
Low B12 often comes from absorption issues you wouldn’t notice otherwise, so where does your level fall? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
- A low vitamin B12 blood test usually means your serum level falls below about 200 to 300 pg/mL, with under 200 pg/mL flagged as a true deficiency by MedlinePlus.
- Low B12 most often comes from poor absorption (pernicious anemia, certain medications, gut surgery) or a low-intake diet, not just from eating too little meat.
- Untreated low B12 can cause anemia and permanent nerve damage, so a confirmed low result should be reviewed by a clinician rather than self-treated with random supplements.
Seeing “low” next to your vitamin B12 result is unsettling, especially when the symptoms are vague. The good news: B12 deficiency is one of the most treatable lab findings you can get. The catch is that the number alone does not tell the whole story, and a borderline result is easy to misread. Here is what a low B12 actually means, what likely caused it, and what to do next.
What does a low vitamin B12 result mean, and what is the cutoff?
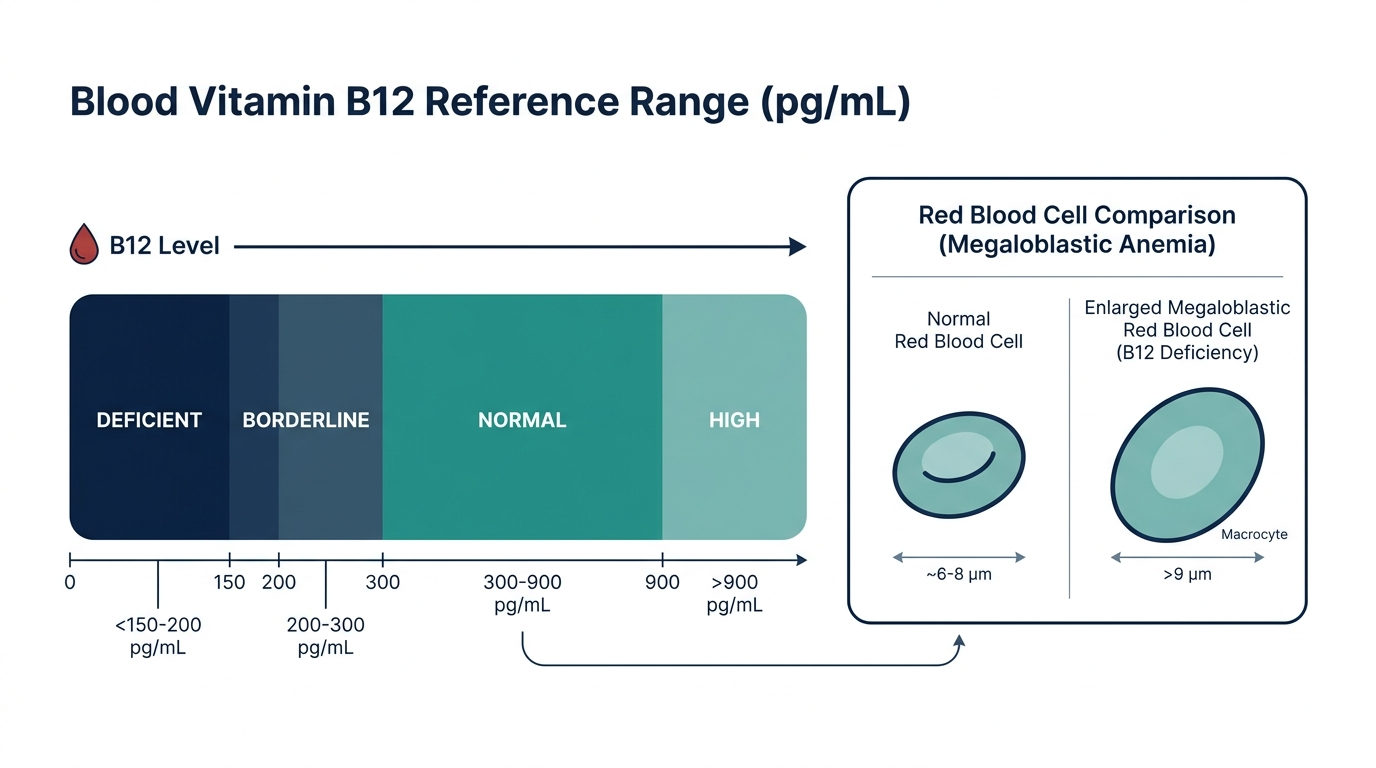
A low vitamin B12 result means your blood carries less of this vitamin than your nerves and red blood cells need to work normally. According to MedlinePlus, the typical normal range is 299 to 1054 pg/mL (219 to 773 pmol/L), and a value under 200 pg/mL indicates a vitamin B12 deficiency. Results between roughly 200 and 300 pg/mL are considered borderline and often need repeat or confirmatory testing.
