
Not sure if your B12 is actually in range? Test it alongside 100+ other biomarkers from home. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
- A vitamin B12 blood test measures the amount of cobalamin (vitamin B12) circulating in your serum, usually reported in picograms per milliliter (pg/mL), to check for deficiency or excess.
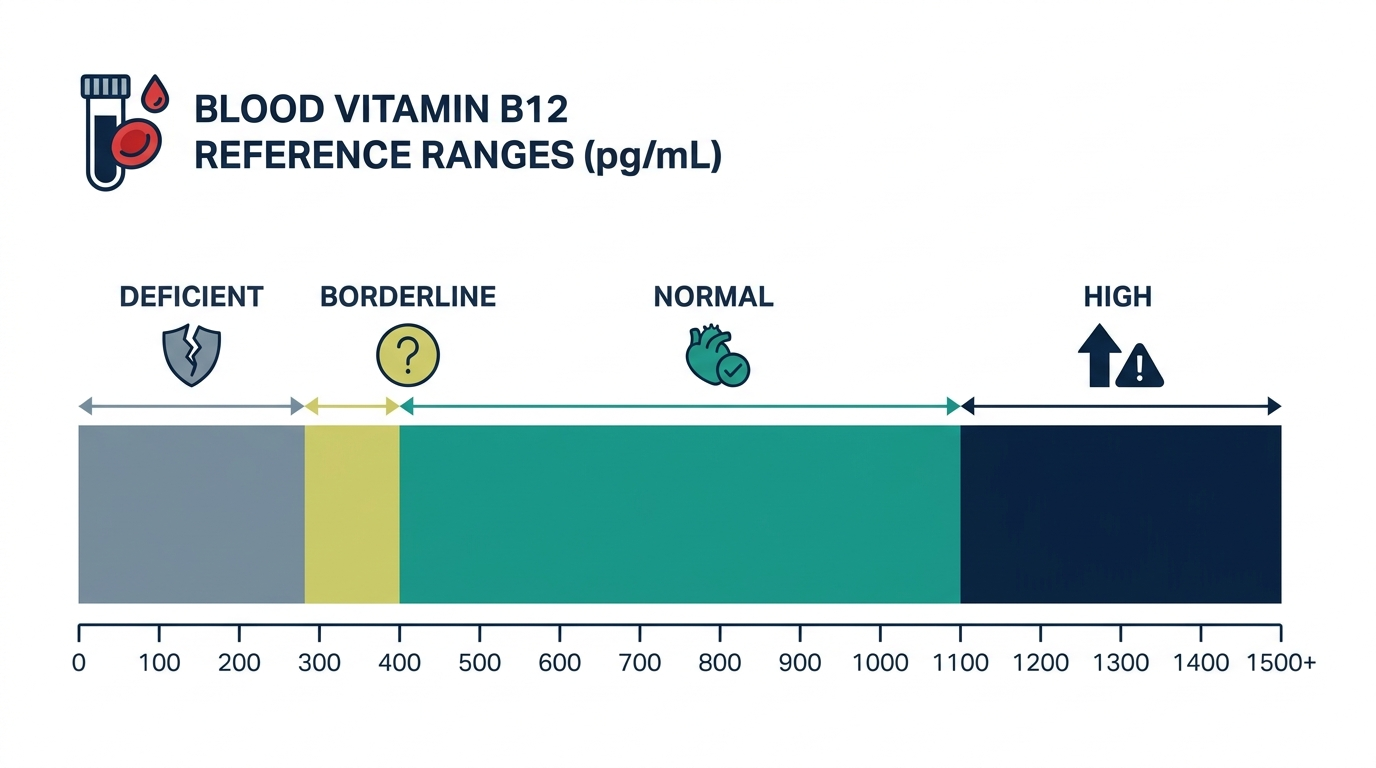
- A typical normal serum vitamin B12 range is roughly 200 to 900 pg/mL, with results below about 200 pg/mL pointing to deficiency and 200 to 300 pg/mL considered a borderline gray zone (MedlinePlus).
