Last updated June 2026. Educational content, not medical advice. TB-500 is not FDA-approved for human use. Consult a licensed clinician before starting any peptide protocol.
Short answer: TB-500 is a synthetic 7-amino-acid fragment, sequence Ac-LKKTETQ-OH, taken from residues 17 to 23 of thymosin beta-4, a 43-amino-acid protein that acts as the principal G-actin buffering molecule in most mammalian cells. By binding free globular actin and preventing it from polymerizing into rigid filaments, TB-500 accelerates the cell migration, angiogenesis, and inflammatory modulation that underlie tissue repair. As of June 2026, no published human trial has tested TB-500 specifically for musculoskeletal recovery, but its parent molecule has cleared Phase 2 and Phase 3 trials in ophthalmology and a 2025 human RCT in cardiac ischemia.
Before trying an unregulated peptide like TB-500, see what your own inflammation and recovery markers actually look like. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
What is TB-500 and where does it come from?
TB-500 is not a compound invented in a lab to hack recovery. It is a short synthetic copy of something your body makes constantly. Thymosin beta-4, the parent molecule, is one of the most abundant intracellular proteins in mammalian cells, present in every tissue type and elevated automatically at sites of injury. The full protein is 43 amino acids long and was originally isolated from the thymus gland, hence the “thymosin” in the name, though its function extends far beyond immune tissue.
TB-500 captures the functionally active core of thymosin beta-4: the seven-amino-acid sequence LKKTETQ that forms the actin-binding domain. This fragment was first described in a landmark 1991 paper in the Journal of Biological Chemistry by Safer, Elzinga, and Nachmias, who confirmed that thymosin beta-4 is identical to “Fx,” the G-actin-sequestering factor previously isolated from platelets. The LKKTETQ sequence is strongly conserved across all beta-thymosins, which tells you evolution has been protecting it for a long time.
In other words: TB-500 is not a novel molecule. It is a trimmed copy of something your cells already rely on.
How does TB-500 work at the cellular level?
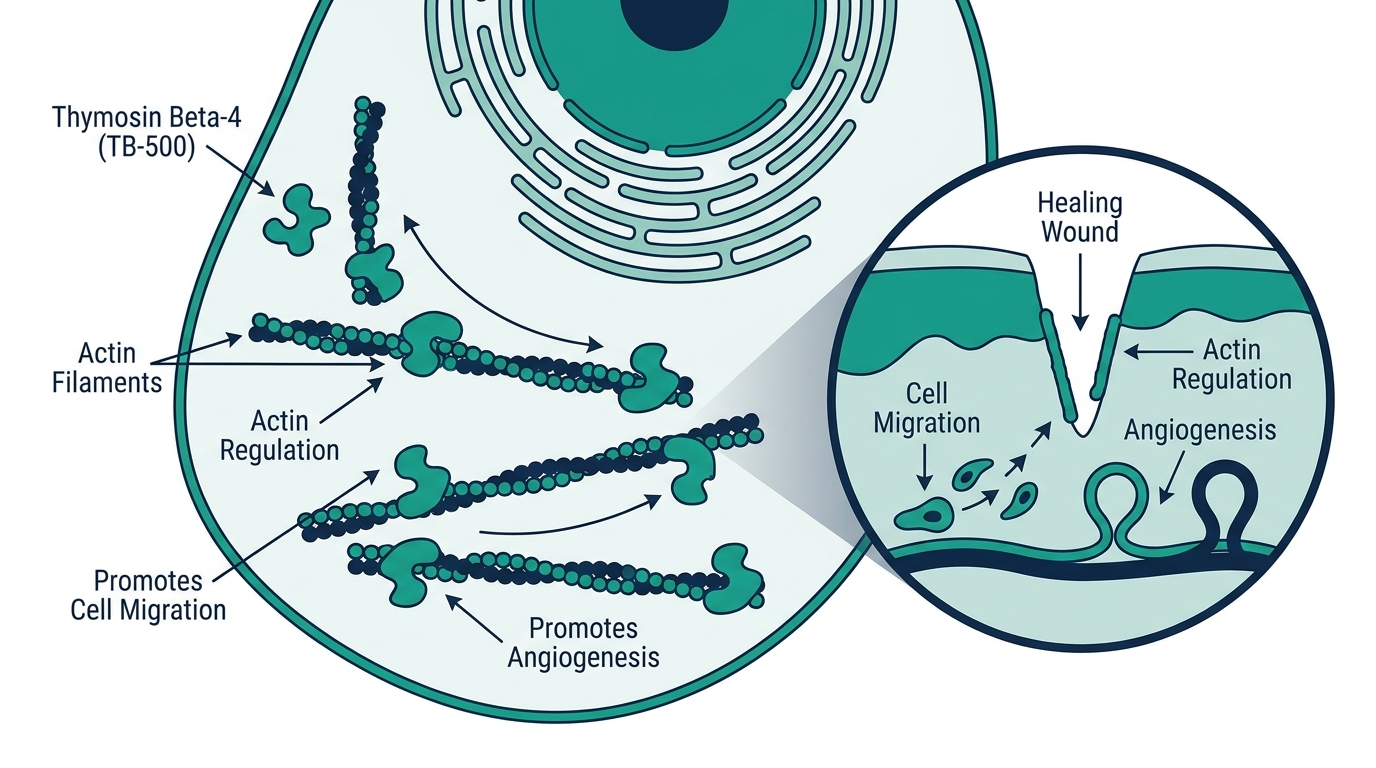
The central mechanism is actin sequestration. Inside every cell, actin exists in two forms: G-actin (globular, free monomers) and F-actin (filamentous, polymerized chains). The ratio between these two forms determines whether a cell is static or actively moving. When the body needs cells to migrate toward an injury, that ratio shifts toward G-actin.
