
Curious what your own estradiol number would say? See it alongside 100+ other biomarkers from one at-home draw. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
- Estradiol (E2) is the strongest form of estrogen, and an estradiol blood test measures how much of it is circulating in your blood, reported in picograms per milliliter (pg/mL).
- MedlinePlus lists a normal estradiol range of about 30 to 400 pg/mL for premenopausal women, 0 to 30 pg/mL after menopause, and 10 to 50 pg/mL for adult men.
- A high estradiol can point to estrogen-producing tumors or early puberty, while a low estradiol often reflects menopause, ovarian insufficiency, or very low body weight.
What is estradiol in a blood test?
Estradiol in a blood test is a measurement of estradiol (E2), the most potent and dominant estrogen in the body, reported in picograms per milliliter (pg/mL). According to MedlinePlus, the normal estradiol range is roughly 30 to 400 pg/mL for premenopausal women, 0 to 30 pg/mL for postmenopausal women, and 10 to 50 pg/mL for adult men.
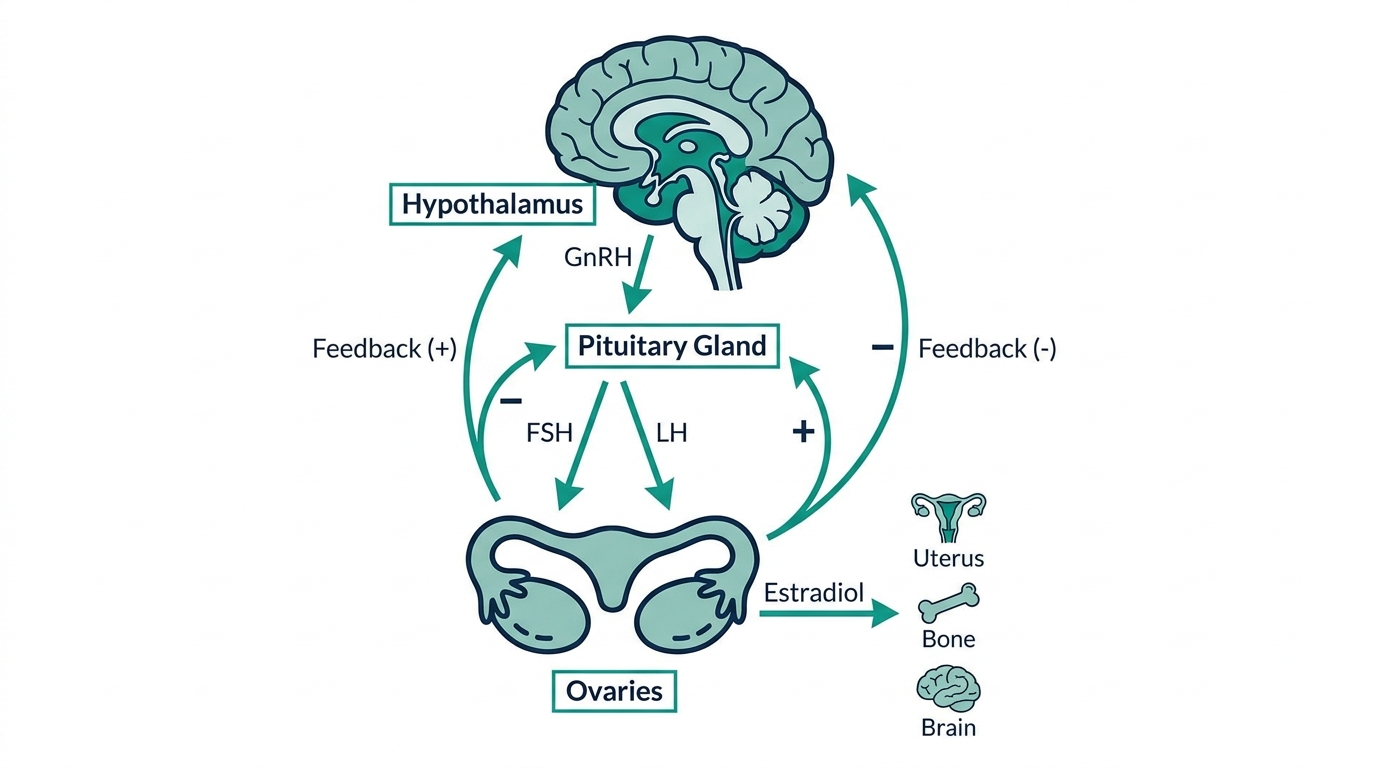
Estradiol is made mostly in the ovaries in females, and in smaller amounts by the testes and by fat tissue in males. It drives the menstrual cycle, supports the uterine lining, and helps protect bone in both sexes (Cleveland Clinic).
