
You ordered a herpes blood test, maybe through an online lab or as part of a full STI panel, and now you are staring at a result that says positive or negative and wondering how much you can actually trust it. It is a fair question, and the honest answer is more complicated than most lab portals let on. A herpes blood test is not a simple yes or no machine. It is a probability tool, and how reliable your result is depends heavily on which type of herpes it found, how strong the signal was, and how common the infection is in people like you.
A positive herpes result raises more questions than it answers. Curious what a full health panel would show too? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Here is the part that surprises people. A positive herpes blood test, especially a weakly positive one, can be wrong almost as often as it is right in certain situations. Knowing why is the difference between a needless scare and a clear head.
How accurate is a herpes blood test?
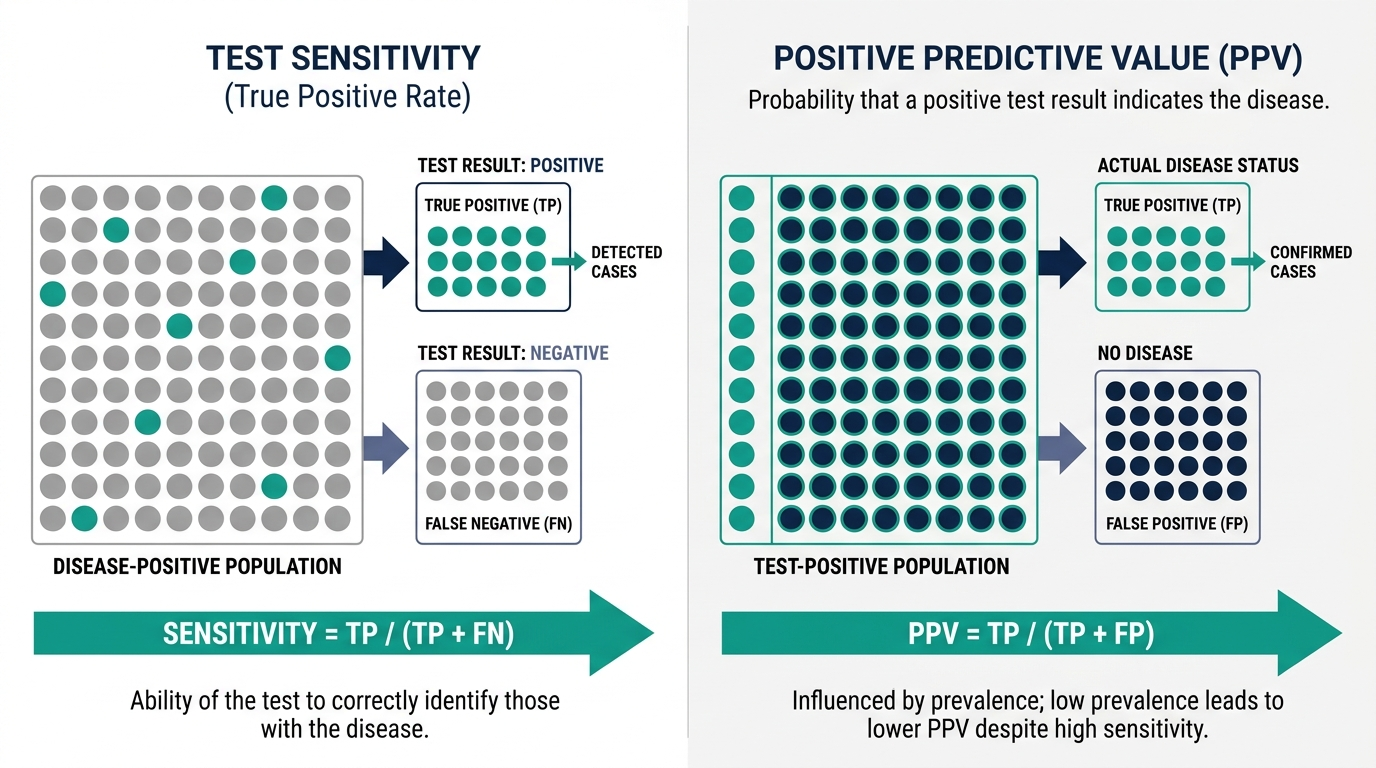
How accurate is a herpes blood test depends almost entirely on which virus it is detecting and how strong the result is. A modern type-specific IgG blood test is generally very good at correctly identifying people who truly carry HSV-2, with sensitivity often reported around 80 to 98 percent and specificity in good studies above 90 percent (Performance of Focus ELISA Tests, PMC). The problem is not whether the test can find antibodies. The problem is that a positive result is not the same thing as a true infection, and the gap between those two ideas is where most of the confusion lives.
