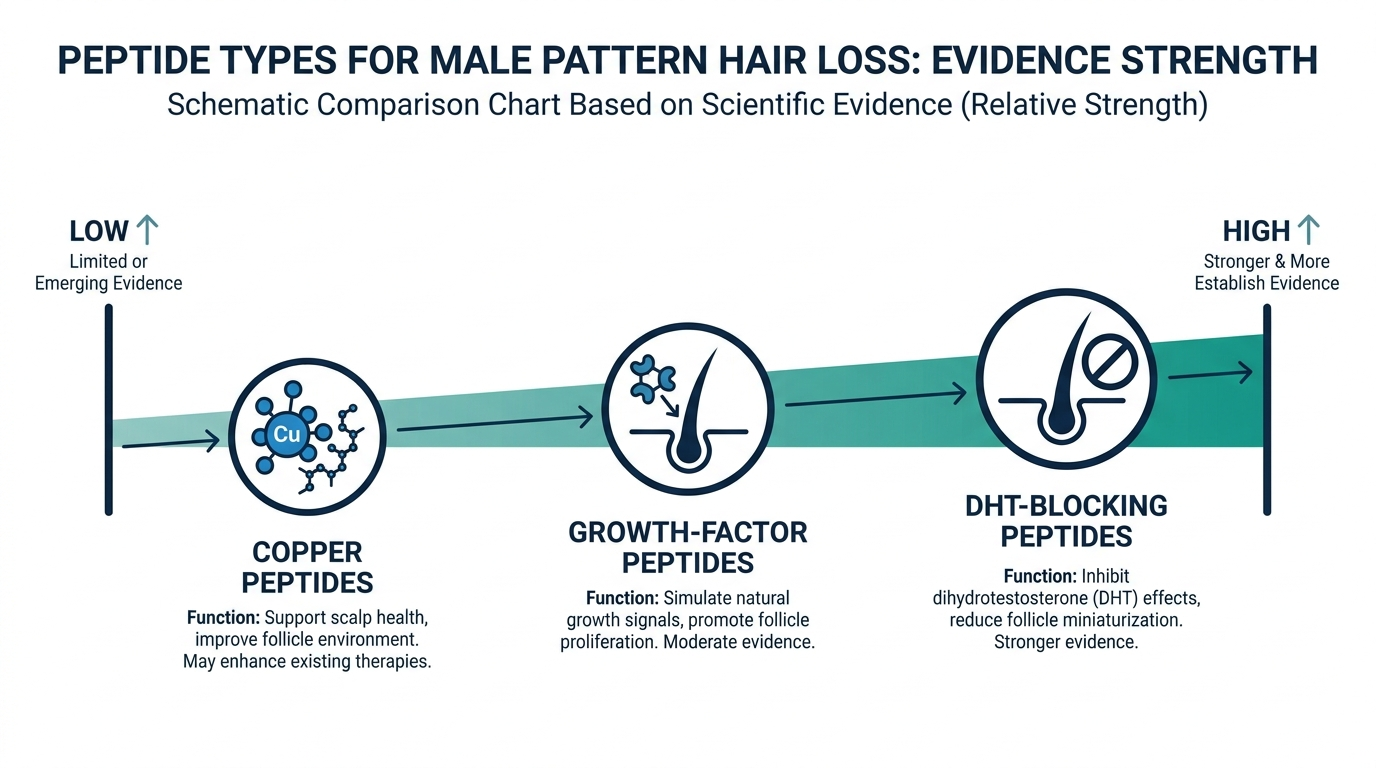
Here is the honest map, ranked by how much human evidence exists.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
What does DHT actually do to a hair follicle?
Understanding the mechanism matters, because different peptides interrupt it at different points, and that changes how you stack them.
