Last updated 18 June 2026. Educational content only, not medical advice. Consult a licensed dermatologist or telehealth clinician before starting any hair loss treatment.
Short answer: The best-evidenced peptide you can buy today without a prescription is GHK-Cu (copper peptide) at 10% concentration, with one 150-day double-blind trial on 120 participants showing a mean gain of +12 hairs per cm² and a 93% reduction in shedding. For sheer breadth of clinical backing among cosmetic peptides, Capixyl (acetyl tetrapeptide-3 + red clover) runs close behind: a 4-month randomized trial in 30 men with androgenetic alopecia found it increased the anagen-to-telogen ratio by 46%, more than reversing the 33% reduction seen in the placebo group.
GHK-Cu leads the evidence for hair growth without a prescription. Want to see your own nutrient and hormone drivers first? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Hair loss is one of the areas where the gap between what the internet promises and what the evidence actually shows is widest. Forums overflow with personal success stories and before-and-after photos that may be real or may reflect the natural variation of hair cycling. Doctors still default to minoxidil and finasteride because those are the only two treatments the FDA has approved for hair loss, and they have the long trial record to prove it.
So where do peptides fit? The honest answer is: they occupy a real, specific niche, but it takes about ten minutes to understand which peptides belong in that niche, which are still pre-clinical animal data dressed up in product marketing, and which require a prescription rather than an Amazon order.
This guide gives you that map, ranked by how much human evidence exists, what each peptide actually does, and what the legal and practical path looks like to actually use it.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
Why is hair loss so resistant to treatment?
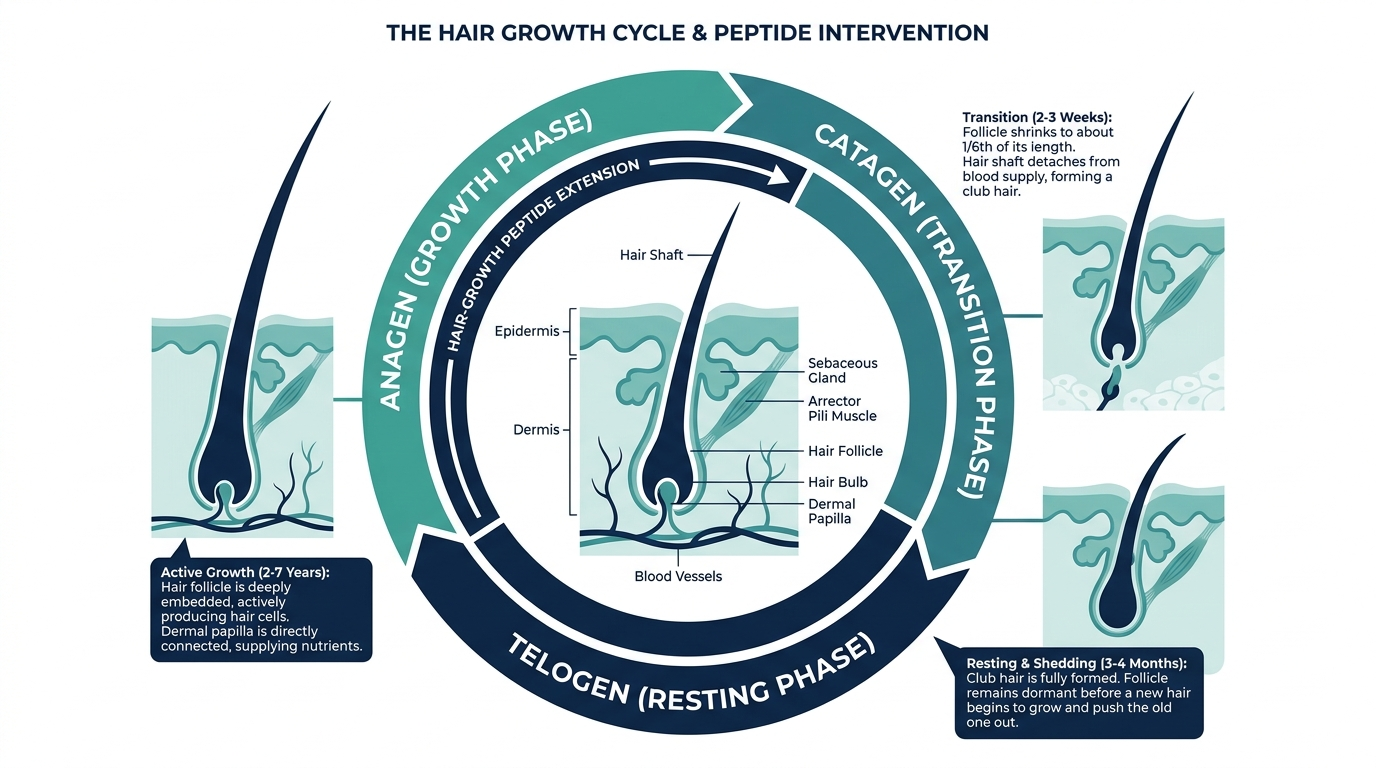
Hair follicles are not simple tubes. Each one is a cycling mini-organ with its own stem cell niche, immune privilege, and vascular supply. The growth cycle has three phases: anagen (active growth, lasting 2 to 5 years), catagen (transition, a few weeks), and telogen (rest, about 3 months). In androgenetic alopecia (pattern hair loss), dihydrotestosterone (DHT) binding to androgen receptors in susceptible follicles shortens the anagen phase from years down to months, and eventually to weeks. The follicle miniaturizes progressively, each cycle producing a thinner, shorter hair until the follicle stops producing visible hair entirely.