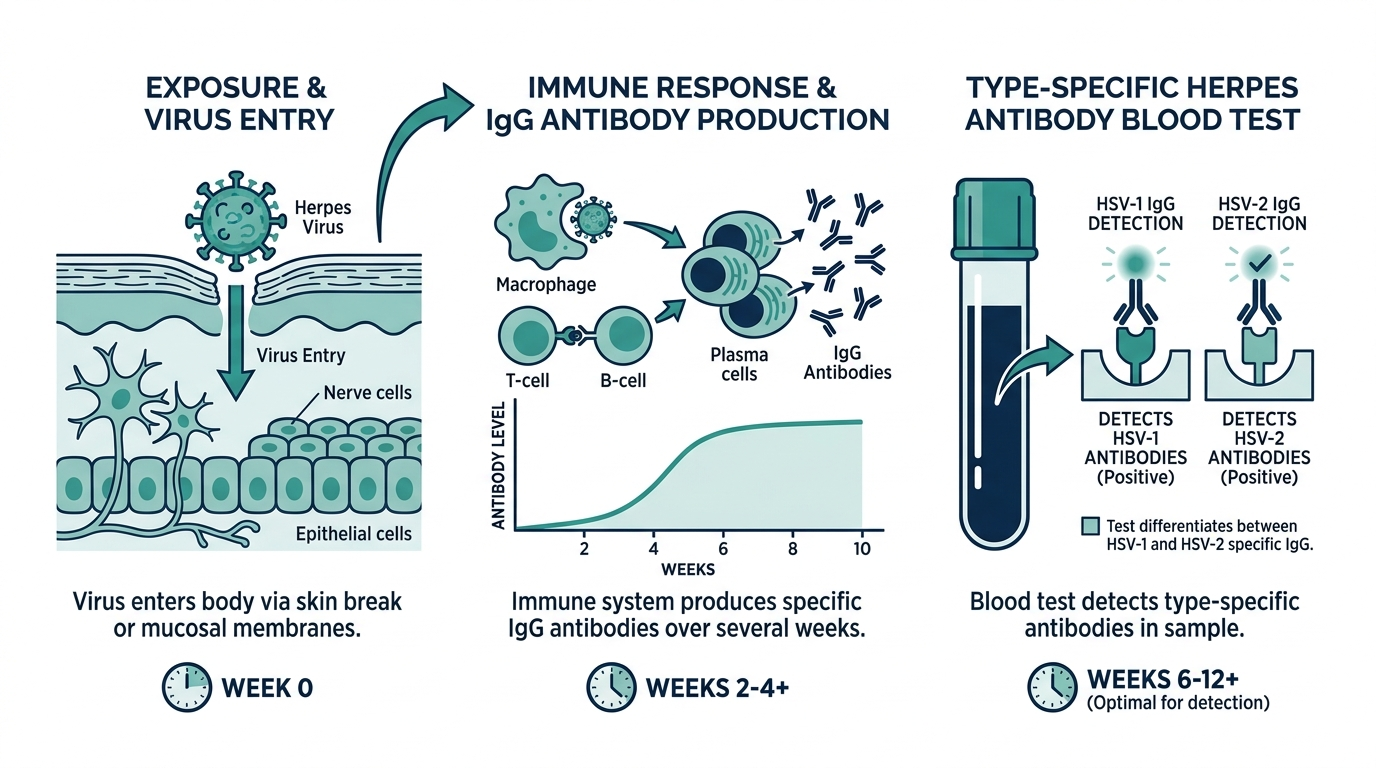
A herpes blood test does not look for the virus itself. It looks for antibodies, the proteins your immune system makes after it has met HSV-1 or HSV-2 (MedlinePlus, serum herpes simplex antibodies). That single fact drives everything below. It means the test can tell you that you were exposed at some point, but it cannot tell you when, where on your body, or whether you are infectious today.

