
Low vitamin D is extremely common, so is your level actually below the 20 ng/mL deficiency line? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
- A low vitamin D blood test usually means your serum 25-hydroxyvitamin D level is below 20 ng/mL (50 nmol/L), the threshold most labs and the NIH use to define deficiency.
- Low vitamin D is extremely common and often silent, but over time it can soften bones (osteomalacia), cause bone pain and muscle weakness, and raise fracture risk, especially in older adults.
- Most low vitamin D results are correctable with sunlight, diet, and supplements, so the next step is to confirm the cause with your clinician and recheck the level after treatment.
If your lab report flags a low vitamin D, you are looking at a single number that measures how much vitamin D is circulating in your blood. The test is called the 25-hydroxyvitamin D test, written as 25(OH)D. This article explains what the number means, why it dropped, what symptoms to watch for, and when low vitamin D becomes something to act on quickly.
What does a low vitamin D result mean, and what is the cutoff?
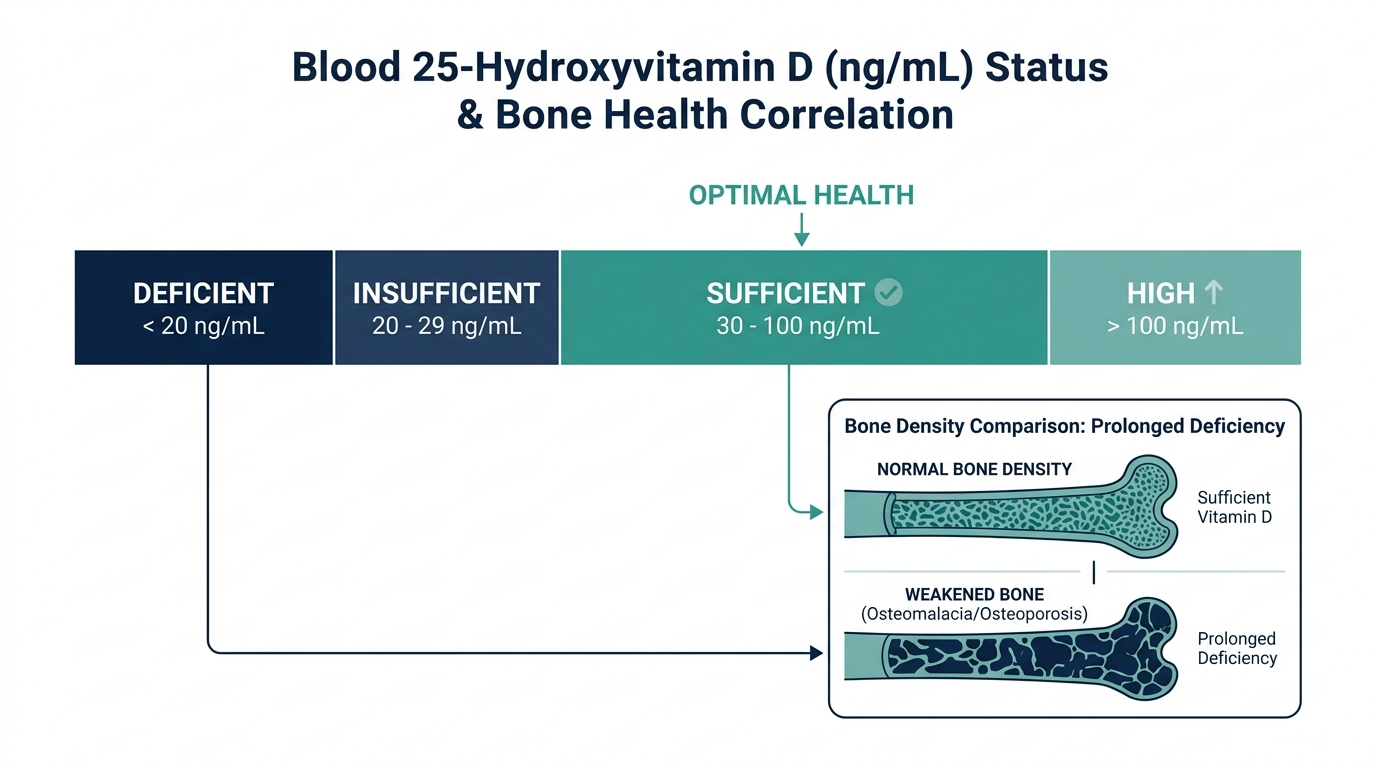
A low vitamin D result means your serum 25-hydroxyvitamin D is below the level your body needs for healthy bones and muscles. The most widely used cutoff for deficiency is below 20 ng/mL (50 nmol/L), per the NIH Office of Dietary Supplements and most US labs. The 25(OH)D reference range typically runs from 20 to 100 ng/mL, so anything under 20 ng/mL falls outside it.