The reference range varies slightly between labs, so always read your result against the range printed on your own report. One important nuance: serum B12 measures total circulating B12, not how much your cells can actually use. That is why a borderline number does not automatically mean you are fine, and why doctors sometimes order follow-up markers even when your B12 looks “low-normal.”

What causes low vitamin B12?
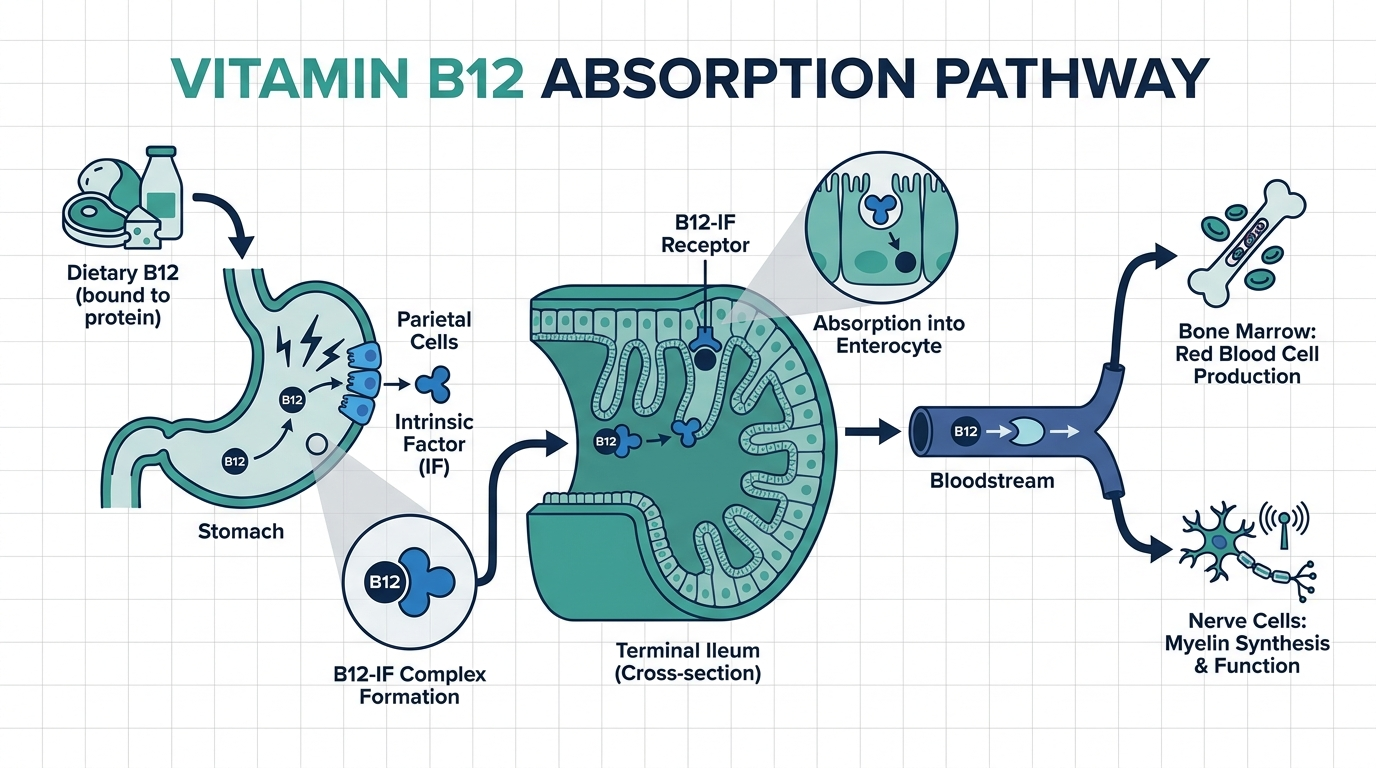
Most low B12 results come from poor absorption rather than poor diet. Per StatPearls (NCBI) and the Cleveland Clinic, the leading cause in older adults is pernicious anemia, an autoimmune condition where the body cannot absorb B12 because it lacks intrinsic factor. Common causes include:
- Pernicious anemia: autoimmune loss of intrinsic factor, especially common after age 60 (StatPearls).