- Because a borderline B12 level can be misleading, clinicians often confirm a true deficiency by measuring methylmalonic acid (MMA), which rises when B12 is genuinely low (StatPearls, NCBI).
What is vitamin B12 in a blood test?
In a blood test, vitamin B12 is a measurement of how much cobalamin is circulating in your serum, a vitamin your body needs to make red blood cells, build DNA, and keep nerves healthy. A common normal range runs from about 200 to 900 pg/mL, though MedlinePlus lists a typical normal window of 299 to 1054 pg/mL (219 to 773 pmol/L), and ranges vary by lab. The test is also called a serum cobalamin or serum B12 test.
Your body cannot make B12 on its own. You get it from animal foods such as meat, fish, eggs, and dairy, or from supplements and fortified foods. Because the liver can store several years of B12, a deficiency often builds slowly and may not show symptoms early. The standard test measures total B12, which includes both the active fraction your cells can use and an inactive bound fraction.

Why is vitamin B12 measured?
Vitamin B12 is measured to find or rule out a deficiency that can cause anemia and nerve damage, and it is one of the most common reasons for ordering this test. According to the Cleveland Clinic, untreated B12 deficiency can lead to megaloblastic anemia and neurological problems that may become permanent if missed for too long.
Clinicians commonly order a B12 test when someone has:
- Unexplained anemia: especially large-cell (macrocytic) anemia seen on a complete blood count.
- Nerve symptoms: numbness, tingling, or pins and needles in the hands and feet, plus balance problems.
- Fatigue and cognitive changes: persistent tiredness, brain fog, memory trouble, or mood changes.
- Higher risk profiles: older adults, vegans and vegetarians, people after weight-loss or stomach surgery, and those on long-term metformin or acid-reducing drugs.
Testing is also used to monitor people already being treated for deficiency, to confirm that injections or supplements are working.
What does a high vitamin b12 mean?
A high vitamin B12 result means your serum level sits above the normal range, often above roughly 900 to 1054 pg/mL depending on the lab, and it is far less common than a low result. MedlinePlus notes that excess B12 is usually removed in the urine, so a genuinely elevated level can sometimes signal that the body is retaining it because of an underlying condition.
Common explanations for a high B12 include recent B12 injections, oral supplements, or multivitamins, which are the most frequent and harmless causes. Less often, a high level can reflect liver disease, kidney disease, or certain blood and bone marrow disorders. Because of this, an unexpectedly high result usually prompts a clinician to review your supplement use first and then consider liver function tests or further workup if no supplement explains it. A single high number is rarely diagnostic on its own.
What does a low vitamin b12 mean?
A low vitamin B12 result means your serum level falls below the normal range, and a value under about 200 pg/mL is widely treated as deficient (MedlinePlus). Levels between 200 and 300 pg/mL sit in a borderline zone where deficiency is possible but not certain, which is why a second confirmatory test is often used.
Low B12 most often comes from absorption problems rather than diet alone. Leading causes include:
- Pernicious anemia: an autoimmune condition where the stomach stops making intrinsic factor, the protein needed to absorb B12 (MedlinePlus).
- Gut and surgical causes: Crohn disease, celiac disease, or stomach and intestinal surgery.
- Medications: long-term metformin and proton pump inhibitors that reduce stomach acid.
- Low intake: strict vegan diets without supplementation.
Symptoms of low B12 can include fatigue, weakness, tingling in the limbs, and loss of balance.

How is vitamin b12 interpreted with other markers?
Vitamin B12 is interpreted alongside other markers because the total B12 number alone can miss or overstate a true deficiency, especially in the 200 to 300 pg/mL borderline range. The most useful add-on is methylmalonic acid (MMA), which accumulates when B12 is genuinely lacking, so a high MMA confirms a real deficiency even when serum B12 looks only mildly low (StatPearls, NCBI).