Two additional failure modes matter for understanding why peptides work where minoxidil plateaus. First, microvascular loss: miniaturizing follicles lose their perifollicular vasculature, so nutrients simply do not reach the papilla. Second, chronic low-grade scalp inflammation: inflammatory cells accumulate around the follicle bulge in early androgenetic alopecia, disrupting the stem cell environment. Minoxidil primarily addresses vasodilation. Peptides, depending on the type, address signaling, structural support, or both, which is why they can stack with, rather than merely duplicate, the established drugs.
The mechanisms are genuinely different. That distinction matters more than the brand names do.
Which peptide has the best clinical evidence for hair growth?
Here is the honest ranking, weighted by the quality and scale of human trials rather than marketing claims.
1. GHK-Cu (copper peptide): the strongest overall evidence base
GHK-Cu is a tripeptide (glycine-histidine-lysine) naturally chelated to copper. It is endogenous, meaning your body makes it, and its plasma concentration drops by more than 60% between age 20 and age 60, which gives it a biological plausibility that purely synthetic peptides lack.
For hair, GHK-Cu works through at least three distinct pathways. It stimulates VEGF (vascular endothelial growth factor) production, rebuilding the perifollicular vasculature that miniaturizing follicles lose. It inhibits TGF-beta, a growth factor that pushes follicles into the catagen (termination) phase prematurely. And it directly activates Wnt/beta-catenin signaling in dermal papilla cells, which is the same pathway that gives hair its instructions to grow.
Early animal research published in the Annals of Dermatology (PubMed ID 1809108) showed hair follicle enlargement in mouse models with results described as comparable to or exceeding 5% minoxidil. An in vitro study using cultured human follicles (PubMed ID 17703734) documented a reduced rate of premature catagen entry, validating the TGF-beta inhibition mechanism in actual human tissue.
The most recent human trial, a 2025 microneedling-assisted application study in 120 participants over 150 days, reported median scalp coverage regrowth of 26.5%, 93% shedding reduction, and a mean density gain of +12 hairs per cm², assessed by both blinded dermatologists and AI-assisted image analysis. Crucially, that study used a 10% GHK-Cu concentration applied with a microneedling device, because standard topical application delivers near-zero absorption. With microneedling-assisted delivery, GHK-Cu absorption reaches 134 nanomoles within nine hours, more than a 20-fold improvement over topical-only methods.