- Diet: low intake in strict vegans and vegetarians, since B12 comes mainly from animal foods (NIH Office of Dietary Supplements).
- Medications: long-term metformin and acid-reducing drugs (proton pump inhibitors, H2 blockers) lower absorption (NIH ODS).
- Gut conditions and surgery: Crohn disease, celiac disease, and stomach or bowel surgery reduce uptake (Cleveland Clinic).
- Age: stomach acid drops with age, which limits how much B12 you can pull from food.
Heavy alcohol use and certain rare genetic conditions can also play a role. Pinning down the cause matters because the fix differs: a vegan needs different treatment than someone with pernicious anemia.
What are the symptoms of low vitamin B12, or is it silent?
Low B12 can be silent for months or years before symptoms appear, then show up as a mix of blood and nerve problems. StatPearls lists fatigue, pale skin, glossitis (a smooth, sore tongue), and pins-and-needles tingling in the hands and feet as classic signs, alongside memory trouble, irritability, and low mood.
The tricky part is that neurological symptoms can begin before anemia shows up on a blood count, and some people feel almost nothing until the deficiency is advanced. Watch for these patterns:
- Hematologic: tiredness, weakness, shortness of breath, pale or slightly yellow skin.
- Neurological: numbness or tingling, balance problems, trouble concentrating, “brain fog.”
- Mood and cognition: depression, irritability, and in severe cases confusion or psychosis (StatPearls).
Because these overlap with so many other conditions, the symptoms alone rarely confirm B12 deficiency. The blood test plus your story is what points the way.
When is low vitamin B12 dangerous?
Low B12 becomes dangerous when it goes untreated long enough to damage nerves or crash your blood counts. The NHLBI notes that B12-deficiency anemia can leave you severely fatigued and short of breath, while StatPearls warns that prolonged deficiency can cause nerve damage that may become permanent if not corrected in time.
In rare, severe cases, B12 deficiency drives down all three blood cell lines at once (pancytopenia), which can be life-threatening but is usually reversible with treatment, according to case reports indexed in PMC (NIH). Red flags that warrant prompt medical attention include worsening numbness or balance loss, marked breathlessness, chest pain, fainting, or confusion. These suggest the deficiency has moved past the “borderline number” stage into territory that needs treatment now, not at your next routine checkup.

What should you do next, and when should you see a doctor?
If your B12 is low, the first step is to confirm it and find the cause, not to start mega-dosing supplements on your own. MedlinePlus and StatPearls note that a borderline or low result is often confirmed by checking methylmalonic acid (MMA); a high MMA points to a true B12 deficiency at the cellular level.
A practical path forward:
- Confirm: ask whether you need a repeat B12, plus MMA and homocysteine, to verify a true deficiency.
- Find the cause: review your diet, medications (metformin, acid blockers), and any gut history with your clinician.
- Treat correctly: pernicious anemia and absorption problems often need B12 injections, while diet-related cases may respond to oral supplements (StatPearls).
- Recheck: follow up to confirm levels and symptoms are improving.
See a doctor promptly if you have neurological symptoms (numbness, tingling, balance issues) or significant fatigue, since these can signal the deficiency is already affecting your nerves.
The insider nuance: why a “normal” B12 can still be too low for you
Here is what experienced clinicians watch for: a serum B12 in the low-normal band (roughly 200 to 350 pg/mL) can still mask a real deficiency, because the test counts total B12, including the portion bound to proteins your cells cannot use. This is why MMA and homocysteine matter; both rise when B12 is functionally low even if the headline number looks acceptable.
If you have classic symptoms but a “normal” B12, do not let the single number end the conversation. Newer markers such as holotranscobalamin (active B12) and the confirmatory MMA test exist precisely for this gray zone. The number on the page is a starting point for a clinical decision, not the final verdict by itself.
The confirmatory tests: MMA, homocysteine, and active B12
Because serum B12 measures total circulating vitamin rather than what your cells can actually use, clinicians rely on a small set of follow-up tests to confirm a true deficiency, especially in the borderline zone. Understanding these turns a confusing low-normal result into a clear answer.
- Methylmalonic acid (MMA): this is the most useful confirmatory test. B12 is needed to process MMA, so when B12 is functionally low, MMA builds up. A high MMA points to a true deficiency at the cellular level, even when serum B12 looks acceptable. Crucially, MMA rises in B12 deficiency but stays normal in folate deficiency, which is what lets it tell the two apart (MMA and homocysteine as B12 indicators, PMC).