Two other markers add context:
- Homocysteine: rises in B12 deficiency, but it also climbs with folate deficiency, so it is less specific than MMA (NCBI).
- Complete blood count (CBC): large red blood cells (high MCV) often accompany B12 deficiency and point clinicians toward testing.
Folate is frequently checked at the same time because B12 and folate deficiencies cause a similar anemia and can mask each other. Reading these together gives a far more reliable picture than any single value.
The insider nuance: a normal B12 number can still be a false reassurance
One detail many people miss is that a serum B12 in the normal range does not always rule out deficiency, because the standard test measures total B12, not the active fraction your cells can actually use. Up to 80 percent of circulating B12 is bound to a protein that does not deliver it to tissues, so a borderline-normal result of, say, 250 pg/mL can still hide a functional shortfall.
This is exactly why MMA and homocysteine matter. When symptoms strongly suggest deficiency but the B12 number looks acceptable, an elevated MMA can reveal the problem the basic test hides (StatPearls). Some labs also offer an active-B12 (holotranscobalamin) test that measures only the usable portion. The practical takeaway is simple: interpret B12 with your symptoms and confirmatory markers, not from one number in isolation.
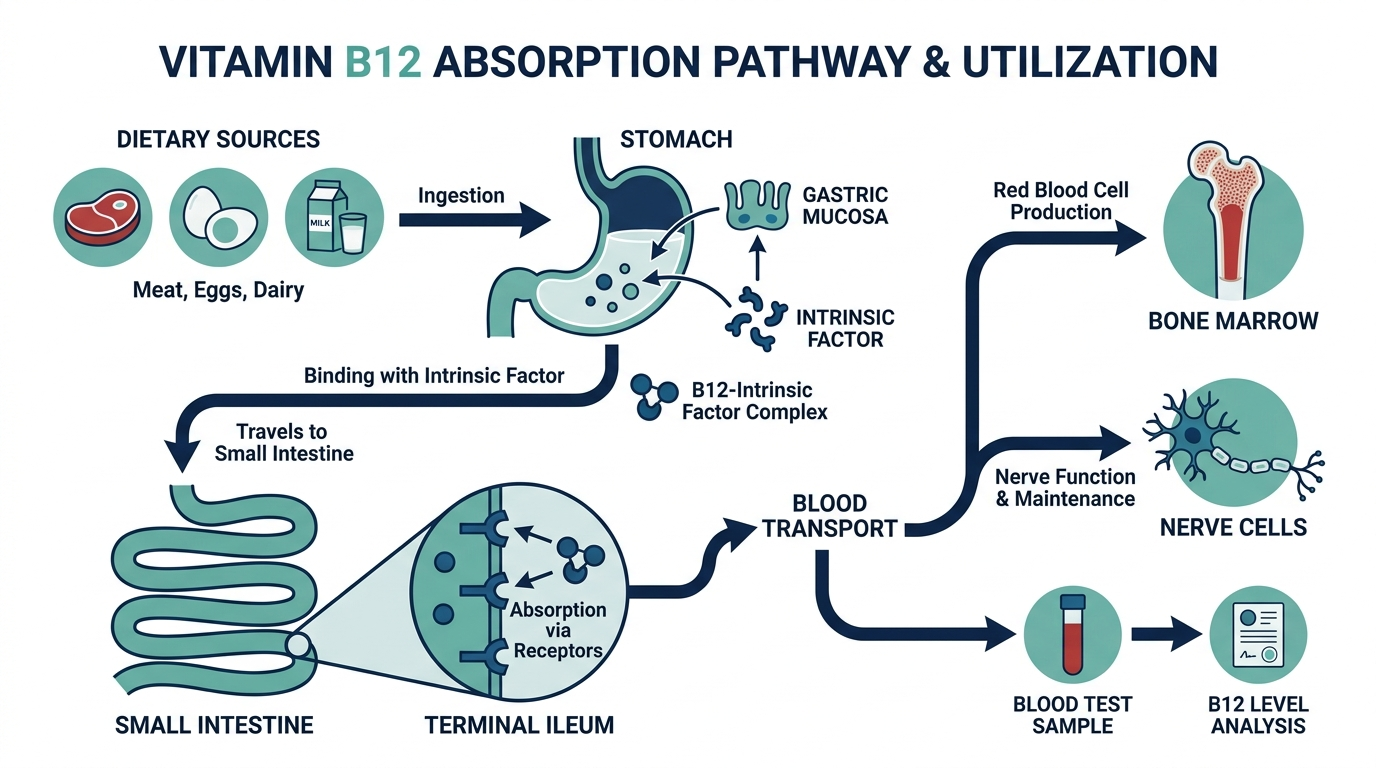
Why B12 absorption is so easy to break
B12 has one of the most elaborate absorption pathways of any nutrient, and that complexity is exactly why deficiency is usually about absorption rather than diet. When you eat B12 bound to animal protein, stomach acid and enzymes first release it. It then binds a carrier protein, and in the stomach a specialized protein called intrinsic factor, made by cells in the stomach lining, latches onto it. That intrinsic factor complex is what allows B12 to be absorbed at the very end of the small intestine, in the terminal ileum.