Do not believe the simplified version that says “just rub copper peptide on your scalp and wait.” The delivery method is half the mechanism. Topical-only at low concentrations has much weaker evidence.
2. Capixyl (acetyl tetrapeptide-3 + red clover extract): best cosmetic-grade evidence
Capixyl is a patented complex from Lucas Meyer Cosmetics combining acetyl tetrapeptide-3, a synthetic peptide that stimulates laminin-5 and collagen IV around the follicle bulge, with red clover isoflavone extract that inhibits 5-alpha-reductase and reduces DHT-driven inflammation in the scalp.
The Sederma-sponsored 4-month study (30 men with androgenetic alopecia, 5% Capixyl lotion versus placebo, 20 drops daily) found the active group increased their anagen-to-telogen ratio by 46%, while the placebo group saw a 33% reduction. That head-to-head direction of effect is clinically meaningful.
Two caveats worth noting. First, the trial was industry-sponsored. Second, 30 participants is a small cohort, and single-site studies are harder to generalize. Still, a 46% improvement in the anagen-telogen balance is not a minor signal, and it captures a real, measurable biological endpoint rather than a subjective satisfaction score.
Capixyl appears in higher-end serums and is often combined with Redensyl, Procapil, and high-solubility caffeine. The Ordinary’s Multi-Peptide Serum for Hair Density (around $22 to $25 for 60 mL at Sephora, Target, or Ulta) stacks Redensyl, Capixyl, Procapil, Baicapil, and AnaGain together at accessible price points, making it one of the few mass-market formulas that addresses multiple pathways simultaneously.
3. Biotinoyl tripeptide-1 (the anchoring peptide in Procapil): strongest anti-shedding data
Biotinoyl tripeptide-1 is a biotin-conjugated tripeptide that anchors hair follicles to the dermal matrix by stimulating adhesion proteins around the follicle base. Sederma’s formulated Procapil complex, which pairs biotinoyl tripeptide-1 with apigenin (an anti-inflammatory flavonoid) and oleanolic acid (a DHT blocker from olive leaf), reported up to 58% reduction in hair loss in 4-month sponsor trials.
A 2025 randomized head-to-head comparison (MDPI Cosmetics, doi: 10.3390/cosmetics12040152) of a topical and oral combination therapy containing oleanolic acid, apigenin, and biotinyl tripeptide-1 in androgenetic alopecia patients found statistically significant improvements in hair density and shaft diameter over 24 weeks. The key insight from that paper: the combination (topical plus oral) outperformed topical alone, suggesting the pathway this peptide targets benefits from systemic reinforcement.
Separately, in vitro studies on human dermal papilla cells exposed to biotinoyl tripeptide-1 serum at concentrations of 0.625% and 1.25% showed cell proliferation rates of 148% and 143% respectively compared to controls, with 5-alpha-reductase inhibition at 1.25% that matched minoxidil-level activity in the same model.
The caveat here is the same as with Capixyl: in vitro and company-sponsored in vivo data differ from large, independent, multi-center RCTs. The signal is real; the effect size in real-world scalps is probably more modest.
4. Redensyl (DHQG + EGCG2): fastest-acting peptide-adjacent complex
Redensyl is not a classic peptide but rather a two-molecule complex: DHQG, a dihydroquercetin-glucoside targeting hair follicle stem cells, and EGCG2, an epigallocatechin gallate-glucoside derivative that reduces apoptosis in outer root sheath cells. It is grouped with hair peptides in the market because it activates some of the same Wnt signaling cascades.
The Induchem-funded trial applied 3% Redensyl once daily for 3 months in a 26-participant cohort and found 85% of volunteers showed clinical improvements, with an average of +9% anagen hair, minus 17% telogen hair, and +8% increase in hair density corresponding to roughly +10,000 new hairs across the entire scalp.
That last number (10,000 new hairs) is regularly quoted without context. The full scalp has around 100,000 hairs, so an 8% density increase means about 8,000 to 10,000 hairs that shifted from telogen back into anagen, not 10,000 new follicles. Worth knowing.