TB-500 binds G-actin with high affinity and keeps it available in the free monomeric pool, preventing premature polymerization into rigid filaments. The effect is essentially a cellular speedometer: more free G-actin means faster cytoskeletal reorganization, faster cell migration to the wound site, and faster closure.
Beyond actin, TB-500 drives downstream signaling through several interconnected pathways:
- Angiogenesis via VEGF. TB-500 upregulates vascular endothelial growth factor (VEGF) by activating hypoxia-inducible factor 1 (HIF-1), which signals new blood vessel formation at injury sites. More blood supply equals faster delivery of oxygen, growth factors, and immune cells.
- Anti-inflammatory modulation. TB-500 downregulates pro-inflammatory cytokines and blunts the prolonged inflammatory phase that often delays recovery in chronic injuries.
- ErbB2/Raf1 cardioprotective signaling. In the 2025 Cardiovascular Research RCT of 96 STEMI patients, recombinant human thymosin beta-4 appeared to reduce cardiomyocyte death through this pathway. In the subgroup treated within 8 hours of reperfusion, infarcted areas were significantly smaller at 90-day follow-up compared to placebo, though the full-cohort primary endpoint did not reach statistical significance.
- Wnt/beta-catenin/Lef-1 pathway for hair and skin. Published research shows thymosin beta-4 regulates VEGF and MMP-2 through this pathway to stimulate hair follicle activation and angiogenesis around the dermal papilla, which explains why TB-500 is sometimes discussed in the context of hair loss, though that application has no clinical trial support.
A 2024 metabolite study by Rahaman et al. adds an important nuance: the wound-healing activity may actually come from a further breakdown metabolite, Ac-LKKTE, rather than the TB-500 fragment itself. This has not been resolved, but it is the kind of detail that matters for anyone designing a clinical trial.
What does the research actually show?
This is where honesty matters more than enthusiasm.