Break any link in that chain and B12 falls, even with plenty in the diet. Low stomach acid from aging or acid-reducing drugs impairs the first release step. Autoimmune destruction of the intrinsic-factor-making cells causes pernicious anemia. Disease or surgery affecting the terminal ileum removes the final absorption site. Understanding this chain is why a low B12 sends clinicians looking for an absorption cause rather than simply telling you to eat more meat.

How the test is performed and what can distort the number
The vitamin B12 test uses a routine venous blood sample, often drawn alongside a complete blood count and folate. It usually needs no fasting on its own. The catch is that the standard assay can be nudged in either direction by a few common factors, which is why a single number is read with care.
- Recent supplements or injections. Any B12 supplement, multivitamin, or injection in the days or weeks before the draw can raise your serum level and mask an absorption problem. This is the single most common reason for a misleadingly normal or high result.
- High-dose biotin. Biotin supplements, popular for hair and nails, can interfere with certain immunoassays and skew results. If you take biotin, tell the lab, as some recommend pausing it before testing.
- Pregnancy and oral contraceptives. These can lower total B12 without necessarily indicating a true tissue deficiency, one more reason confirmatory markers matter.
- Assay limitations in specific conditions. In some autoimmune settings, antibodies can interfere with the measurement and produce a falsely normal reading despite real deficiency.
The practical rule: report every supplement you take, and treat a borderline value as a starting point for confirmatory testing rather than a final answer.
Why symptoms can appear before, or after, the number moves
B12 deficiency is unusual because the timeline of symptoms and lab values does not always line up. The liver stores several years of B12, so a new absorption problem can take a long time to show up as a low number. Meanwhile, nerve symptoms can begin while the serum value still looks borderline, because tissues can run short even when the blood pool looks adequate.
The symptoms fall into a few clusters worth recognizing:
- Blood-related. Fatigue, weakness, pale or slightly yellow skin, and shortness of breath from megaloblastic anemia, where red cells grow large and inefficient.
- Neurological. Numbness and tingling in the hands and feet, balance problems, and an unsteady gait. These reflect damage to the protective covering of nerves and are the symptoms most likely to become permanent if the deficiency is missed for too long.
- Cognitive and mood. Brain fog, memory trouble, irritability, or low mood, which can be mistaken for other conditions.
- Mouth and tongue. A sore, smooth, or inflamed tongue and mouth ulcers in some people.
The reason clinicians take neurological symptoms seriously even with a borderline number is that nerve damage from prolonged deficiency can be irreversible. That risk is the whole argument for confirming with methylmalonic acid rather than waiting to see if the level drops further.
How much B12 you need and where it comes from
For most adults, the recommended dietary allowance is about 2.4 micrograms per day, rising to roughly 2.6 micrograms in pregnancy and 2.8 micrograms while breastfeeding, per the National Institutes of Health Office of Dietary Supplements. These are small amounts, which is why deficiency is usually about absorption rather than intake in people who eat animal foods.
