Phosphorus rarely gets its own test, so where does yours actually sit? Find out alongside 100+ other biomarkers. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
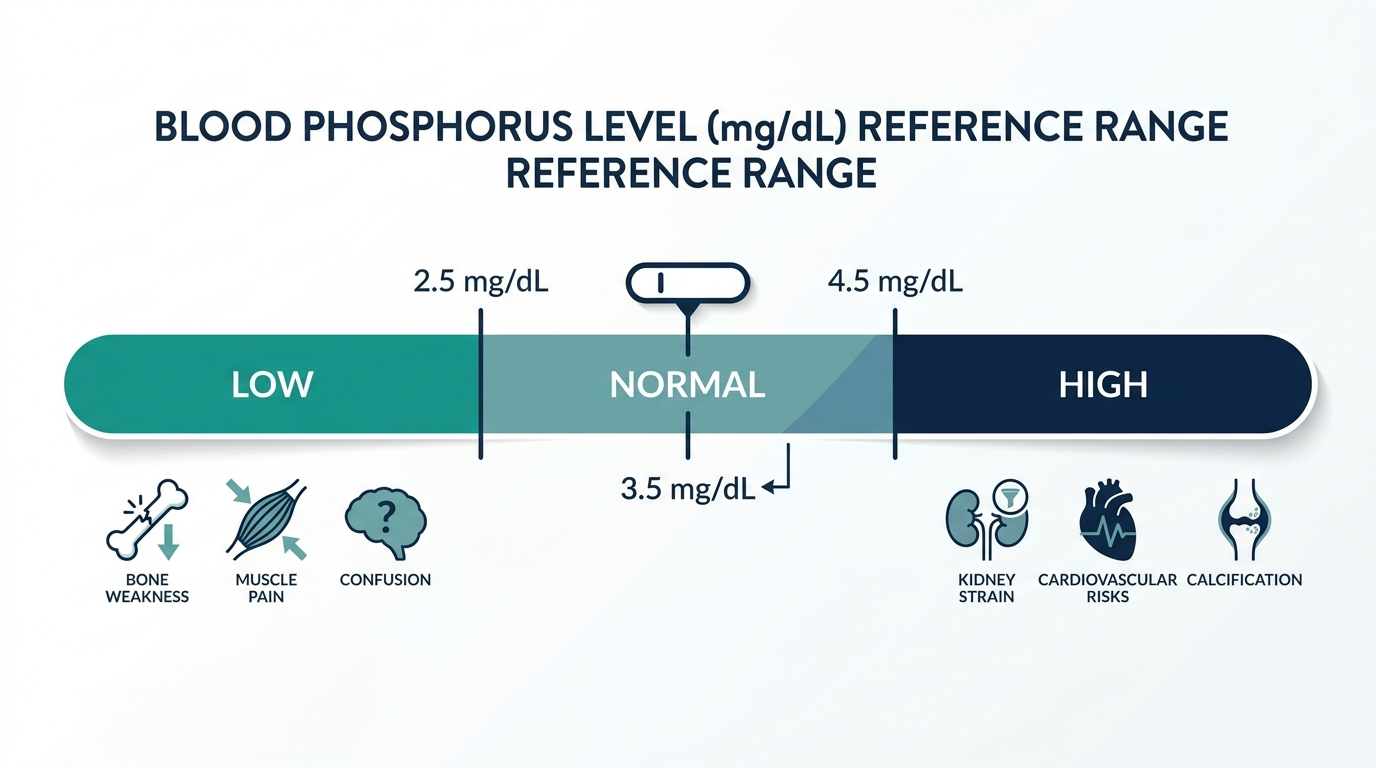
- A phosphorus blood test, also called a serum phosphate test, measures the amount of phosphate mineral circulating in your blood, with a normal adult range of roughly 2.5 to 4.5 mg/dL (Cleveland Clinic).
- High phosphorus (above 4.5 mg/dL, called hyperphosphatemia) is most often caused by chronic kidney disease, because failing kidneys cannot clear excess phosphate from the blood (MSD Manual).
- Low phosphorus (below 2.5 mg/dL, called hypophosphatemia) can result from malnutrition, alcohol use disorder, refeeding after starvation, or overactive parathyroid glands, and severe cases can weaken muscles and bones (Cleveland Clinic).
What is phosphorus in a blood test?
A phosphorus blood test measures phosphate, the form phosphorus takes inside your body, dissolved in your blood. The normal adult reference range is about 2.5 to 4.5 mg/dL according to Cleveland Clinic, though exact cutoffs vary slightly by laboratory. Phosphorus is the body’s second most abundant mineral after calcium, and roughly 85 percent of it is stored in your bones and teeth.