5. PTD-DBM (CXXC5 inhibitor): most exciting pipeline molecule, no human RCT yet
PTD-DBM is a cell-penetrating peptide that inhibits CXXC5, a negative regulator of Wnt/beta-catenin signaling. A landmark 2023 study published in Cells demonstrated dose-dependent increases in CXXC5 expression following DHT treatment, corresponding decreases in beta-catenin, and restoration of Wnt signaling with PTD-DBM treatment. CXXC5 knockout mice showed complete resistance to DHT-induced hair loss in that model.
The problem: as of June 2026, no published randomized controlled trial in humans exists for PTD-DBM. All efficacy data come from animal models and cell culture. It is the most mechanistically compelling peptide on this list. It is also the one where the gap between forum enthusiasm and actual clinical proof is largest.
Anyone selling injectable PTD-DBM “for research use” and implying it will regrow hair is working from animal studies only. That is not automatically wrong, but it is not the same as controlled human evidence.
How do the top hair peptides compare?
| Peptide | Best Human Evidence | Effect Size | OTC / Rx | Approximate Price | Strongest Limitation |
|---|---|---|---|---|---|
| GHK-Cu 10% + microneedling | 120-person, 150-day double-blind | +12 hairs/cm², 93% shedding reduction | OTC | $50 to $80 (serum + device) | Delivery-dependent; topical-only is weaker |
| Capixyl (5%) | 30-person RCT, 4 months | +46% anagen/telogen ratio vs. placebo | OTC | $22 to $65 (in multi-actives) | Industry-sponsored, small N |
| Biotinoyl tripeptide-1 / Procapil | 24-week open-label combination trial, 2025 | Significant density + shaft diameter gain | OTC | $22 to $40 (in formulas) | No independent large-scale RCT |
| Redensyl (3%) | 26-person, 3-month sponsored | +8% density (~10,000 hairs shifted to anagen) | OTC | $22 to $50 (in multi-actives) | Industry-sponsored, small N |
| PTD-DBM | Animal models only (as of June 2026) | 100% prevention in CXXC5 knockout mice | Research / grey zone | Variable, research vials | Zero human RCT data |
| GHK-Cu injectable (prescription) | Compounding pharmacy route | Same molecule; potentially higher bioavailability | Rx via telehealth | $225/50 mg dose | Regulatory grey zone post-April 2026 reclassification |
What about growth hormone peptides like sermorelin?
This one trips people up. Sermorelin is a growth hormone-releasing hormone analogue, not a hair-specific peptide. Its mechanism is systemic: it increases circulating growth hormone, which raises IGF-1. IGF-1 directly stimulates hair matrix keratinocyte proliferation and extends the anagen phase by activating the PI3K/AKT pathway in follicle cells.
The 2025 MDPI paper on IGF-1 and hair regeneration (doi: 10.3390/cimb47090773) confirmed that follicles in androgenetic alopecia show reduced IGF-1 responsiveness, so raising systemic IGF-1 through sermorelin may support the follicular environment, particularly in patients with documented growth hormone deficiency.
Personally, I would not use sermorelin as a hair-first intervention. It is a systemic hormone modulator requiring a prescription and clinical monitoring, and its effect on hair, while mechanistically plausible, is indirect, slow, and poorly quantified for hair endpoints. The better use case for sermorelin is someone who has both growth hormone deficiency and thinning hair, and who is working with a clinician who can track both IGF-1 levels and hair density over time.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
Is there a delivery method myth worth busting?
Yes, and it is a significant one. Most people buy a copper peptide serum, apply it to dry scalp, and expect the 12-hair-per-cm² result from the clinical trial. That is not what the trial tested.
The 2025 GHK-Cu trial that produced those numbers used a microneedling-assisted delivery protocol. Standard topical application of a large peptide molecule onto intact skin delivers near-zero systemic absorption. Microneedling creates temporary microchannels in the stratum corneum, and measured GHK-Cu absorption jumps from near-zero to 134 nanomoles within nine hours under that method. A 20-fold difference in delivery is not a minor optimization. It is the protocol.