What kind of herpes blood test is considered accurate?
The accurate kind is a type-specific IgG antibody test, and the kind to avoid is an IgM test. Type-specific tests, often based on a viral protein called glycoprotein G, can separately detect antibodies to HSV-1 and HSV-2, which matters because the two viruses behave very differently and carry very different implications (MedlinePlus, HSV test).
IgM tests are a common trap. They are marketed as detecting recent or new infection, but in practice they cannot reliably tell HSV-1 from HSV-2, they can turn positive during old reactivations rather than new infections, and they produce a high rate of misleading results. If a lab panel hands you an HSV IgM number, treat it with deep skepticism and ask whether a type-specific IgG test was run instead. The IgG version is the one the evidence supports for figuring out whether you carry the virus (MedlinePlus, HSV test).
How accurate are herpes blood tests for HSV-2 specifically?
For HSV-2, the genital strain most people worry about, accuracy is genuinely good when the positive signal is strong, and genuinely shaky when it is weak. The most widely used test, a HerpeSelect type ELISA, has been shown to catch nearly everyone who truly has HSV-2 antibodies, with one study of university students reporting 100 percent sensitivity and 94 percent specificity (Performance of Focus ELISA Tests, PMC). On paper those are reassuring numbers.
The catch is the index value, the number behind your positive result. Many labs call anything above 1.1 a positive, but results in the low positive zone, roughly 1.1 to 3.5, are far less trustworthy than results well above that. In the same university study, positives clustered at low index values were frequently false alarms, which is why the authors suggested using a higher cutoff to define a true positive (Performance of Focus ELISA Tests, PMC). In plain terms, a strongly positive HSV-2 result is usually real. A barely positive one often is not.
Are herpes blood tests accurate for HSV-1?
Herpes blood tests are noticeably less reliable for HSV-1 than for HSV-2, and most people are not told this. In the university study, the type-specific test detected only about 69 percent of people who truly carried HSV-1 antibodies, even though its specificity was high at roughly 98 percent (Performance of Focus ELISA Tests, PMC). That low sensitivity means a meaningful share of people with HSV-1 will get a falsely negative blood result.
This matters because HSV-1 is extremely common, mostly causes oral cold sores, and increasingly causes genital herpes too. A negative HSV-1 blood test does not firmly rule out the virus the way a negative HSV-2 result tends to. If your real question is about oral or genital HSV-1 and you have an actual sore, a swab of the lesion is a far better tool than blood.

Why do herpes blood tests give false positives?
False positives happen mostly because of weak signals in people who are unlikely to have the infection in the first place, and the math behind this is the single most important thing to understand about herpes testing. When a test is used to screen a low-risk population, even a small false positive rate produces a flood of wrong positives relative to true ones.
One study illustrated this starkly. Among university students with no history of genital herpes, the HSV-2 test flagged a number of positives, but its positive predictive value was only about 37.5 percent, meaning most of those positives were false (Performance of Focus ELISA Tests, PMC). The cause was not a broken test. It was low prevalence colliding with low index values.
This is exactly why confirmatory testing exists. Researchers have shown that running a second, different method such as the biokit HSV-2 rapid assay on top of an initial ELISA positive sharply improves the predictive value and weeds out false alarms (biokit HSV-2 Rapid Assay study, NCBI). A single positive ELISA, especially a low one, should be treated as a flag to confirm, not a verdict.
The insider truth: a positive result and a true infection are not the same thing
Here is what clinicians who order these tests understand and patients rarely hear. The accuracy of your herpes blood test is not a fixed property of the test. It shifts with your risk. The exact same test, with the exact same specificity, becomes dramatically less trustworthy when used on someone with no symptoms and no known exposure.
Think of it like a smoke detector that occasionally beeps at burnt toast. In a building that catches fire often, almost every beep means real fire. In a building that almost never burns, most beeps are toast. The detector did not change. The base rate did. A herpes blood test in a low-risk person with a borderline index value is mostly hearing toast, which is why a weak positive in someone with no symptoms should trigger a confirmatory test rather than a diagnosis (biokit HSV-2 Rapid Assay study, NCBI).