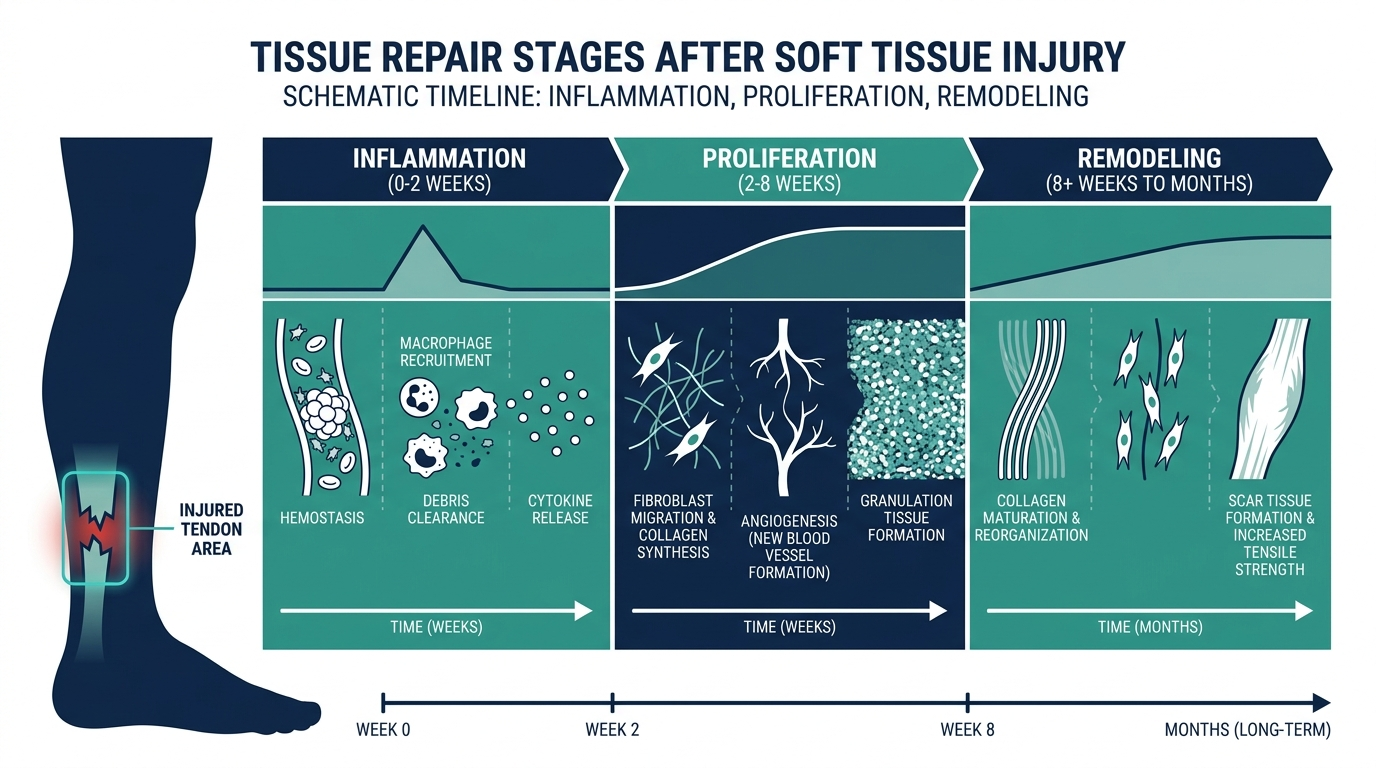
Preclinical evidence is substantial. Animal models consistently show thymosin beta-4 and TB-500 accelerating wound closure, improving tissue architecture, reducing scar formation, and supporting functional recovery across dermal, corneal, tendon, and cardiac models. Phase 2 ophthalmology trials of the parent compound showed a 35% reduction in ocular discomfort and a 59% reduction in corneal staining versus placebo at day 56. Phase 3 data in neurotrophic keratopathy showed fast, complete healing in the treatment group by week 4.
Human safety data for the TB-500 fragment specifically is limited. A 2021 Phase 1 safety trial in 84 healthy Chinese volunteers found the compound well tolerated at both single and multiple intravenous doses, with no dose-limiting toxicities and no serious adverse events. No human orthopedic efficacy trials of TB-500 itself have been published as of June 2026.
The anecdotal record is large but uncontrolled. Thousands of athletes and biohackers have reported faster recovery from tendon tears, ligament sprains, and muscle strains. Community forums on r/peptides and similar spaces treat the compound as near-consensus for soft-tissue injuries. These reports are real signals, but they are not controlled data, and they cannot separate TB-500’s effect from rest, physical therapy, and the natural course of healing.
Personally, I read that anecdotal record as a meaningful indication of biological activity in humans, not as a substitute for a real RCT. The Phase 2 dry-eye trials showed the molecule does something measurable in people; the animal models show it does something consistent across species. That is a stronger foundation than most research compounds have. But “stronger than most research compounds” is not the same as “proven safe and effective for injection into humans,” and that gap is exactly what nobody at a grey-market vendor will flag for you.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
How is TB-500 different from BPC-157?