Why the value swings so much: in menstruating women, estradiol changes daily across the cycle, so a single number only makes sense alongside the cycle day it was drawn on.
Why is estradiol measured?
Estradiol is measured to evaluate how well the ovaries, testes, or adrenal glands are working and to investigate hormone-related symptoms. MedlinePlus notes the test is commonly used to assess fertility, abnormal puberty, menstrual problems, and the response to hormone treatment (MedlinePlus).
Clinicians order an estradiol test in situations such as:
- Fertility workups: tracking follicle development during IVF or ovulation-stimulation cycles.
- Menopause questions: confirming whether ovarian estrogen has dropped in someone with hot flashes or missed periods.
- Puberty concerns: evaluating early or delayed sexual development in children.
- Men’s health: investigating breast tissue growth (gynecomastia) or low libido, since excess estradiol can be a factor.
The Mayo Clinic Laboratories catalog also lists estradiol monitoring for people on estrogen therapy or aromatase-inhibitor treatment, where the goal is to keep levels within a target band.
What does a high estradiol mean?
A high estradiol means more estrogen is circulating than expected for your sex, age, and cycle stage. MedlinePlus states that elevated results can reflect early (precocious) puberty, an estrogen-producing tumor of the ovaries or adrenal glands, or, in men, gynecomastia and reduced testosterone balance (MedlinePlus).
Common drivers of a high reading include:
- Normal cycle surges: estradiol peaks near ovulation, reaching roughly 64 to 357 pg/mL per Mayo Clinic Laboratories, so timing matters.
- Pregnancy: levels rise far above the nonpregnant range and are not a concern on their own.
- Excess body fat: fat tissue converts other hormones into estradiol, which can raise levels in men and postmenopausal women.
- Tumors or liver disease: less common but important to rule out when the rise is unexplained.
A single high value is rarely a diagnosis. Your clinician interprets it against the full clinical picture before acting.
What does a low estradiol mean?
A low estradiol means estrogen production has fallen below the expected range, which is normal after menopause but can signal a problem in younger people. MedlinePlus reports that low results may reflect ovarian failure (early menopause), primary ovarian insufficiency, Turner syndrome, or low estrogen from rapid weight loss or anorexia (MedlinePlus).
Typical causes of a low reading include:
- Menopause: the expected drop to about 0 to 30 pg/mL once the ovaries stop producing estrogen (MedlinePlus).
- Very low body weight: intense exercise, eating disorders, or rapid weight loss can suppress ovarian function.
- Pituitary or hypothalamic issues: the brain signals that drive the ovaries can be disrupted.
- Polycystic ovary syndrome (PCOS): can produce low or atypical estradiol patterns.
Low estradiol over time matters because estrogen helps protect bone, so persistent deficiency raises the risk of bone thinning.

How is estradiol interpreted with other markers?
Estradiol is almost never read alone. Clinicians pair it with FSH (follicle-stimulating hormone) and LH (luteinizing hormone) to tell whether a low estradiol comes from the ovaries themselves or from the brain signals above them. In menopause and ovarian insufficiency, estradiol is low while FSH is high, a pattern Cleveland Clinic describes for failing ovarian function (Cleveland Clinic).
Other common companions:
- FSH and LH: separate ovarian causes from pituitary causes.
- Progesterone: read alongside estradiol to map the menstrual cycle and confirm ovulation.
- Testosterone: in men, the estradiol-to-testosterone balance matters more than estradiol alone.
- AMH: often added in fertility evaluations to estimate ovarian reserve.
This is why an isolated estradiol number, without the cycle day or partner hormones, is hard to act on.