At-home dermarollers (0.25 to 0.5 mm) and electric microneedling stamps are widely available for $20 to $90. The Hairgenetix system, which bundles a 10% GHK-Cu + 5% AHK-Cu serum with a mesotherapy delivery device, is priced at approximately $50 (product) plus the device, and is the only off-the-shelf combination specifically built around microneedling-assisted copper peptide delivery as of the 2026 buyer’s guide. Neurogan Health’s GHK-Cu Hair and Scalp Serum (4% GHK-Cu, approximately $47/month subscription) works without microneedling but at lower absorption.
The practical takeaway: if you are using a GHK-Cu serum on intact scalp with no delivery assist, you are likely getting a fraction of the effect the trial measured. A $30 dermaroller changes the math more than a $100 upgrade in serum brand.
What is the legal path to prescription peptide hair therapy?
For the cosmetic peptides above (GHK-Cu topicals, Capixyl, Redensyl, biotinoyl tripeptide-1), no prescription is needed. You buy them as cosmetics or supplements.
For injectable GHK-Cu, the regulatory situation shifted meaningfully in April 2026. The FDA had placed GHK-Cu on the 503A Category 2 list (substances presenting potential safety risks, banned from compounding) in November 2023. On 22 April 2026 the FDA removed it from that list, and HHS signaled in February 2026 that GHK-Cu and approximately 13 other peptides are expected to return to Category 1 (permitted for compounding) status, pending a Pharmacy Compounding Advisory Committee meeting scheduled for 23 to 24 July 2026.
In plain terms: injectable GHK-Cu for hair is moving back toward a legitimate compounding pharmacy route, available through a physician’s prescription. Telehealth clinics such as Defy Medical, Marek Health, and Hone Health already offer broader peptide therapy programs (typically $199 to $399 per month with labs and monitoring), and injectable GHK-Cu is expected to re-enter their formularies once the July 2026 PCAC decision lands.
If someone is selling you injectable PTD-DBM or injectable GHK-Cu with no prescription, no named compounding pharmacy, and no clinical oversight, the legal and safety analysis from the broader peptide market applies. Know what you are doing, and understand that a research vial is not a clinic.
What does a real peptide hair protocol look like?
A clinically grounded protocol in 2026 layers multiple mechanisms rather than betting everything on a single ingredient, because no single peptide addresses all three failure modes (DHT pathway, vascular loss, and inflammation) at once.
A reasonable stacking approach, in order of evidence strength:
- Topical minoxidil or topical finasteride (FDA-approved, the anchor). Minoxidil 5% applied twice daily is the evidence baseline. Many patients use a compounded FollicureRX spray combining minoxidil, finasteride, and ketoconazole.
- GHK-Cu 10% serum with microneedling twice weekly. This targets the vascular and Wnt pathways minoxidil does not.
- A multi-active formula with Capixyl, Redensyl, and Procapil (the anagen anchoring and DHT-inflammation layer). The Ordinary’s Multi-Peptide Serum at $22 to $25 is a rational entry point before committing to premium-priced alternatives.
- Baseline blood panel to rule out ferritin below 70 ng/mL (associated with telogen effluvium in women and men), thyroid dysfunction, and inflammatory markers that amplify follicle loss.
Personally, I think the biggest mistake people make is skipping step 4 and spending $300 on serums while a ferritin of 28 ng/mL is driving the shedding. A biomarker panel is not glamorous, but it is the only way to know whether the root cause is even addressable topically.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
What is the best peptide for hair growth overall?
By the current weight of human evidence, GHK-Cu at 10% concentration used with microneedling-assisted delivery has the strongest combined data: +12 hairs per cm², 93% shedding reduction, and 26.5% scalp coverage improvement at 150 days in a 120-person double-blind trial. Capixyl is the best-evidenced cosmetic-grade peptide for improving the anagen-to-telogen ratio specifically.
Do peptides regrow hair that is already gone?