TB-500 and BPC-157 are often mentioned together, and often confused. They are different molecules with different mechanisms and different tissue targets.
| Feature | TB-500 (Thymosin Beta-4 fragment) | BPC-157 (Body Protection Compound) |
|---|---|---|
| Origin | Endogenous: synthetic copy of a fragment of thymosin beta-4, a natural human protein | Synthetic: no known endogenous counterpart |
| Length | 7 amino acids (Ac-LKKTETQ-OH) | 15 amino acids |
| Primary mechanism | G-actin sequestration, cell migration, VEGF-driven angiogenesis | Nitric oxide signaling, growth factor upregulation, local vascular repair |
| Healing scope | Systemic: circulates body-wide, reaches multiple injury sites at once | Local: strongest effect when injected near the target tissue |
| Best-studied tissue | Skin, cornea, cardiac | Tendon, ligament, gut lining |
| WADA status | Prohibited, Section S2, in-competition and out-of-competition | Prohibited, Section S2 |
| FDA 503A category | Category 2 (pending July 2026 PCAC review for possible Category 1) | Removed from Category 2 on April 22, 2026; also pending July 2026 PCAC review |
| Human RCT data | Phase 1 safety (n=84); cardiac (n=96, parent molecule only) | No published human RCT for any indication |
The practical difference that most users care about: BPC-157 is the local sniper, TB-500 is the systemic sweep. If you have one injured shoulder, BPC-157 injected locally is theoretically more targeted. If you are dealing with diffuse muscle fatigue, multiple simultaneous injuries, or systemic inflammation, TB-500’s whole-body circulation is the argument for choosing it. The “Wolverine Stack” combining both is popular precisely because neither covers the other’s territory completely.
Do not believe anyone who tells you one is simply “better” than the other. They work through different pathways on different tissues. The comparison only makes sense against a specific injury context.
What is the regulatory status of TB-500 in 2026?
TB-500’s legal status is more complicated than a single yes or no, and it changed meaningfully in early 2026.
In late 2023, the FDA placed TB-500 on its 503A Category 2 list, designating it as a substance that may present significant safety risks, effectively prohibiting licensed U.S. compounding pharmacies from making it.
Then, on February 27, 2026, HHS Secretary Robert F. Kennedy Jr. announced that 14 of the 19 restricted peptides, including TB-500, BPC-157, CJC-1295, Ipamorelin, and Thymosin Alpha-1, are expected to return to legal compounding status. The FDA’s Pharmacy Compounding Advisory Committee is scheduled to formally review TB-500 and six other peptides at its July 23 to 24, 2026 meeting. A positive outcome would move TB-500 to Category 1, permitting licensed 503A compounding pharmacies to prescribe it with a physician’s order.
Three things that announcement does NOT mean:
- TB-500 is not FDA-approved as a finished drug. Compounding authorization and drug approval are separate legal categories.
- Moving to Category 1 does not affect the WADA Prohibited List. Athletes under WADA-compliant testing, including military personnel, remain strictly liable. TB-500 is prohibited in and out of competition under Section S2 of the 2026 WADA Prohibited List, and violations carry the maximum sanctions because peptide hormones are “non-specified substances.”
- The July 2026 meeting outcome is not guaranteed. If the PCAC has safety concerns, the path back to compounding could be delayed or narrowed.
The smart read on 2026: the regulatory door is swinging back toward the legal route. Anyone who bought TB-500 from a grey-market research vendor last year to avoid legal hurdles may find the legal route catches up with them before next year.
Who uses TB-500 and for what?
The honest map of current users divides into three groups with very different evidence bases.
Group 1: Athletes and physically active individuals. This is the largest group by volume. Weightlifters, CrossFit athletes, weekend warriors, and professional athletes recovering from tendon and muscle injuries represent the core of the forum-documented use case. The theory is sound: soft-tissue injuries involve exactly the cellular migration, angiogenesis, and inflammation modulation that thymosin beta-4 governs. The practice is almost entirely anecdotal.
Group 2: Longevity and biohacker community. People interested in systemic anti-inflammatory support, recovery optimization, and tissue resilience often include TB-500 in broader peptide stacks alongside BPC-157, GHK-Cu, and NAD+. Again, the preclinical rationale is coherent; controlled human data is absent.
Group 3: People pursuing the licensed telehealth route. A growing number of telehealth peptide clinics have begun prescribing TB-500, anticipating the July 2026 regulatory change. However, any clinic offering injectable TB-500 in June 2026 is doing so outside fully compliant compounding pharmacy channels, given the compound’s current Category 2 status. As noted in the template for this silo: [a clinic advertising injectable TB-500 before the PCAC meeting should prompt a question about which pharmacy is filling it and under what authorization.
Reported uses (preclinical or anecdotal, not proven in human RCTs):
– Soft-tissue injuries: muscle strains, ligament sprains, tendinopathy
– Post-surgical recovery support
– Chronic inflammatory conditions affecting joints or fascia
– Hair loss (based on mouse studies showing follicle activation)
– Cardiac recovery (based on the 2025 human RCT of the parent molecule)
– Dry eye and corneal healing (based on Phase 2 and Phase 3 trials of the parent molecule RGN-259)
What are the known risks and side effects?