The insider nuance: the assay you get changes the number
Here is what often gets missed: the lab method matters as much as the result. Standard immunoassays can be unreliable at very low estradiol levels, the exact range seen in men, children, and postmenopausal women. For those groups, labs increasingly use liquid chromatography mass spectrometry (LC-MS/MS), which Mayo Clinic Laboratories uses for its serum estradiol testing because it stays accurate at low concentrations (Mayo Clinic Laboratories).
Practically, this means two things. First, do not compare an estradiol result from one lab directly against a different lab’s number, because the reference ranges and methods differ. Second, if a man or a postmenopausal woman is told their estradiol is “undetectable” or oddly high on a standard assay, asking whether a sensitive (LC-MS/MS) test is appropriate can change the interpretation. Always confirm against the reference range printed on your own report.
How estradiol moves across the menstrual cycle
The single biggest reason an estradiol number confuses people is that in a menstruating woman it is a moving target, not a fixed level. Across one cycle it can swing several fold, so the same value can be perfectly normal on one day and abnormal on another. Understanding the shape of that curve is the key to reading your own result.
| Cycle phase | Approximate cycle days | What estradiol is doing |
|---|---|---|
| Early follicular | Days 1 to 5 | Lowest of the cycle, since the previous corpus luteum has broken down and a new follicle has not yet ramped up. |
| Late follicular | Days 6 to 12 | Rising steadily as the dominant follicle grows and pumps out estradiol. |
| Ovulation | Around day 13 to 14 | Peaks sharply, often the highest reading of the cycle, then triggers the LH surge that releases the egg. |
| Luteal | Days 15 to 28 | A second, smaller rise from the corpus luteum, then a fall in the days before the period if pregnancy does not occur. |
This is why a baseline estradiol is usually drawn on day 2 or 3, when the level is at its stable floor, and why ovulation tracking targets mid-cycle. It is also why comparing a mid-cycle value against an early-follicular reference range is meaningless. Two accurate results, drawn a week apart, can differ two or threefold and both be normal. Always record the cycle day next to the number.

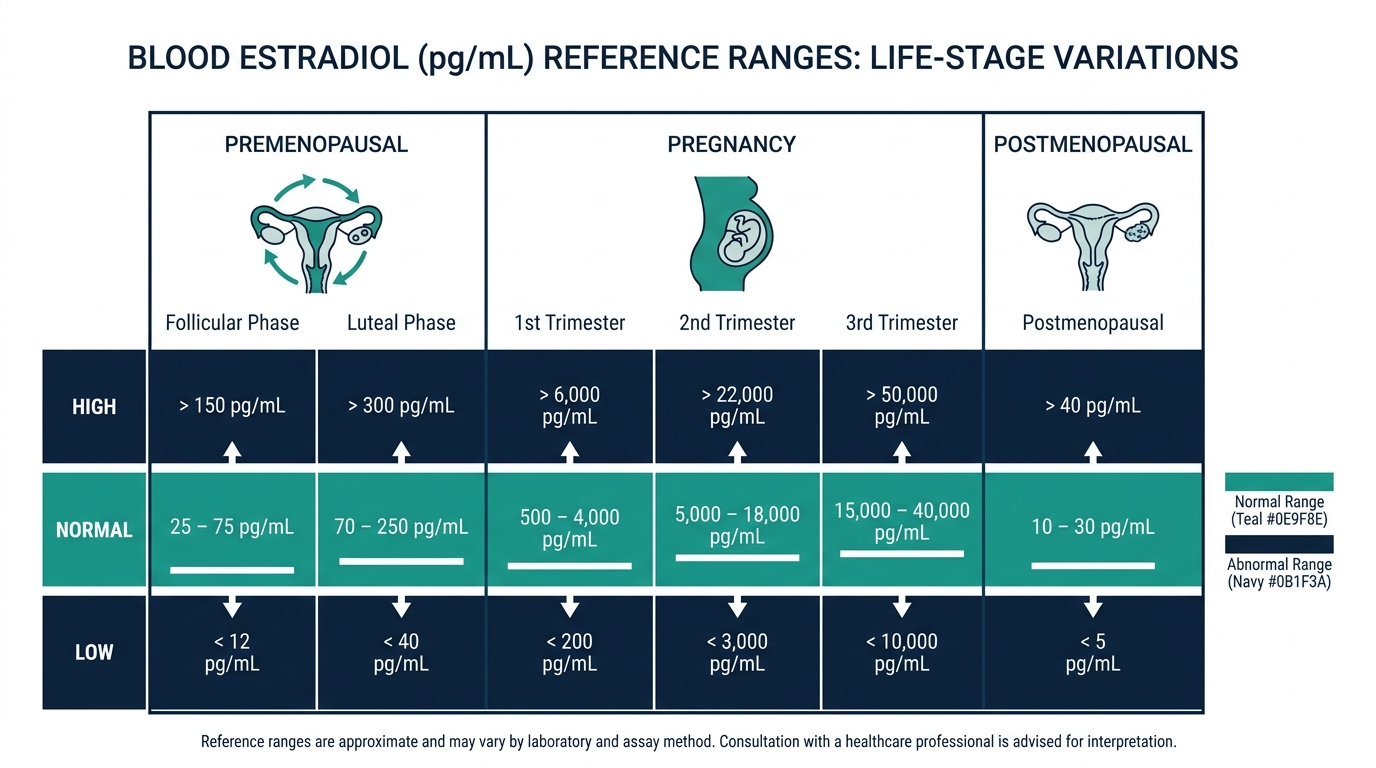
Estradiol across the stages of life
Beyond the monthly cycle, estradiol changes dramatically across a lifetime, and each stage has its own expected pattern. A result that would alarm you at one age is entirely normal at another.
- Before puberty: estradiol is very low in children. A rise before the expected age is one of the signals evaluated in precocious puberty.