Where it gets confusing is the gray zone. Different expert groups draw the lines differently:
- Below 12 ng/mL: The 2011 Endocrine Society guideline defines this as outright deficiency.
- 12 to 20 ng/mL: Generally considered deficient or at risk by the NIH and National Academies of Sciences (NASEM).
- 20 to 30 ng/mL: Often labeled insufficiency, though in 2024 the Endocrine Society stepped back from a firm 30 ng/mL target for healthy adults.
- 30 ng/mL and above: Considered sufficient by most labs.
So a result of 17 ng/mL is clearly low, while a result of 26 ng/mL sits in the debated middle. Your clinician interprets it alongside your symptoms, age, and bone health, not in isolation.

What causes low vitamin D?
Low vitamin D usually comes from too little sun exposure, too little dietary intake, or a body that cannot absorb or activate it well. The NIH notes vitamin D is hard to get from food alone, and roughly 90% of adults aged 51 to 70 fall short of recommended intake from diet, which is a major reason low readings are so common.
Common drivers include:
- Limited sunlight: Indoor lifestyles, northern latitudes, winter months, and routine sunscreen use all cut the skin’s vitamin D production.
- Darker skin: Higher melanin reduces how much vitamin D the skin makes from the same sun exposure.
- Age: Older skin synthesizes vitamin D less efficiently.
- Malabsorption: Celiac disease, Crohn’s disease, and weight-loss surgery limit fat absorption, and vitamin D is fat-soluble.
- Obesity: Vitamin D gets sequestered in body fat, lowering blood levels.
- Kidney or liver disease: These organs convert vitamin D into its active form, so disease there blunts activation.
What are the symptoms, or is it silent?
Low vitamin D is often completely silent, which is why so many people only find out from a blood test. When symptoms do appear, they are usually vague and easy to blame on something else. The classic signs, per Cleveland Clinic and MedlinePlus, are bone pain, muscle weakness, fatigue, and mood changes.
More specific clues that point toward true deficiency, especially the bone-softening condition osteomalacia, include:
- Bone pain: Often a dull ache in the lower back, hips, pelvis, thighs, or feet.
- Tenderness: Bones may feel sore when pressed, particularly the shins and ribs.
- Muscle weakness: Trouble climbing stairs or rising from a chair, sometimes with a waddling gait.
- Frequent illness or low mood: Reported by many, though less specific to vitamin D alone.
In children, severe long-standing deficiency causes rickets, which deforms growing bones. In adults, the same deficiency produces osteomalacia rather than rickets.
When is low vitamin D dangerous?
Low vitamin D becomes dangerous when it is deep or long-lasting enough to weaken your skeleton. Levels below 25 ng/mL are linked to a higher risk of secondary hyperparathyroidism, lower bone mineral density, and fractures, and the risk climbs as the number falls, especially in older adults.
Watch for these warning situations:
- A very low number (under 12 ng/mL): This signals true deficiency that warrants prompt treatment.
- Bone fractures from minor falls: A possible sign of osteomalacia or osteoporosis.
- Persistent bone pain plus muscle weakness: The combination most associated with symptomatic deficiency.