The honest answer is: we do not have complete long-term safety data for TB-500 in humans, and anyone claiming otherwise is guessing.
What the 2021 Phase 1 trial (84 volunteers, intravenous administration, short follow-up) established is that single and multiple doses were well tolerated with no dose-limiting toxicities and no serious adverse events. That is a meaningful data point, not a comprehensive safety profile.
Reported side effects from anecdotal human use:
– Injection site reactions: redness, mild swelling, itching (typical for subcutaneous injection of any peptide)
– Nausea and dizziness, reported infrequently
– Headache, reported infrequently
– Fatigue in the first few days, attributed to systemic signaling activity
The theoretical concern that gets the most attention in clinical discussions is mitogenic potential. Thymosin beta-4 promotes cell migration and proliferation, which is what makes it interesting for wound healing and tissue repair. That same property raises a theoretical question about whether it could accelerate growth in existing occult tumors or precancerous tissue. No clinical evidence shows this in humans, but no long-term human trial has looked for it either. This is why the clinical guidance from physicians who discuss TB-500 consistently includes a contraindication for individuals with active or suspected malignancy.
A contraindication that gets less attention but matters: TB-500 should not be used during pregnancy. The compound’s effects on angiogenesis and cell migration in a developing fetus are unknown.
What is the legitimate route to TB-500 in 2026?
The grey-market route, buying a research vial labeled “not for human use,” is the one most people currently use and the one with the most exposure. This is the same landscape that just consumed Peptide Sciences and Science.bio, both of which vanished with no warning, no refunds, and no accountability.
The emerging licensed route, which is where this is heading, runs through telehealth clinics that work with compliant 503A compounding pharmacies. After the July 2026 PCAC meeting, if TB-500 returns to Category 1, that route becomes fully legible and verifiable. A legitimate provider will show you the named pharmacy, the physician prescribing, baseline labs before the first dose, and a product label from a regulated facility.
The price difference is real: research-grade TB-500 vials run roughly $100 to $200 per month in grey-market supply, versus $300 to $600 monthly for a full telehealth peptide recovery protocol with monitoring and pharmacy-grade product. But the grey-market price does not include what you are actually buying: the identity test, the dose verification, the clinical oversight, and the accountability if anything goes wrong.
Telehealth GLP-1 program with provider visits and pharmacy coordination.
How is TB-500 typically handled in a research setting? (Educational overview only)
This section is for educational context only. TB-500 is not FDA-approved for human use. Dosing decisions require a licensed clinician.
In the research and clinical discussion literature, TB-500 is described as a lyophilized (freeze-dried) powder that requires reconstitution with bacteriostatic water before administration. Reconstitution involves injecting bacteriostatic water into the vial without agitating the powder, letting it dissolve, and calculating the concentration carefully. The concentration math matters: a decimal error does not produce a slightly different dose, it produces a dose that is off by a factor of ten.
Reported protocols in the community literature use a “loading phase” followed by a “maintenance phase,” with the loading phase typically running four to eight weeks and maintenance running once or twice per month. The administration route is subcutaneous injection, typically into a skin fold near the abdomen or thigh, similar to insulin administration.
Because TB-500 is described as systemically active rather than locally targeted, it does not require injection near the injury site, which distinguishes it from BPC-157. This means reconstitution accuracy matters more than injection site selection.
None of this constitutes a medical protocol. A licensed physician prescribing TB-500 after the PCAC decision will provide a dose, a pharmacy-prepared product, and instructions from someone who holds a license and carries accountability for them.
Turn what you just learned into action.
Superpower lets you test 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
What is TB-500 peptide used for?
TB-500 is used primarily for soft-tissue recovery, including muscle strains, ligament sprains, and tendinopathy, based on preclinical animal studies and a large anecdotal record in athletes. Its parent molecule, thymosin beta-4, has Phase 2 and Phase 3 clinical evidence for dry eye disease and corneal repair, and a 2025 human RCT showed promise in cardiac ischemia recovery. No human RCT has been published specifically for TB-500 in any orthopedic or musculoskeletal indication.
Is TB-500 the same as thymosin beta-4?
No, though they are closely related. Thymosin beta-4 is the full 43-amino-acid endogenous protein your body produces. TB-500 is a synthetic 7-amino-acid fragment (Ac-LKKTETQ-OH) corresponding to residues 17 to 23 of the full protein, covering its actin-binding domain. TB-500 was synthesized as a more stable, injectable form of the active core of the parent molecule. Most clinical trials have studied the full-length protein (sometimes sold under the name RGN-259), not the fragment.