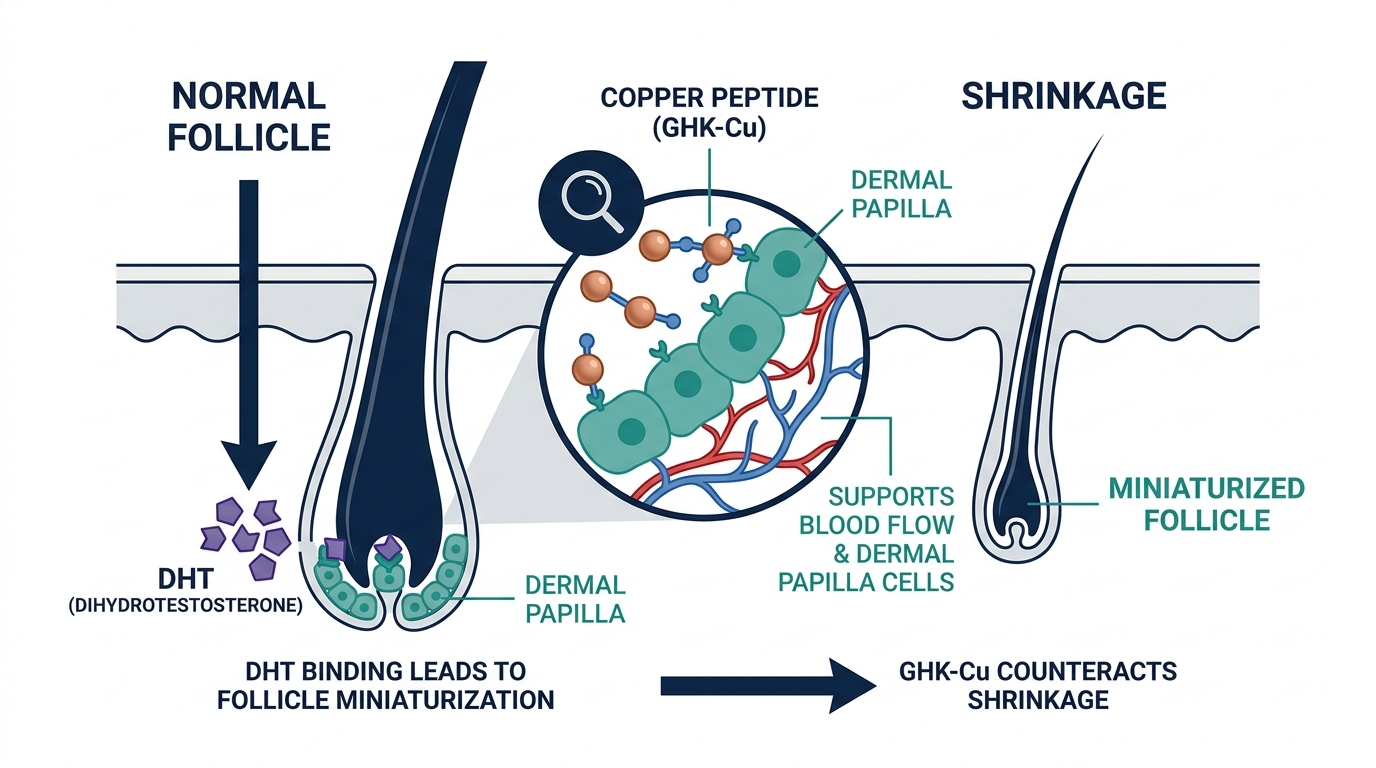
DHT is converted from testosterone by the enzyme 5-alpha-reductase inside the scalp. In men with a genetic sensitivity, DHT binds to androgen receptors in the dermal papilla cells at the base of the follicle. Over time, it shortens the anagen (active growth) phase, extends the telogen (resting) phase, and physically shrinks the follicle diameter. A follicle that once produced a thick 80-micron terminal hair begins producing a fine 20-micron vellus hair, and eventually nothing at all.
Finasteride blocks 5-alpha-reductase, reducing scalp DHT by roughly 60 to 70%. Minoxidil opens potassium channels to increase blood flow and extend the anagen phase. Neither one repairs the follicle. They slow the process and, in the early-to-mid stages, partially reverse it.