- Falls in older adults: Weak muscles from low vitamin D raise fall and fracture risk together.
Importantly, low vitamin D itself is not an emergency. The danger is the slow damage to bone and muscle over months to years if it goes uncorrected, not a sudden crisis.

What to do next, and when to see a doctor
The next step after a low vitamin D result is to talk with your clinician about the likely cause and a correction plan, then recheck the level after about 3 months of treatment. Most low readings respond to sunlight, vitamin D rich foods, and supplements, with the dose tailored to how low you started.
Practical actions:
- Confirm the cause: Your clinician may check calcium, parathyroid hormone, or kidney function if the deficiency is severe or unexplained.
- Adjust intake: Fatty fish, fortified milk, eggs, and a vitamin D3 supplement are common fixes; deficiency often needs a higher loading dose first.
- Get sensible sun: Short, regular sun exposure helps, balanced against skin cancer risk.
- Recheck: A repeat 25(OH)D test confirms you have reached a healthy range.
See a doctor promptly if you have ongoing bone pain, muscle weakness, a fracture from a minor fall, or a result under 12 ng/mL. Anyone with a malabsorption condition, kidney or liver disease, or a history of fractures should treat low vitamin D as a priority rather than a footnote.
Insider nuance: not all vitamin D tests are equal
One thing clinicians know that patients rarely hear is that the 25(OH)D test measures storage, not activity, and that lab-to-lab variation is real. The test reports total 25(OH)D, the long-lived storage form, which is why it is the right marker for status. A different test, 1,25-dihydroxyvitamin D, measures the active hormone but is not used to diagnose ordinary deficiency, because it can look normal even when your stores are empty.
Assay differences also matter. Two labs can return slightly different numbers from the same blood draw, so a value of 21 versus 19 ng/mL should not be treated as a hard pass or fail. This is part of why expert groups have softened rigid cutoffs and why your clinician weighs the trend and your symptoms more than a single decimal point.
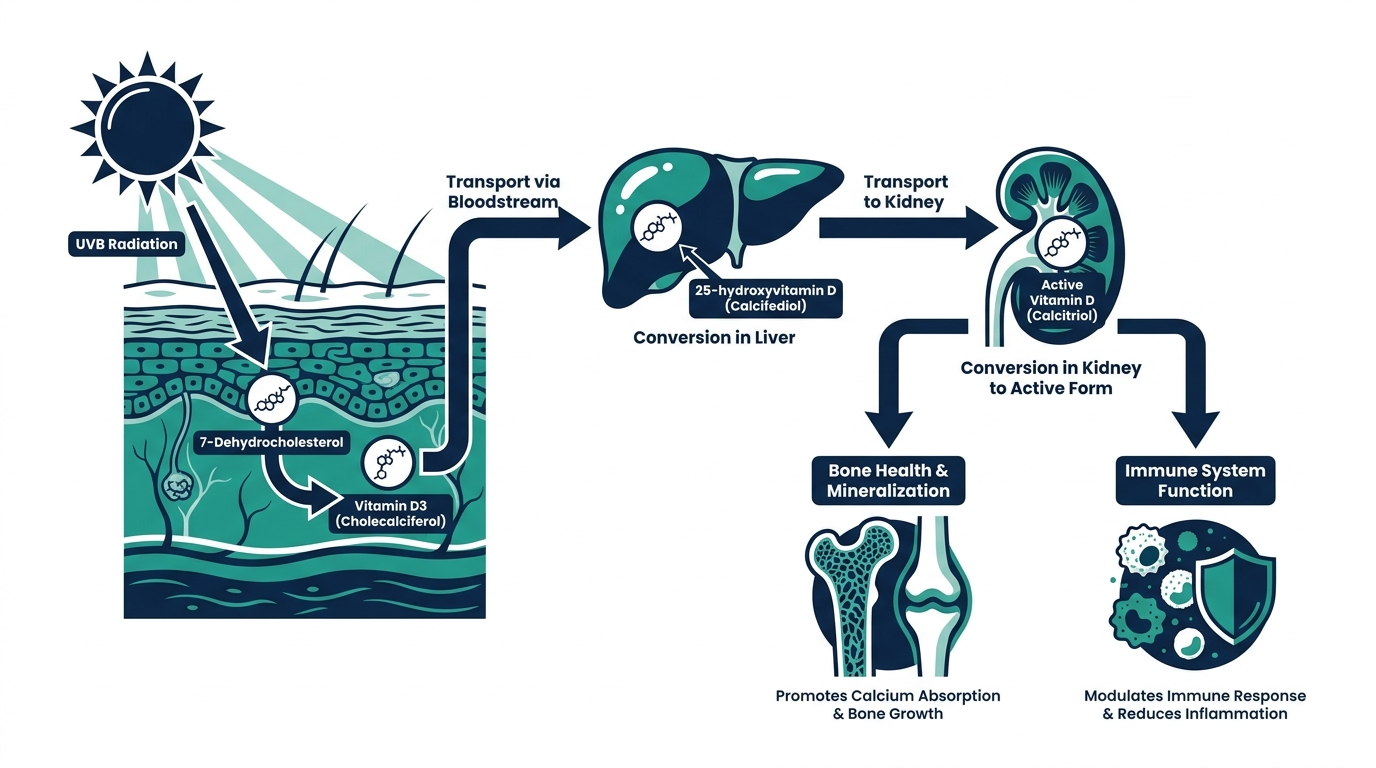
How your body makes and uses vitamin D