- Homocysteine: this rises when either B12 or folate is low, so on its own it cannot distinguish the two. Paired with MMA, though, it sharpens the picture. High homocysteine with high MMA suggests B12; high homocysteine with normal MMA suggests folate.
- Holotranscobalamin (active B12): this measures only the fraction of B12 bound to transcobalamin, the portion your cells can take up. It targets the same gray zone MMA does and is offered by some labs as an earlier signal of functional deficiency.
The practical rule is simple. If you have symptoms but a borderline or low-normal B12, these tests are how your clinician decides whether the number is a false reassurance. The headline B12 value is a starting point, not the verdict.

The folate trap: why B12 and folate must be read together
One of the most important and least understood interactions in this whole area is between vitamin B12 and folate. Both are needed to build healthy red blood cells, and a deficiency of either produces the same tell-tale change on a CBC: large, immature red cells, seen as a mean corpuscular volume (MCV) above about 100, a pattern called macrocytic anemia.
Here is the trap. If someone with an undiagnosed B12 deficiency takes folic acid, whether as a supplement or from heavily fortified foods, the folate can correct the anemia and normalize the MCV. That sounds good, but it is dangerous, because folate does not fix the neurological damage that B12 deficiency causes. The blood picture looks better while the nerves keep deteriorating silently in the background.
This is why a low B12 should never be treated by simply taking a B-complex vitamin and moving on. It is also why clinicians order B12 and folate together and lean on MMA to confirm which one is truly deficient. If your anemia resolves but your numbness or balance problems persist, the folate trap is exactly the scenario to raise with your clinician.
How much B12 you need and where it comes from
The recommended dietary allowance of vitamin B12 for most adults is about 2.4 micrograms per day, rising modestly in pregnancy and breastfeeding (NIH Office of Dietary Supplements). That is a small amount, but the catch is that B12 comes almost entirely from animal foods, which is why diet and absorption both matter.
Rich natural sources include:
- Shellfish: clams and oysters are among the most concentrated sources.
- Organ meats: beef liver is exceptionally high.
- Fish: salmon, trout, and tuna.
- Meat and poultry: beef, and to a lesser extent chicken.
- Dairy and eggs: milk, yogurt, cheese, and egg yolks.
Because plant foods contain essentially no B12 unless fortified, strict vegans and many vegetarians need a reliable source such as fortified breakfast cereals, fortified plant milks, nutritional yeast, or a supplement. This is also why diet-related deficiency is one of the more straightforward cases to correct: the fix is adding a dependable source. Absorption-related deficiency is different, because no amount of dietary B12 helps if your gut cannot take it up, which is the reason the cause matters as much as the number.
How low B12 is treated: injections versus pills
Treatment depends entirely on why you are low, which is the single most important reason to identify the cause before reaching for supplements.
Diet-related deficiency
If you simply are not taking in enough B12 and your gut absorbs normally, oral supplements or a richer diet usually restore your level over weeks. This is the simplest scenario.
Absorption-related deficiency
If the problem is that your body cannot absorb B12, as in pernicious anemia, gut surgery, or damage from inflammatory bowel disease, oral pills at ordinary doses often are not enough because the absorption pathway itself is broken. In these cases treatment classically uses B12 injections, which bypass the gut entirely. A common approach starts with more frequent injections to refill stores, then tapers to a maintenance schedule. High-dose oral B12 works for some absorption problems through a passive uptake pathway, but this is a decision for your clinician based on the cause and your response.
Medication-related deficiency
When long-term metformin or acid-reducing drugs are the driver, your clinician weighs adjusting the medication against adding B12, since stopping a needed drug is not always the right trade.
The recurring theme is that a low B12 is highly treatable, but the correct treatment is tied to the cause. Self-treating with random supplements can normalize the number while missing an underlying absorption problem that needs a different fix entirely.

Recovery timeline: what improves and what may not
Once treatment starts, different symptoms recover on different schedules, and setting the right expectation prevents both impatience and false alarm.
- Blood counts: the anemia typically begins improving within days to weeks, and red cell size (MCV) normalizes over a couple of months as new, healthy cells replace the old.
- Energy and general symptoms: fatigue and weakness often lift within weeks as the anemia corrects.
- Neurological symptoms: numbness, tingling, and balance problems recover more slowly, over months, and this is the key caveat: nerve damage from long-standing, severe deficiency may not fully reverse if treatment came too late.
That last point is the reason clinicians urge prompt evaluation of neurological symptoms rather than watchful waiting. The window in which nerve damage is fully reversible is finite. A follow-up test after treatment confirms your level has risen, but the more meaningful check is whether your symptoms are resolving on the expected timeline.