Peptides can work at three other points: re-activating Wnt/beta-catenin signaling (which the follicle needs to stay in anagen), reducing perifollicular inflammation (a major but underappreciated driver of miniaturization), and directly stimulating dermal papilla cell proliferation. That is why the most common clinical approach in 2026 is not peptides-or-minoxidil but peptides-alongside-minoxidil, addressing both the vascular and the cellular layers.
Which peptide has the most hair evidence in humans?
GHK-Cu (Glycyl-L-Histidyl-L-Lysine Copper): the best-documented option you can buy
GHK-Cu is a naturally occurring tripeptide. Your body produces it, but levels drop significantly with age: roughly 200 ng/mL at age 20, falling to around 80 ng/mL by age 60 (Formblends/peptide-hub). That age-related decline maps closely onto when most men begin noticing diffuse thinning, which is worth noting even if it is not the sole cause.
The mechanism is unusually broad for a single molecule. GHK-Cu activates Wnt/beta-catenin signaling in dermal papilla cells, promotes the production of vascular endothelial growth factor (VEGF) to increase follicular blood supply, reduces the inflammatory signaling that drives miniaturization, and has been shown in human-derived tissue to reduce premature catagen entry (the shift from growth to resting phase). In mouse models, follicle enlargement was comparable to or exceeded 5% minoxidil.
For human evidence: a 150-day double-blind trial of 120 participants using a 10% GHK-Cu serum reported 93% shedding reduction and a mean gain of +12 hairs per cm². A 2025 microneedling-assisted study showed a 26.5% median scalp coverage improvement as scored by blinded dermatologists, though it lacked a traditional control group. The critical limitation everyone should know: large, multi-center, placebo-controlled randomized controlled trials for GHK-Cu in androgenetic alopecia still do not exist. The evidence is genuinely promising and not yet conclusive.
Topical delivery is the accessible route. Concentrations of 0.5% to 2% are the standard cosmetic range. Products reaching 10% GHK-Cu now exist, including Hairgenetix’s serum (10% GHK-Cu + 5% AHK-Cu, around EUR 49.95), Neurogan’s spray formula (4% / 2400 mg, around USD 59), and PeptideLabz’s dropper (10% GHK-Cu + 5% AHK-Cu, around USD 35). One thing the product pages tend not to mention: standard topical formulations have very poor penetration to the dermal papilla, the cells that actually matter. A 2023 study showed microneedle-assisted delivery increased GHK-Cu absorption from near-zero to 134 nanomoles within nine hours, a greater than 20-fold improvement (Hairgenetix science page). If you are serious about topical copper peptides, a 0.25 mm to 0.5 mm dermaroller used once a week and the serum applied immediately after is a meaningfully different intervention than serum alone.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
AHK-Cu (L-Alanyl-L-Histidyl-L-Lysine Copper): GHK-Cu’s quieter, often-overlooked partner
AHK-Cu is a structural analog of GHK-Cu that operates through overlapping but distinct pathways. Where GHK-Cu’s primary action is anti-inflammatory and follicle-stimulatory, AHK-Cu shows stronger anti-apoptotic activity, meaning it protects dermal papilla cells from programmed cell death. It also has documented VEGF-stimulating effects, supporting the perifollicular vasculature that DHT-damaged follicles lose over time.
A 2025 pilot study from Tokyo Medical University compared 2.5% minoxidil combined with 0.025% AHK-Cu against each compound alone at full strength. The combination group showed +31.4 hairs per cm² gain, outperforming either compound in isolation (Canada Peptide). This is why most of the better formulated serums now pair GHK-Cu and AHK-Cu rather than using either alone.
Personally, I find AHK-Cu the more interesting molecule for men specifically, because DHT-driven miniaturization is fundamentally a cell-death process at the follicle level. A peptide that interrupts apoptosis is hitting the problem at exactly the right point.
Acetyl Tetrapeptide-3: the one with a head-to-head vs. minoxidil trial
Acetyl Tetrapeptide-3 (INCI: Acetyl Tetrapeptide-3) works differently from the copper peptides. It strengthens the extracellular matrix proteins surrounding the hair follicle anchor zone, which is one of the less-discussed reasons follicles miniaturize: the structural scaffold holding them in place degrades.