Understanding why a number is low is easier once you see the assembly line vitamin D travels. It is not really a vitamin in the classic sense, it behaves more like a hormone your body builds in stages. When ultraviolet B light hits your skin, it converts a cholesterol derivative into vitamin D3. That raw form is inactive. Your liver then adds a hydroxyl group to make 25-hydroxyvitamin D, the storage form your blood test measures. Finally your kidneys convert that into 1,25-dihydroxyvitamin D, the active hormone that tells your gut to absorb calcium and phosphate and helps keep bone remodeling in balance.
This three-step chain explains most low readings. If sunlight is scarce, step one stalls. If the liver is diseased, step two falters. If the kidneys are failing, step three cannot finish, which is why people with advanced kidney disease can have adequate storage levels yet still lack the active hormone. It also explains why the storage form, 25(OH)D, is the right test: it sits in the middle of the chain, changes slowly, and reflects your overall supply rather than a momentary snapshot.
ng/mL versus nmol/L: reading your units correctly
One of the most common sources of needless panic is a units mix-up. Vitamin D results come in two scales depending on the lab and country. In the United States, results are usually reported in nanograms per milliliter (ng/mL). Much of the rest of the world uses nanomoles per liter (nmol/L). The two are not interchangeable at face value, and confusing them can make a healthy level look alarmingly low or vice versa.
The conversion is straightforward: multiply ng/mL by 2.5 to get nmol/L, or divide nmol/L by 2.5 to get ng/mL. So the 20 ng/mL deficiency cutoff equals 50 nmol/L, and 30 ng/mL equals 75 nmol/L. If you ever compare a result from two different labs or a test taken abroad, check the units first. A reading of “50” is deficient in nmol/L but perfectly sufficient in ng/mL, and that single detail changes the whole interpretation.
How much vitamin D you actually need
The amount needed to correct a low level is usually higher than the amount needed to maintain a normal one. For general maintenance, the NIH sets the recommended dietary allowance at 600 IU (15 mcg) per day for adults aged 1 to 70, and 800 IU (20 mcg) per day for those 71 and older (NIH Office of Dietary Supplements). Those figures assume minimal sun exposure and are aimed at bone health across the population.