The flip side matters just as much. A negative result is not bulletproof either. Your body can take up to three months to make detectable HSV antibodies, so a test run too soon after a possible exposure can come back negative even when you are truly infected (MedlinePlus, HSV test). Timing is part of accuracy.
When should you get a herpes blood test for it to be accurate?
For the most accurate result, you generally need to wait long enough for antibodies to build, often around 12 to 16 weeks after a possible exposure, because testing inside the window period risks a false negative. The body simply has not finished its antibody response yet (MedlinePlus, serum herpes simplex antibodies).
It also helps to be clear about what you are testing for. A blood test answers the question have I ever been infected with this virus. It does not tell you whether a sore you have right now is herpes (Cleveland Clinic, genital herpes). If you have an active lesion, the more accurate path is a direct swab of that sore for a PCR or culture test, which looks for the virus itself rather than your immune memory of it.
Why national guidelines actually advise against screening most people
Here is a fact that stuns people who ordered a herpes test as part of a “complete” STI panel: expert bodies specifically recommend against routinely running this blood test on people without symptoms. This is not obscure caution. It is a formal position built on the exact accuracy problems described above.
The U.S. Preventive Services Task Force recommends against routine serologic screening for genital herpes in asymptomatic adolescents and adults, including pregnant people, a stance it reaffirmed and graded as a “D” recommendation, meaning the harms outweigh the benefits (U.S. Preventive Services Task Force). CDC guidance likewise does not recommend HSV-2 serologic screening in the general population (CDC).
The reasoning is precisely the base-rate problem. Because the tests have limited positive predictive value and produce a high rate of false positives when used on people unlikely to be infected, screening asymptomatic individuals does not improve their health and can cause real harm: anxiety, relationship strain, and stigma from a result that may well be wrong (U.S. Preventive Services Task Force). If a general STI panel you ordered online included HSV IgG by default, that is worth knowing. A positive from such a panel, in a person with no symptoms, is exactly the scenario where the result is least trustworthy.
Blood test versus swab: matching the test to your situation
One of the most common and consequential mistakes is using the wrong test for the question you actually have. A blood test and a lesion swab answer completely different questions, and picking the wrong one wastes time or produces a misleading answer.
| Your situation | Better test | Why |
|---|---|---|
| You have an active sore or blister right now | Swab of the lesion (PCR or culture) | Detects the actual virus in the sore, confirms location and type, far more definitive |
| No symptoms, wondering about past exposure | Type-specific IgG blood test, interpreted cautiously | Detects antibodies, but with the false-positive limits above |
| Recent possible exposure, no sore yet | Wait, then blood test at the right window | Antibodies take up to three months to develop |
The headline is simple: if you have a sore, do not rely on blood. A direct swab of an active lesion for PCR is the most accurate way to confirm herpes, because it finds the virus itself rather than your immune memory of a past encounter (Cleveland Clinic). Blood testing earns its place only when there is no lesion to swab and the question is genuinely about prior exposure.
What to actually do with a positive result
If you are holding a positive herpes blood test, resist the urge to treat it as a settled diagnosis, especially if it was unexpected. Work through it in order.
- Find your index value. The strength of the positive matters. A strongly positive HSV-2 result is usually real, while a low positive in the roughly 1.1 to 3.5 range is much more likely to be a false alarm and warrants confirmation (PMC).
- Ask for a confirmatory test. Running a second, different method on a low positive sharply reduces false positives, which is why a single low ELISA should prompt confirmation rather than a diagnosis (NCBI).
- Check whether it was IgG or IgM. If the positive came from an IgM test, its reliability is poor and a type-specific IgG test should be run instead (MedlinePlus).
- Put your own risk in the picture. The same result means different things depending on symptoms and exposure history. Bring both to a clinician who can interpret the number in context rather than in isolation.
The goal is to avoid the two classic errors: accepting a false positive as truth, and dismissing a true positive out of denial. The index value, a confirmatory test, and an honest look at your own risk are the three tools that separate those cases.

HSV-1 and HSV-2: why the distinction changes the meaning
People often treat “herpes” as one thing, but which type you carry substantially changes what a positive result implies, and a good test reports them separately for exactly this reason.