Who is most at risk of low B12 and should consider testing
B12 deficiency is far more common in some groups than others. If you belong to one of these, a low result is unsurprising, and testing is worth discussing even if your symptoms are vague.
- Adults over 60: stomach acid production falls with age, which reduces how much B12 you can pull from food. Pernicious anemia also becomes more common with age.
- Strict vegans and long-term vegetarians: because B12 comes almost entirely from animal foods, plant-based eaters without a reliable fortified source or supplement are at clear risk.
- People on long-term metformin: this common diabetes drug reduces B12 absorption over years of use.
- People on acid-reducing drugs: proton pump inhibitors and H2 blockers lower the stomach acid needed to release B12 from food.
- People with gut disease or surgery: Crohn disease, celiac disease, and any surgery affecting the stomach or the last part of the small intestine (the ileum, where B12 is absorbed) all impair uptake.
- Heavy alcohol users: alcohol affects both intake and absorption.
- People with autoimmune conditions: those with other autoimmune diseases have a higher chance of pernicious anemia.
If two or more of these apply to you, particularly age plus a medication like metformin or an acid blocker, a low or low-normal B12 fits the pattern and is usually straightforward to confirm and correct. The presence of a risk factor also helps your clinician interpret a borderline number, because context is what turns an ambiguous value into a decision.
Common misconceptions about low B12
A few persistent myths cause people to either panic or dismiss a low B12 result. Clearing them up helps you respond correctly.
- “Low B12 just means I need to eat more meat.” Often untrue. In older adults, most deficiency comes from poor absorption, not low intake, and eating more animal food does not fix a broken absorption pathway.
- “A normal B12 rules out deficiency.” Not always. A low-normal serum B12 can still hide a functional deficiency, which is exactly why MMA and homocysteine exist.
- “I can just take a high-dose supplement and skip the doctor.” Risky. Self-treating can normalize the number and even correct anemia while missing an underlying cause, and folic acid in a B-complex can mask B12 deficiency while nerves keep deteriorating.
- “If my energy is back, I am cured.” Not necessarily. Blood symptoms recover faster than nerve symptoms, so feeling more energetic does not confirm your nerves have fully healed.
- “B12 deficiency is harmless because it is common.” Common does not mean benign. Untreated, it can cause anemia and permanent nerve damage, which is why a confirmed low result deserves a real evaluation.
Read your B12 as one piece of a larger picture that includes the cause, the confirmatory markers, and your symptoms over time, and it becomes one of the most fixable findings on your entire lab report.
Turn what you just learned about vitamin b12 into action.
Superpower lets you test vitamin b12 and 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
What B12 level is considered dangerously low?
A serum vitamin B12 under 200 pg/mL is generally classified as a deficiency by MedlinePlus. Levels well below that, especially with anemia or nerve symptoms, are more concerning and warrant prompt treatment. Confirmatory testing with methylmalonic acid helps gauge how true the deficiency is.
Can low B12 be fixed quickly?
Often yes. Diet-related deficiency may improve within weeks of oral supplements, while absorption problems like pernicious anemia usually need B12 injections that start frequently, then taper, per StatPearls. Nerve symptoms can take longer to recover, and very longstanding damage may not fully reverse.
Is low B12 always caused by diet?
No. While strict vegans and vegetarians are at higher risk, most low B12 results in older adults come from poor absorption, such as pernicious anemia, gut disease, surgery, or long-term metformin and acid-reducing medications (NIH, Cleveland Clinic).
What is borderline B12 and should I worry?
A result between roughly 200 and 300 pg/mL is borderline, per MedlinePlus. It does not confirm deficiency but is not clearly normal either. Doctors often repeat the test or add methylmalonic acid and homocysteine to decide whether treatment is needed.
Can low B12 cause permanent damage?
Yes, if untreated. StatPearls warns that prolonged B12 deficiency can cause nerve damage that may become permanent. This is why neurological symptoms like numbness, tingling, or balance problems with a low B12 should be evaluated promptly rather than monitored indefinitely.
Sources
- MedlinePlus, Vitamin B12 level
- Cleveland Clinic, Vitamin B12 Deficiency
- StatPearls (NCBI), Vitamin B12 Deficiency
- NIH Office of Dietary Supplements, Vitamin B12 Fact Sheet
- NHLBI (NIH), Vitamin B12 Deficiency Anemia
- PMC (NIH), Pernicious Anemia and Severe B12 Deficiency Case Report
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