Correcting an established deficiency is a different job. Clinicians often use a higher loading approach for several weeks, then step down to a maintenance dose, with the exact plan tailored to how low you started and why. The tolerable upper intake level for adults is set at 4,000 IU per day for long-term use without medical supervision, and going well beyond that on your own can cause harm rather than help. The right dose is the one that moves your level into range on a recheck, not the biggest number you can find on a bottle.
Food sources, with real amounts
Food alone rarely fixes a true deficiency, but it supports maintenance and shows why diet is such a weak lever for most people. Very few foods are naturally rich in vitamin D, and the richest are fatty fish:
- Wild-caught salmon: roughly 988 IU per 3.5-ounce serving, among the highest of any natural food (Healthline review of USDA data).
- Farmed salmon: around 441 IU per 3.5-ounce serving, less than wild but still substantial.
- Herring, sardines, and canned tuna: moderate amounts, roughly in the low hundreds of IU per serving.
- Egg yolks, beef liver, and cheese: small contributions, best thought of as top-ups.
- Fortified foods: milk, some plant milks, orange juice, and cereals carry added vitamin D, which is how many people get most of their dietary intake.
Do the math and the limitation is obvious. Even a generous salmon dinner a few times a week leaves a gap for someone starting deficient, which is exactly why supplements and sunlight, not diet alone, are the usual path back to normal.

The cofactors: calcium, magnesium, and parathyroid hormone
Vitamin D does not work in isolation, and a low result is best read alongside a few partners. Its main job is to help you absorb calcium, so when vitamin D runs low, blood calcium can dip. Your body responds by raising parathyroid hormone (PTH), which pulls calcium out of bone to keep blood levels steady. This is why a low vitamin D paired with a high PTH is a red flag that deficiency is already stressing your skeleton, and it often prompts more urgent treatment.
Magnesium matters too. The enzymes that convert vitamin D through its activation steps depend on magnesium, so a significant magnesium shortfall can blunt how well supplementation works. This is one reason a person who “does not respond” to vitamin D pills sometimes turns out to have an unaddressed magnesium issue. If your level stays stubbornly low despite consistent supplementation, this is worth raising with your clinician rather than simply escalating the dose.
Can vitamin D be too high?
Yes, and it is worth knowing because the fix for a low level should not overshoot into a high one. Vitamin D is fat-soluble, so unlike water-soluble vitamins your body cannot easily flush an excess. Toxicity is almost always caused by overusing high-dose supplements, not by sun or food. The core danger is hypercalcemia, too much calcium in the blood, which can cause nausea, vomiting, weakness, frequent urination, and in severe cases kidney stones or kidney damage (Harvard Health).
The practical lesson is balance. Correcting a deficiency does not mean pushing your number as high as possible. More is not better past the point of sufficiency, and megadoses taken without monitoring are the most common route to trouble. This is another reason a follow-up test after treatment is not optional bookkeeping, it confirms you landed in range rather than sailing past it.
Who should be tested, and how often
Major guidelines do not recommend screening every healthy adult, because widespread testing has not been shown to improve outcomes for people at low risk. Testing earns its place when there is a reason to expect a problem or a need to guide treatment. Consider a 25(OH)D test if you have:
- Bone disease such as osteoporosis or a fracture from a minor fall.
- A malabsorption condition like celiac or Crohn disease, or a history of weight-loss surgery.
- Chronic kidney or liver disease.
- Very limited sun exposure, darker skin, or older age combined with symptoms.
- Unexplained bone pain or muscle weakness.
For someone being treated for deficiency, a recheck at about 3 months confirms the plan is working, since it takes weeks for a new steady state to form. Once you are stable and the cause is under control, routine annual retesting is usually enough unless your situation changes.
Timing of the draw is less finicky than for some tests, because 25(OH)D moves slowly and does not require fasting. What does help is consistency: retesting through the same lab, at a similar time of year, removes two hidden sources of variation, seasonal sunlight and assay differences between labs. If you supplement, taking your dose with a meal that contains some fat improves absorption, since vitamin D is fat-soluble.