Peptides work best on follicles that are miniaturizing but still alive. Once a follicle is completely scarred and non-functional, no topical or injectable peptide will regenerate it. This is why earlier intervention produces better results. Follicle viability can be assessed by a trichoscopy (dermoscopy of the scalp) by a dermatologist, which shows whether follicle openings are still present.
Can women use the same hair growth peptides as men?
Yes. GHK-Cu, Capixyl, Redensyl, and biotinoyl tripeptide-1 are sex-neutral in mechanism and are not contraindicated in women. Topical finasteride (used alongside peptides in some compounded formulas) has a systemic absorption concern for pregnant women, so women of childbearing age should confirm with a clinician before using any finasteride-containing compound.
How long before peptides show results on hair?
The hair growth cycle means you will not see density improvements for at least 3 months, and meaningful cosmetic change typically requires 5 to 6 months of consistent use. Shedding reduction is usually the first sign that the protocol is working, often visible around 6 to 8 weeks.
Is copper peptide the same as GHK-Cu?
In the hair and skincare context, they are used interchangeably, but technically GHK-Cu is one specific copper peptide: glycine-histidine-lysine chelated with a copper (II) ion. AHK-Cu (alanine-histidine-lysine-copper) is a related copper tripeptide with similar hair follicle elongation data at picomolar concentrations, but less extensive human trial data than GHK-Cu.
Does Redensyl or Capixyl work better for hair growth?
They target different mechanisms, so they work better together than versus each other. Redensyl activates follicle stem cells; Capixyl anchors follicles to the dermal matrix and inhibits DHT-driven inflammation. Products like The Ordinary’s Multi-Peptide Serum for Hair Density include both, which is part of why that formula is a rational starting point.
What about PTD-DBM for hair regrowth?
PTD-DBM has compelling animal and cell-culture data showing it activates Wnt signaling by blocking CXXC5, a negative regulator that DHT upregulates. No published human randomized controlled trial exists as of June 2026. The 2023 Cells paper and earlier mouse models are genuinely interesting, but the clinical application is still pre-investigational. Do not mistake forum enthusiasm for a human evidence base.
Hydrolyzed type I & III collagen peptides, third-party tested, unflavored.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources:
- Hairgenetix 2025 GHK-Cu 150-day trial and buyer’s guide: https://hairgenetix.com/blogs/articles/best-copper-peptide-hair-growth-serums-2026-buyers-guide
- GHK-Cu clinical overview and telehealth pricing (Innerbody 2026): https://www.innerbody.com/ghk-cu-peptide
- GHK-Cu hair growth mechanisms and study data (FormBlends): https://formblends.com/articles/peptide-hub/ghk-cu-hair-growth-copper-peptide
- Capixyl Redensyl Procapil clinical review (PerfectHairHealth): https://perfecthairhealth.com/redensyl-capixyl-procapil-rcp-for-natural-hair-regrowth-scientific-review/
- CXXC5/PTD-DBM and DHT-induced alopecia via PGD2 (PMC): https://pmc.ncbi.nlm.nih.gov/articles/PMC9954685/
- Biotinoyl tripeptide-1 vs. minoxidil combination therapy (MDPI Cosmetics 2025): https://www.mdpi.com/2079-9284/12/4/152
- IGF-1 in hair regeneration (MDPI 2025): https://www.mdpi.com/1467-3045/47/9/773
- Wnt/beta-catenin approaches beyond minoxidil and finasteride (ACS J. Medicinal Chemistry): https://pubs.acs.org/doi/10.1021/acs.jmedchem.5c02108
- Topical alternatives for hair loss beyond conventional (PMC 2025): https://pmc.ncbi.nlm.nih.gov/articles/PMC12251978/
- FDA bulk drug substances under 503A (BPC-157 reclassification context): https://www.fda.gov/drugs/human-drug-compounding/bulk-drug-substances-used-compounding-under-section-503a-fdc-act
- The Ordinary Multi-Peptide Serum for Hair Density product page: https://theordinary.com/en-us/multi-peptide-serum-for-hair-density-hair-scalp-treatment-100434.html
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.