A 2020 randomized triple-blind controlled trial over 24 weeks compared a combination of acetyl tetrapeptide-3, biochanin A, and Panax ginseng extract against 3% minoxidil solution in 32 subjects with mild to moderate androgenetic alopecia. Terminal hair count increased 8.3% in the peptide group versus 8.7% in the minoxidil group, a statistically equivalent result. The peptide group had zero adverse reactions; one person in the minoxidil group developed scalp eczema (PMC full text). That is not a headline comparing to 5% minoxidil or the finasteride+minoxidil stack, which produces around +29.68 hairs per cm² at 24 weeks in the network meta-analysis data. But for men who cannot tolerate topical minoxidil, acetyl tetrapeptide-3 is the peptide with the most direct clinical comparison.
What is the most exciting peptide in the pipeline?
PP405: a genuinely different mechanism, not available yet
PP405 (developed by Pelage Pharmaceuticals) works through a mechanism unrelated to any existing hair loss drug: it blocks the mitochondrial pyruvate carrier (MPC), which forces follicle stem cells to shift their energy production toward lactate. That lactate surge is the natural metabolic signal that wakes dormant follicles and initiates a new growth cycle. No hormones, no vasodilation, just a metabolic switch at the stem cell level.
Phase 2a results: 31% of treated men showed a greater than 20% increase in hair density after 4 weeks of daily application, versus 0% in the placebo group. The hair produced was terminal, not vellus. No systemic absorption was detected in blood tests. The company received $120 million in Series B funding in October 2025 and is planning Phase 3 trials in 2026 (PeptideDeck).
The important caveat: PP405 is entirely unavailable. FDA approval is the earliest 2027 to 2029 scenario. Any product you find marketed online as “PP405” right now is not the genuine compound.
PTD-DBM: the Wnt pathway approach, promising but very early
PTD-DBM disrupts the binding of CXXC5 to Dishevelled proteins, effectively removing a brake on Wnt/beta-catenin signaling. In mouse models it stimulated both hair regrowth and follicle neogenesis (creation of new follicles from skin cells, a capability that minoxidil and finasteride cannot match). The original research comes from Yonsei University’s Choi lab.
As of June 2026, no completed peer-reviewed human efficacy trial exists for PTD-DBM in any hair loss indication. A spinout called CosmeRNA/Epi Biotech has produced cosmetic formulations in South Korea, but these are not FDA-reviewed. Research-peptide vendors sell it online under “research use only” labeling. The gap between mouse-model follicle neogenesis and human clinical results is the specific gap the entire peptide field runs into repeatedly, and it is real (Wikipedia PTD-DBM).
Do not believe any source claiming PTD-DBM is proven to regrow hair in humans. It is not. It is interesting and worth watching, but not worth paying for injections outside a clinical setting in 2026.
Peptides for men’s hair growth: evidence comparison
| Peptide | Mechanism | Availability | Strongest human evidence | Side-effect risk |
|---|---|---|---|---|
| GHK-Cu | Wnt/beta-catenin, VEGF, anti-inflammatory | Topical serum (OTC) | 150-day RCT: +12 hairs/cm², 93% shedding reduction | Minimal (mild scalp irritation possible) |
| AHK-Cu | Anti-apoptotic, VEGF, ECM support | Topical serum (OTC), often paired with GHK-Cu | Combo with minoxidil: +31.4 hairs/cm² pilot | Minimal |
| Acetyl Tetrapeptide-3 | ECM strengthening, follicle anchoring | Topical serum (OTC) | Non-inferior to 3% minoxidil at 24 weeks (RCT, 32 subjects) | None reported in trials |
| PTD-DBM | Wnt/beta-catenin (CXXC5 inhibitor) | Research peptide vendors (not legal for human use) | Mouse models only; no human RCT | Unknown in humans |
| PP405 | Mitochondrial pyruvate carrier blockade | Not available (Phase 3 pending) | Phase 2a: 20%+ density in 31% of men at 4 weeks | No systemic adverse events in trials |
| GHK-Cu + minoxidil | Dual: cellular + vascular | Prescription (minoxidil) + topical peptide | Most common clinical combination in 2026 | Minoxidil’s usual profile |
Can peptides work alongside minoxidil and finasteride?