- Reproductive years: the high, cyclical pattern described above, driving the menstrual cycle and supporting fertility.
- Perimenopause: often the most erratic phase, with estradiol swinging high and low from cycle to cycle as ovarian function becomes irregular. A single reading here is especially hard to interpret.
- Postmenopause: the ovaries largely stop producing estradiol, so levels settle low, generally below 30 pg/mL (MedlinePlus). Most remaining estrogen now comes from fat tissue converting other hormones.
- Men across adulthood: a low, relatively steady level in the range of about 10 to 50 pg/mL, produced partly by the testes and partly by fat tissue converting testosterone.
Because the expected value shifts so much with age and stage, the reference range printed on your report is set for your group. That is the number to compare against, not a generic adult range.
Symptoms that often prompt an estradiol test
Estradiol is usually checked because of symptoms, not as a routine screen. Knowing which complaints point toward high versus low estrogen helps you understand why the test was ordered and what the result is looking for.
Signs that can accompany low estradiol:
- Hot flashes, night sweats, and vaginal dryness, the classic menopause cluster.
- Missed or absent periods in someone still of reproductive age.
- Low mood, poor sleep, and reduced libido.
- Over the long term, accelerated bone loss, since estrogen helps preserve bone density.
Signs that can accompany high estradiol:
- Heavy or irregular menstrual bleeding.
- Breast tenderness or, in men, breast tissue growth (gynecomastia).
- Bloating and mood swings.
- In children, early breast development or other early puberty signs.
These symptoms overlap with many other conditions, which is exactly why the blood test exists. The result turns a vague complaint into a measurable value that can be tracked and treated.
Monitoring estradiol during hormone therapy
One of the most common reasons to repeat an estradiol test is to follow treatment, and the goal there is different from diagnosis. Instead of asking “is this normal,” the clinician asks “is this in the target band we set.”
- Menopausal hormone therapy: estradiol may be checked to confirm that a dose is being absorbed and is reaching a level expected to relieve symptoms without overshooting.
- Fertility treatment: during ovarian stimulation for IVF, estradiol is measured repeatedly, sometimes every day or two, because a rising level tracks how the follicles are responding. A very high level can flag a risk of overstimulation.
- Aromatase inhibitor therapy: in some breast cancer care, the aim is to keep estradiol very low, so a sensitive assay is used to confirm suppression (Mayo Clinic Laboratories).
- Gender-affirming care: estradiol is followed to keep levels within an individualized target.