- HSV-1 is extremely common and classically causes oral cold sores, though it increasingly causes genital infections too, usually through oral contact. A large share of the adult population carries it, often acquired in childhood with no connection to sexual activity.
- HSV-2 is the type most associated with genital herpes and recurrent genital outbreaks, and it is the one people usually mean when they worry about a sexually transmitted infection.
This is why a bare “herpes positive” is nearly meaningless without the type. A positive HSV-1 antibody test in an adult may simply reflect a cold sore infection from childhood and says nothing about recent sexual exposure. A positive HSV-2, when genuinely confirmed, carries different implications for outbreaks and transmission. Any result worth acting on tells you which virus it found, and if yours does not, that is the first thing to clarify.
What a confirmed result means for outbreaks and partners
If confirmatory testing establishes that you genuinely carry HSV, it helps to keep the reality in proportion, because the diagnosis is far more common and manageable than the stigma suggests. A large fraction of the population carries one type or another, most without ever knowing, and many never have a noticeable outbreak.
A few grounded points to discuss with a clinician rather than infer from a lab portal:
- Many carriers are asymptomatic or barely symptomatic, which is part of why the virus is so widespread and why a blood-test positive so often surprises people.
- Transmission can occur even without visible sores, through asymptomatic viral shedding, which is why open conversation with partners matters more than waiting for an outbreak.
- Antiviral medication can reduce both outbreak frequency and transmission risk, and is a routine, effective option your clinician can discuss.
- A positive antibody test does not tell you when or from whom you acquired the virus, so it should never be used to assign blame within a relationship.
The through line of this entire topic is that a herpes blood test is a probability tool, not an oracle. Its number only becomes meaningful when read alongside the virus type, the strength of the signal, your symptoms, your risk, and, when the result is weak or unexpected, a confirmatory test. Handled that way, it informs rather than frightens.
Common misconceptions that cause needless worry
Several persistent myths make herpes testing far more distressing than it needs to be. Correcting them defuses most of the panic a surprise positive creates.
- “A positive blood test means I am infectious right now.” It does not. The test detects past exposure through antibodies, not active virus or current contagiousness. Only a swab of an active sore speaks to what is happening today.
- “Any positive is a definite diagnosis.” In low-risk, asymptomatic people, a weak positive is often false, which is exactly why confirmatory testing and index values matter so much (NCBI).
- “A negative test guarantees I am clear.” Not if you tested inside the window period, since antibodies can take up to three months to appear (MedlinePlus). HSV-1 blood tests also miss a meaningful share of true carriers.
- “The test tells me when and from whom I caught it.” It cannot. Antibody testing gives no timeline and no source, so it should never be used to assign blame.
Read against these corrections, a herpes blood result becomes what it actually is: one probabilistic data point, most useful when the signal is strong, the type is specified, and the interpretation happens with a clinician rather than alone in front of a portal.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
How accurate is a herpes blood test overall?
A type-specific IgG blood test is generally accurate for confirmed HSV-2, with sensitivity often around 80 to 98 percent, but its reliability drops sharply for weakly positive results and in low-risk people, where many positives turn out to be false (Performance of Focus ELISA Tests, PMC). A strong positive is usually real, a borderline one often needs confirming.
Can a herpes blood test be wrong?
Yes, in both directions. It can be falsely positive, especially at low index values in low-prevalence groups where one study found a positive predictive value of only about 37.5 percent, and falsely negative if taken too soon after exposure before antibodies develop (Performance of Focus ELISA Tests, PMC).
Are herpes blood tests accurate for HSV-1?
Less so than for HSV-2. Type-specific blood tests have detected only around 69 percent of true HSV-1 carriers in some studies, so a negative HSV-1 blood result does not reliably rule out the virus (Performance of Focus ELISA Tests, PMC). For an active sore, a swab is more accurate.
Why does my positive herpes test need to be confirmed?
Because a single positive ELISA, particularly a weak one, has a high chance of being false in low-risk people. Running a second, different method such as the biokit assay improves accuracy and filters out false positives (biokit HSV-2 Rapid Assay study, NCBI).
How long after exposure should I wait to test?
Generally around 12 to 16 weeks, because your body can take up to three months to produce detectable HSV antibodies, and testing earlier risks a false negative (MedlinePlus, HSV test).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