Food sources are almost entirely animal-derived, which is why plant-based eaters need a reliable supplemented or fortified source:
- Richest sources: clams, liver, and other organ meats carry very high amounts.
- Everyday sources: fish such as salmon and tuna, beef, poultry, eggs, and dairy.
- For plant-based diets: fortified nutritional yeast, fortified plant milks and cereals, and B12 supplements, since plants do not reliably provide B12.
Older adults deserve a special note: an estimated portion of people over 50 develop atrophic gastritis with reduced stomach acid, which impairs absorption of B12 from food even when intake is adequate. For this reason, guidance suggests older adults get much of their B12 from supplements or fortified foods, whose B12 is easier to absorb.

How a confirmed deficiency is treated
Treatment depends on the cause and severity, and understanding the logic helps you follow your clinician’s plan.
- Absorption problems like pernicious anemia. When the gut cannot absorb B12 from food, treatment traditionally uses intramuscular B12 injections, which bypass the gut entirely. High-dose oral B12 can also work for some people because a small fraction is absorbed by a passive route that does not need intrinsic factor, but the choice is individualized.
- Dietary deficiency. In someone whose only problem is low intake, such as an unsupplemented vegan diet, oral supplementation and dietary changes usually suffice.
- Reversing medication effects. If long-term metformin or an acid-reducing drug is driving the deficiency, your clinician weighs supplementation against adjusting the medication, never stopping a prescribed drug on your own.
- Monitoring the response. Blood counts typically improve within weeks, while neurological recovery is slower and depends on how long the deficiency lasted. A recheck confirms the plan is working.
A key point: neurological symptoms can improve with treatment but may not fully reverse if the deficiency was prolonged, which is exactly why early detection matters more than for many other nutrients.
Reading B12 in context: worked scenarios
The interpretation of a B12 result hinges on the company it keeps. A few examples:
- B12 at 180 pg/mL with tingling feet and large red cells. A clear deficiency picture. This warrants prompt treatment and a search for the cause, such as pernicious anemia.
- B12 at 250 pg/mL with clear nerve symptoms. A borderline number that does not match the symptoms. An elevated methylmalonic acid can confirm a functional deficiency the total B12 hides.
- B12 at 1,100 pg/mL in someone taking a daily multivitamin. Almost always explained by the supplement. The clinician reviews supplement use before any further workup.
- B12 high with no supplements. Less common and worth a second look, since an unexplained high level can occasionally reflect liver, kidney, or blood disorders.
- Normal B12 but high homocysteine and normal MMA. Points more toward folate than B12, showing why folate is often checked at the same time.
Who should consider getting tested
B12 is not a universal screen for every healthy adult, but several groups carry enough risk that testing is often worthwhile, especially when symptoms are present:
- Older adults. Reduced stomach acid with age lowers absorption, making this one of the highest-yield groups to test.
- Vegans and strict vegetarians. Without supplementation or fortified foods, intake can fall short over time, and stores eventually deplete.
- People on long-term metformin or acid-reducing drugs. Both are linked to lower B12 over years of use, so periodic checks are reasonable.
- Anyone after stomach or intestinal surgery. Bariatric surgery and procedures affecting the stomach or terminal ileum impair the absorption pathway.
- People with unexplained anemia or neurological symptoms. Fatigue with large red cells, or tingling and balance problems, are classic prompts to test.
If you fall into one of these groups, ask your clinician whether a B12 check, ideally with a plan to confirm borderline results, makes sense for you. Catching a deficiency before nerve symptoms set in is the whole point.
Common misunderstandings about the B12 test
- “A normal B12 means I am fine.” Not always. The standard test measures total B12, much of which is inactive. A borderline-normal value with symptoms can still hide a functional deficiency detectable by MMA or active B12.