In all of these, the raw number matters less than whether it lands inside the intended window. That is why treatment monitoring is scheduled at set intervals and read against a personal target rather than a population range.

Why estradiol matters beyond fertility
It is easy to think of estradiol as a reproductive hormone only, but it acts throughout the body in both women and men. That wider role is why a persistently low level can carry consequences far beyond the menstrual cycle.
- Bone: estradiol slows the breakdown of bone. This is a major reason bone loss speeds up after menopause, when estradiol falls, and why long-standing low estrogen at any age raises the risk of thinning bones (Cleveland Clinic).
- Cardiovascular system: estrogen influences blood vessels and cholesterol handling, part of why heart disease patterns differ before and after menopause.
- Brain and mood: estradiol shifts affect sleep, mood, and cognition for many people, which is why symptoms in these areas often track with hormonal transitions.
- Genital and urinary tissue: estrogen maintains the tissue of the vagina and lower urinary tract, so a drop can cause dryness and discomfort.
- In men: a small amount of estradiol is necessary for bone health and libido, so both too little and too much can cause problems, which is why it is read against testosterone rather than alone.
Seen this way, an estradiol result is not just a fertility marker. It is a readout on a hormone that touches bone, heart, brain, and tissue health across the whole lifespan.
Estradiol, estrone, and estriol: the three estrogens
People often use “estrogen” and “estradiol” as if they were the same thing, but estrogen is a family and estradiol is one member. Knowing the difference explains why a result is labeled E2 and why it changes with life stage.
- Estradiol (E2): the strongest estrogen and the dominant one during the reproductive years. This is what a standard estradiol test measures (Cleveland Clinic).
- Estrone (E1): a weaker estrogen that becomes the main form after menopause, produced largely by fat tissue. It is why body fat influences estrogen levels in older women and in men.
- Estriol (E3): the weakest estrogen, produced in large amounts by the placenta during pregnancy, which is why it is measured mainly in a prenatal context.
When a report says “estradiol” or “E2,” it is measuring the potent reproductive-years form specifically, not total estrogen. This is worth checking, because a general “estrogen” order and a specific estradiol order are not identical, and the reference ranges differ.
What happens after an abnormal estradiol result
An out-of-range estradiol is a starting point, not a conclusion. The next steps depend on the direction and the clinical context, and they almost always involve more than repeating the single test.
- Recheck timing first. For a menstruating woman, the initial question is whether the draw matched the intended cycle day. A mistimed sample is often re-drawn before anything else.
- Add the partner hormones. FSH and LH separate an ovarian cause from a brain-signal cause, and progesterone helps confirm ovulation. In men, testosterone is read alongside to judge the balance.
- Look for a driver. An unexplained high value may prompt evaluation for an estrogen source such as a tumor or, more commonly, excess body fat and its conversion of hormones. A low value in a young person prompts a look at weight, exercise load, the pituitary, and ovarian reserve.
- Match the workup to the goal. Fertility, menopause, puberty, and men’s health each lead to a different set of follow-up tests, which is why there is no single “next test” after an abnormal estradiol.
The takeaway is that estradiol is one instrument in an orchestra. A clinician reads it with the surrounding hormones and your symptoms before deciding what, if anything, it means for you.
Test preparation and what can distort the result
Estradiol has fewer prep rules than a metabolic panel, but a few factors can shift the number enough to change interpretation.
- Cycle timing is the dominant factor. As covered above, the cycle day matters more than any dietary prep. A draw scheduled to the wrong day is the most common reason a result looks off.
- Fasting is usually not required, though a combined hormone panel may carry its own instructions, so follow what your clinician says (MedlinePlus).
- Medicines and hormones can move it. Birth control pills, hormone therapy, and some other drugs change estradiol, so tell the lab what you take.
- The assay method matters at low levels. For men, children, and postmenopausal women, a sensitive mass spectrometry method is more reliable than a standard immunoassay, which can be inaccurate at the low end.
- Do not compare across labs. Different methods and reference ranges mean two labs can report different numbers for the same sample. Read your value against the range on your own report.