Common mistakes after a low result
A low number is easy to fix, but a handful of predictable missteps keep people stuck at the same reading months later. The most common is simply not taking the supplement consistently. Vitamin D corrects on a timescale of weeks, and skipping doses several times a week quietly halves the effective intake, so a level that should have climbed barely moves.
A few other traps to avoid:
- Taking it on an empty stomach: Vitamin D is fat-soluble, so absorption is noticeably better when the dose rides along with a meal that contains some fat rather than a glass of water first thing in the morning.
- Chasing the biggest bottle: Reaching for a very high dose without monitoring is not faster, it is riskier. The dose that lands you back in range on a recheck is the right one, not the largest number on the shelf.
- Rechecking too soon: Testing again after two or three weeks catches you before a new steady state has formed and can look falsely disappointing. A recheck at about 3 months tells the real story.
- Ignoring the cause: If a malabsorption condition or magnesium shortfall is the reason, more pills alone will not fix it. Treating the underlying driver is what makes the supplement work.
None of these are exotic. They are the ordinary reasons a motivated person retests and sees the same low value, then wonders why the plan failed when the plan was fine and the execution slipped.
Vitamin D across life stages
The same low number can carry a different weight depending on who is holding the report. Needs shift across the lifespan, and a result that is unremarkable for one person deserves closer attention in another.
In pregnancy, adequate vitamin D supports the developing skeleton and is commonly checked when there are risk factors, since deficiency in the mother can affect the baby. Breastfed infants are a special case, because breast milk is low in vitamin D, which is why pediatric guidance often includes a supplement for exclusively breastfed babies. In children, severe long-standing deficiency causes rickets, the growth-plate disorder that softens and bows developing bones.
At the other end of life, older adults face a double burden. Aging skin makes vitamin D less efficiently from the same sun, intake from food often falls short, and the fracture stakes are higher because bone is already thinner. This is why the NIH sets a higher recommended intake of 800 IU per day for adults 71 and older, and why a low result in an older person who has fallen or fractured is treated with more urgency than the same value in a healthy young adult. The number is the same. The context around it is not.
Curious where your vitamin D really sits?
Baseline vitamin D and 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Is a vitamin D level of 25 ng/mL too low?
A level of 25 ng/mL sits above the deficiency cutoff of 20 ng/mL but below the 30 ng/mL that many labs call sufficient. It is borderline rather than clearly deficient, so your clinician decides whether to act based on your bone health and symptoms.
How long does it take to correct low vitamin D?
Most people raise their level into the healthy range within 8 to 12 weeks of consistent supplementation, which is why clinicians usually recheck a 25(OH)D test after about 3 months rather than sooner.
Can low vitamin D make you tired?
Fatigue is one of the commonly reported symptoms of low vitamin D, according to Cleveland Clinic and MedlinePlus. However, tiredness has many causes, so a blood test is needed to confirm vitamin D is the reason before assuming it.
What is the most accurate vitamin D test?
The 25-hydroxyvitamin D (25(OH)D) test is the standard and most accurate way to assess vitamin D status, because it measures the storage form that reflects your overall supply. The active 1,25-dihydroxyvitamin D test is not used for routine deficiency screening.
Should everyone get their vitamin D tested?
No. Major guidelines recommend testing people at higher risk, such as those with bone disease, malabsorption, limited sun exposure, or unexplained muscle and bone pain, rather than screening every healthy adult.
Sources
- NIH Office of Dietary Supplements, Vitamin D Fact Sheet for Health Professionals
- Cleveland Clinic, Vitamin D Deficiency: Causes, Symptoms and Treatment
- MedlinePlus, 25-hydroxy vitamin D test
- StatPearls (NCBI), Vitamin D Deficiency
- Endocrine Society, Evaluation, Treatment, and Prevention of Vitamin D Deficiency Clinical Practice Guideline (2011)
- Endocrine Society, Vitamin D Insufficiency and Epistemic Humility Guideline Communication (2024)
- Cleveland Clinic, Osteomalacia: What It Is, Symptoms and Treatment
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