Yes, and in clinical practice, this is the standard recommendation. The 2025 network meta-analysis in Frontiers in Medicine found the finasteride-plus-minoxidil combination produced +29.68 hairs per cm² at 24 weeks, the strongest result in the reviewed RCT pool (Frontiers in Medicine). Adding a copper peptide serum to that stack targets a third mechanism (follicular cell health and inflammation) that neither drug addresses. There is no published interaction concern between topical GHK-Cu and topical minoxidil applied at different times.
The sensible protocol most telehealth hair clinics now use: oral or topical minoxidil as the vascular driver, low-dose topical finasteride to address DHT locally without the systemic hormonal exposure of the oral tablet, and a copper peptide serum applied after microneedling sessions every two to four weeks. PDRN (polydeoxyribonucleotide) injections, which produced +17.9% hair count and +13.5% thickness in clinical trials, are increasingly added as an injectable component when the budget allows (PDRN Care).
None of this is something you should design yourself. A licensed dermatologist or telehealth hair clinic should be setting doses and confirming your labs before you combine prescription and non-prescription elements.
What is the myth about copper peptides being “natural” and therefore safe at any dose?
Here is the one that costs people results: because GHK-Cu is a naturally occurring peptide your body makes, many men assume more is always better. That is wrong. Copper is also a metal that participates in free radical chemistry. At excessive concentrations, copper can generate oxidative stress rather than reducing it. The cosmetic-grade window for topical GHK-Cu is 0.5% to 2% for daily application. The high-concentration serums reaching 10% are designed for periodic use, post-microneedling, not daily full-scalp saturation. Using a 10% serum twice daily as a “stronger must be better” approach introduces unnecessary copper load and can cause scalp inflammation that counteracts the peptide’s anti-inflammatory action.
The insider version of this: the reason most clinical studies showing strong results pair copper peptide application with microneedling is not just that microneedling improves penetration. It is that microneedling is done on a schedule (every two to four weeks), which creates a natural ceiling on exposure. The peptide stays in therapeutic territory. Daily high-dose application without the delivery-limiting factor of intact skin barrier is a different pharmacokinetic profile, and not necessarily a better one.
When do peptides genuinely not work for hair loss?
Peptides are useful for active, miniaturizing follicles. They cannot regrow hair from follicles that are completely dead. The clinical indicator for whether a follicle is still functional is a trichoscopy exam, which a dermatologist performs with a dermoscope. Areas where you can still see fine vellus hairs or where miniaturized follicles are visible are candidates for peptide-based stimulation. Areas that are fully smooth and shiny with no follicular openings visible at all have, in most cases, no follicles to stimulate.
This is why starting earlier matters more with peptides than with any other hair loss intervention. Finasteride can stabilize loss and partially recover even moderate miniaturization. Copper peptides at a follicle that is 60% miniaturized have considerably more to work with than copper peptides at a follicle that has been miniaturizing for 15 years. The practical translation: if you are in your late 20s or 30s noticing diffuse thinning, peptides are a realistic tool. If you are looking at areas of complete baldness in your 50s, no topical peptide is going to help there.
What about injectable peptides for hair? The telehealth route
For men who want a monitored, clinical approach, several telehealth platforms now offer injectable peptide therapy for hair. PDRN mesotherapy is the most widely available option, typically administered as a series of 12 weekly sessions. A licensed provider injects very small amounts directly into the scalp dermis, bypassing the penetration problem entirely. This is a different risk profile and a different evidence base than topical cosmetic serums, and it requires a clinical consultation, baseline bloodwork, and ongoing follow-up.
Platforms including Defy Medical, Marek Health, and Hone Health offer hair-focused peptide protocols as part of broader optimization programs. A full consultation with lab review typically costs $150 to $300 upfront, with ongoing injection sessions from $199 to $399 per month. The critical question to ask any provider: what specific pharmacy compound are you using, what is the lot number, and can I see the COA? Any clinic that cannot answer that immediately is not operating at the standard you should expect.