Questions people ask most after an estradiol result
The most common question is simple: is my number normal? The honest answer is that estradiol has no single normal value the way something like sodium does. What counts as normal depends entirely on your sex, your age, and, for menstruating women, the exact day of the cycle the blood was drawn. A value that is perfectly expected in the middle of a cycle would look strikingly high in the days right after a period. This is why comparing your result to a friend’s, or to a generic chart, so often leads people astray. The context printed next to the number matters as much as the number itself.
People also ask whether a low estradiol means menopause. Not on its own. A low estradiol can reflect the natural early part of the cycle, hormonal birth control that suppresses ovarian output, low body weight or intense training, or a signal problem higher up in the brain. Menopause is one explanation among several, and clinicians tell them apart by reading estradiol together with FSH rather than by the estradiol figure alone.
A third recurring question is whether birth control or hormone therapy will skew the result. It usually will, and in a predictable direction. Combined hormonal contraceptives suppress the body’s own estradiol production, so a low reading on the pill is expected rather than alarming. Estrogen therapy raises it. Because of this, it is worth telling whoever orders the test exactly what you are taking, since the same number carries a completely different meaning depending on your current medications.
Timing an estradiol test so the number means something
For a menstruating woman, when the blood is drawn can change the interpretation more than almost anything else. Estradiol rises steadily through the first half of the cycle, peaks around ovulation, dips, and rises again in the second half. A result only makes sense when it is matched to the cycle day it was collected on. If your clinician is checking ovarian reserve or investigating fertility, they will often ask for the draw early in the cycle, around days two to four, when the baseline is meant to be low and a high reading carries specific meaning. Guessing at the day, or drawing whenever is convenient, can turn a useful test into an uninterpretable one.
Beyond cycle timing, a few practical steps keep the result clean. Note any hormonal medication, including the pill, patch, or hormone therapy, and mention recent use of biotin supplements, which can interfere with some hormone immunoassays and skew the reading. If you are tracking estradiol across several tests, such as during hormone therapy, try to draw at a consistent point relative to your dose and, where possible, use the same lab each time, since methods differ and very low levels in particular are read more reliably on some instruments than others.
None of this requires memorizing numbers. It comes down to a habit: pair every estradiol result with the cycle day, the medications you are on, and the lab that ran it, then read the value inside that frame. A result stripped of its context is easy to misread in either direction, while the same number, properly labeled, often answers the question you were testing for in the first place.
Turn what you just learned about estradiol into action.
Superpower lets you test estradiol and 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
Do I need to fast before an estradiol blood test?
No. Estradiol testing does not usually require fasting. The bigger factor is timing: in menstruating women, the draw is often scheduled to a specific cycle day. Follow your clinician’s instructions, since some hormone panels drawn at the same time may have their own prep rules.
What day of my cycle should estradiol be tested?
It depends on the goal. A baseline is often drawn on day 2 or 3 of the cycle, while ovulation tracking targets mid-cycle. Mayo Clinic Laboratories shows estradiol peaking near ovulation, so the cycle day must be recorded for the result to be meaningful.
Is estradiol the same as estrogen?
Not exactly. Estrogen is a group of hormones, and estradiol (E2) is the strongest and most common form during the reproductive years. The other main types are estrone (E1) and estriol (E3). When people say “estrogen test,” they usually mean estradiol, per Cleveland Clinic.
Can men have their estradiol tested?
Yes. Men make small amounts of estradiol, with a normal range of about 10 to 50 pg/mL per MedlinePlus. Testing is used to investigate breast tissue growth, low libido, or fertility issues, often alongside testosterone to assess the balance between the two hormones.
What estradiol level confirms menopause?
No single number confirms menopause on its own. A low estradiol (often under 30 pg/mL) combined with a high FSH supports the diagnosis, especially after 12 months without a period. Your clinician reads these together with your symptoms rather than relying on estradiol alone.
Sources
- MedlinePlus, Estradiol blood test (Medical Encyclopedia)
- MedlinePlus, Estrogen Levels Test
- Cleveland Clinic, Estrogen: Hormone, Function, Levels and Imbalances
- Mayo Clinic Laboratories, Estradiol, Serum (test EEST)
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Related: compare at-home thyroid hormone tests.
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