Is TB-500 legal in the US in 2026?
It occupies a grey zone. The FDA placed TB-500 on the 503A Category 2 restricted list in 2023, prohibiting compounding pharmacies from dispensing it. In February 2026, HHS signaled that TB-500 and about 13 other peptides are expected to return to Category 1 (permitted for compounding), with a formal FDA Pharmacy Compounding Advisory Committee review scheduled for July 23 to 24, 2026. Selling TB-500 “for research use only” is permitted. Using it or prescribing it for human use outside a compliant pharmacy is not.
Is TB-500 banned in sports?
Yes. TB-500 is prohibited at all times (in-competition and out-of-competition) under the 2026 WADA Prohibited List, Section S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). It is classified as a non-specified substance, meaning violations carry the maximum sanctions. The FDA reclassification process has no bearing on the WADA ruleset.
How is TB-500 different from BPC-157?
TB-500 is a synthetic fragment of an endogenous human protein; BPC-157 is a wholly synthetic compound with no known naturally occurring counterpart. TB-500 works systemically, circulating body-wide to support multiple tissues simultaneously through actin regulation and VEGF signaling. BPC-157 works locally, with the strongest effect when injected near the target tissue, through nitric oxide and growth factor pathways. They are often stacked together (“Wolverine Stack”) because neither covers the other’s mechanism or tissue targets.
What does the research actually show for TB-500?
The strongest evidence is for the full-length thymosin beta-4 parent molecule, not TB-500 specifically. Phase 2 human trials in dry eye disease showed 35% reduction in ocular discomfort and 59% reduction in corneal staining versus placebo. A 2025 RCT of 96 STEMI patients showed reduced infarct size in those treated with recombinant thymosin beta-4 within 8 hours of reperfusion, though the overall primary endpoint was not statistically significant. TB-500 as a fragment has Phase 1 human safety data (84 volunteers, well tolerated) but no published human efficacy trial for any orthopedic or tissue-repair indication.
What are the side effects of TB-500?
Reported side effects include injection site reactions (redness, mild swelling, itching), nausea, headache, and brief fatigue. The Phase 1 safety trial found no dose-limiting toxicities and no serious adverse events in 84 volunteers. Long-term human safety data is not available. A theoretical concern about cell-proliferation effects in people with existing or occult malignancy has not been studied. TB-500 is contraindicated for pregnant individuals and those with active or suspected cancer.
Telehealth GLP-1 program with provider visits and pharmacy coordination.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources:
– FDA 503A bulk drug substances list: https://www.fda.gov/drugs/human-drug-compounding/bulk-drug-substances-used-compounding-under-section-503a-fdc-act
– WADA 2026 Prohibited List: https://www.wada-ama.org/en/prohibited-list
– Pubmed: Zhu et al. 2025 Cardiovascular Research RCT of rhTB4 in STEMI (96 patients): https://pubmed.ncbi.nlm.nih.gov/41229390/
– Pubmed: Sosne et al. 2015 Phase 2 thymosin beta-4 dry eye trial: https://pubmed.ncbi.nlm.nih.gov/25826322/
– Pubmed: The actin binding site on thymosin beta4 promotes angiogenesis (2003): https://pubmed.ncbi.nlm.nih.gov/14500546/
– PMC: Thymosin Beta-4 Induces Mouse Hair Growth: https://pmc.ncbi.nlm.nih.gov/articles/PMC4470810/
– Pharmacy Times: The peptide reclassification pharmacist analysis: https://www.pharmacytimes.com/view/the-peptide-reclassification-everyone-s-talking-about-a-pharmacist-s-take-on-what-rfk-jr-s-announcement-actually-means
– Meto blog: FDA July 2026 peptide advisory meeting overview: https://meto.co/blog/fda-peptide-approval-2026
– Superpower.com: TB-500 guide (actin-binding domain, regulatory status): https://superpower.com/guides/tb-500
– Dr. Jeffrey Peng MD: TB-500 for injury recovery, research review: https://www.jeffreypengmd.com/post/tb-500-for-injury-recovery-what-the-research-actually-shows
– Wikipedia: Thymosin beta-4 structure and sequence: https://en.wikipedia.org/wiki/Thymosin_beta-4
– BSCG: TB-500 WADA status, sports and military bans: https://www.bscg.org/blogs/single/tb-500-status-risks-and-bans-in-sport-and-military
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.