For any peptide that is still labeled “research use only” (which includes most injectable peptides not on the prescription list), the safety angle is real, not procedural. The FDA labeling exists because the safety-and-efficacy evidence in humans has not cleared the bar for approval. That gap is closing for several molecules, but it has not closed yet.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
Turn what you just learned into action.
Superpower lets you test 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
What is the best peptide for men’s hair growth in 2026?
GHK-Cu is the best-supported option available without a prescription, backed by a 150-day double-blind trial showing +12 hairs per cm² and 93% shedding reduction. For the most evidence per dollar, a serum combining 10% GHK-Cu and 5% AHK-Cu, applied after dermaroller sessions every two to four weeks, is the practical standard. PP405 is the most exciting molecule in the pipeline but will not be available before 2027 at the earliest.
Is GHK-Cu as good as minoxidil?
Not in head-to-head evidence volume. Minoxidil has decades of multi-center RCT data and FDA approval. GHK-Cu has a promising but smaller human evidence base. The stronger clinical argument is that GHK-Cu works through a different mechanism and is often used alongside minoxidil for additive effect, rather than as a replacement. A 2025 pilot study found that combining AHK-Cu (a related copper peptide) with low-dose minoxidil outperformed either alone.
Can copper peptides regrow hair in bald areas?
Only if the follicles are still present and merely miniaturized. A trichoscopy exam, performed by a dermatologist, is the only way to confirm whether a visible bald area still contains dormant follicles. Copper peptides cannot regenerate follicles from scratch; that is the mechanism that PTD-DBM and PP405 are being developed for.
Are there any side effects from copper peptide hair serums?
The side-effect profile is minimal: mild scalp redness or irritation in some users, usually attributable to the delivery vehicle rather than the copper peptide itself. The theoretical risk of excessive copper at very high concentrations causing oxidative stress is real but not documented as a clinical problem at cosmetic concentrations. Do not use 10% formulations daily; reserve them for post-microneedling sessions.
What is PTD-DBM and should I try it?
PTD-DBM is a synthetic peptide that blocks a negative regulator of the Wnt/beta-catenin pathway, showing follicle neogenesis in mouse models. It has no completed human RCTs as of June 2026, and the products sold online carry “research use only” labeling meaning they are not approved for human injection. Wait for human trial data before spending money here.
How long do peptide hair serums take to work?
Minimum three months to evaluate any change, six months for a realistic assessment. This matches the hair growth cycle: the anagen phase runs three to seven years, but the visible effect of follicle stimulation only manifests after the follicle has cycled through. A three-month photo comparison, taken in the same light and camera distance, is the minimum meaningful measurement.
Does diet affect whether peptides work for hair?
Yes, significantly. Iron deficiency, zinc deficiency, and low ferritin are among the most common reversible causes of hair thinning, and they look identical to early androgenetic alopecia. A biomarker panel that checks ferritin, zinc, thyroid (TSH and free T4), and inflammatory markers (CRP, IL-6) before you start any topical treatment identifies whether there is a nutritional driver that needs addressing first. Topical peptides have a much harder job when the building blocks for keratin synthesis are missing.
Author: Vital Signs Today Editorial Team. Educational content, not medical advice. Sources linked inline throughout.
Primary sources:
- NCBI/NIH: Male Androgenetic Alopecia, Endotext
- PMC: Epidemiological landscape of androgenetic alopecia in the US, PLOS One 2025
- PMC: Acetyl Tetrapeptide-3 vs. 3% Minoxidil RCT 2020
- Frontiers in Medicine: Network meta-analysis, minoxidil combinations 2025
- Dermatology Times: PP405 Phase 2a trial results
- PeptideDeck: PP405 complete 2026 guide
- Wikipedia: PTD-DBM
- Formblends: GHK-Cu hair growth mechanisms and delivery data
- Hairgenetix: Scientific research hub, copper peptides, PDRN, microneedling
- Canada Peptide: AHK-Cu therapeutic potential
- PDRN Care: PDRN for hair growth, clinical evidence
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.