- “High B12 is dangerous, so I should stop supplements immediately.” A high level from supplements is usually harmless because excess is cleared in urine. The concern is an unexplained high level without supplements, not the supplement-driven one.
- “I eat meat, so I cannot be deficient.” Most deficiency comes from poor absorption, not low intake. Pernicious anemia, gut disease, surgery, and certain medications can cause deficiency in people who eat plenty of B12.
- “B12 and folate are interchangeable.” They cause similar anemia and can mask each other, but they are different vitamins with different treatments. Treating with folate alone can improve the blood count while nerve damage from B12 deficiency quietly worsens, which is why both are measured.
Why B12 and folate must be read as a pair
B12 rarely travels alone on a workup, and the reason is a genuine trap in how deficiency is treated. B12 and folate work as partners in the same pathway that builds DNA and matures red blood cells, so a shortage of either one produces a very similar picture on a complete blood count: large, immature red cells known as macrocytic anemia. Because the blood picture looks alike, folate is usually measured alongside B12 to tell the two apart before anyone starts treatment.
The trap is specific and well known to clinicians. Giving folate to someone who is actually B12 deficient can correct the anemia, so the blood count improves and everyone feels reassured, while the underlying B12 deficiency keeps quietly damaging the nervous system. The blood problem gets masked, but the nerve problem does not, and nerve damage from prolonged B12 deficiency can become permanent. This is exactly why the order of testing and treatment matters, and why a clinician confirms B12 status before treating a folate-pattern anemia rather than simply reaching for the vitamin that is easiest to replace.
There is a practical lesson for anyone reading their own results. If your report shows a large-cell anemia, look for both B12 and folate, not just one. If only folate was checked and it was low, that does not clear you of a B12 problem, and it is a fair question to raise with your clinician. The same caution applies to high-dose supplements bought over the counter. A general multivitamin or a folic acid supplement can nudge blood counts toward normal without addressing a B12 gap, which is one more reason a genuine deficiency is confirmed with the right tests before being treated, rather than guessed at from a single number.
Don’t just read about vitamin b12, track it.
A single result is a snapshot. Superpower re-tests vitamin b12 and 100+ markers over time so you can watch them move as you change sleep, food, and training.
Frequently asked questions
Do I need to fast before a vitamin B12 blood test?
Usually no. A standard serum B12 test does not require fasting. However, if your clinician orders it as part of a panel with tests that do require fasting, such as glucose or lipids, you may be asked to fast. Always follow the specific instructions your lab or provider gives you.
What is a dangerously low B12 level?
A serum B12 below about 200 pg/mL is generally considered deficient, and very low levels well under this can cause anemia and nerve damage (MedlinePlus). Severity depends on symptoms and how long the deficiency has lasted, not the number alone, so any low result should be discussed with a clinician promptly.
Can supplements affect my B12 test result?
Yes. Recent B12 supplements, multivitamins, or injections can raise your serum B12 and may produce a normal or high result even if you have an absorption problem. Tell your clinician about any supplements before testing, since this is one of the most common reasons for an unexpectedly high B12.
What is the difference between total B12 and active B12?
Total B12 measures all cobalamin in your serum, including a large inactive fraction. Active B12, also called holotranscobalamin, measures only the portion your cells can use. Active B12 can sometimes detect deficiency earlier, but total B12 remains the standard first test in most labs.
How often should B12 be checked?
There is no single schedule for everyone. People being treated for deficiency may be rechecked within a few months to confirm improvement. Higher-risk groups, such as older adults, vegans, and those on long-term metformin or acid reducers, may be tested periodically. Your clinician sets the timing based on your situation.
Sources
- MedlinePlus, Vitamin B12 level
- Cleveland Clinic, Vitamin B12 Deficiency
- StatPearls (NCBI Bookshelf), Vitamin B12 Deficiency
- NIH Office of Dietary Supplements, Vitamin B12 Fact Sheet for Health Professionals
- Mayo Clinic Laboratories, Vitamin B12 Assay, Serum
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