Most labs report the result as “phosphorus” or “phosphate,” and the two terms are used interchangeably on a panel. Only about 1 percent of your total body phosphorus sits in the bloodstream, so a blood test captures just a thin slice of the whole picture. Children and teenagers normally run higher than adults, often up to 4.5 to 6.5 mg/dL, because growing bones pull in more phosphate (MedlinePlus). Your clinician reads the number against your kidney function, calcium, and vitamin D status rather than in isolation.

Why is phosphorus measured?
Phosphorus is measured to check kidney function, bone health, and parathyroid activity, since these systems jointly control phosphate balance. Because the kidneys clear most excess phosphate, an abnormal result is one of the early metabolic signals seen in chronic kidney disease, which is the most common cause of high phosphorus (MSD Manual).
Phosphate does heavy lifting throughout the body. It is a structural part of bone and teeth, it forms the backbone of DNA and RNA, and it powers energy transfer through ATP, the molecule your cells use as fuel. A doctor may order this test as part of a metabolic panel, when monitoring kidney disease, or when symptoms point to a mineral imbalance.
- Kidney monitoring: tracking phosphate in people with reduced kidney function or on dialysis.
- Bone and parathyroid disorders: investigating abnormal calcium, vitamin D problems, or parathyroid disease.
- Nutritional concerns: evaluating malnutrition, alcohol use disorder, or recovery from severe illness.
What does a high phosphorus mean?
High phosphorus, called hyperphosphatemia, is a level above roughly 4.5 mg/dL and most commonly signals that the kidneys are not clearing phosphate well (MSD Manual). Hyperphosphatemia typically develops once chronic kidney disease has destroyed about 40 to 50 percent of functioning kidney tissue, because the remaining kidney cannot excrete the full daily phosphate load (NIH PMC).
Beyond kidney disease, high phosphate can come from underactive parathyroid glands (hypoparathyroidism), too much vitamin D, tissue breakdown from severe injury, or certain phosphate-containing laxatives. Many people with high phosphorus feel no symptoms at first. Over time, persistently elevated phosphate pulls calcium out of bones and can deposit calcium into blood vessels and soft tissue, raising cardiovascular risk in kidney patients. This is why the National Kidney Foundation flags phosphorus control as a priority in advanced kidney disease, often managed with diet changes and phosphate binders taken with meals (National Kidney Foundation).
What does a low phosphorus mean?
Low phosphorus, called hypophosphatemia, is a level below about 2.5 mg/dL and usually reflects poor intake, poor absorption, or phosphate shifting into cells rather than true depletion (Cleveland Clinic). It is far less common than high phosphorus in the general population but appears often in hospitalized and critically ill patients.
Frequent causes include alcohol use disorder, severe malnutrition, overactive parathyroid glands (hyperparathyroidism), vitamin D deficiency, and refeeding syndrome, where phosphate plummets when nutrition restarts after starvation. Certain antacids that bind phosphate and diabetic ketoacidosis treatment can also drop the level.
- Mild low phosphorus: often silent and corrected by treating the underlying cause.
- Severe low phosphorus: can cause muscle weakness, confusion, bone pain, and in extreme cases breathing or heart problems.
Because symptoms overlap with many conditions, clinicians confirm the cause before treating, and they replace phosphate cautiously to avoid swinging the level too high.

How is phosphorus interpreted with other markers?
Phosphorus is almost never read alone, because it moves in tandem with calcium, parathyroid hormone (PTH), and vitamin D. As a rule of thumb, phosphate and calcium often shift in opposite directions, so a doctor reviews them together to locate the problem (Cleveland Clinic).
The classic pattern in advanced kidney disease is high phosphate with low or normal calcium and high PTH, a state called secondary hyperparathyroidism (NIH PMC). In hypoparathyroidism the opposite shows up, with high phosphate and low calcium driven by too little PTH. Vitamin D status matters too, since active vitamin D increases absorption of both minerals from the gut.
- Calcium: paired with phosphorus to assess bone and parathyroid disorders.
- PTH: the hormone that fine tunes how much phosphate the kidneys excrete.
- Creatinine and eGFR: kidney function tests that explain most high phosphorus results.
The insider nuance most patients miss
One detail clinicians watch that patients rarely hear about: the timing and conditions of your blood draw can sway a phosphorus result enough to look abnormal when nothing is wrong. Phosphate has a natural daily rhythm, dipping in the morning and rising later in the day, and a recent high-carbohydrate meal or an insulin surge can pull phosphate into cells and temporarily lower the reading.
Two lab artifacts also matter. Hemolysis, where red blood cells rupture in a poorly handled sample, leaks phosphate out and falsely raises the number, which is why a flagged result is sometimes just a re-draw away from normal. This is also why most clinicians prefer a fasting morning sample for the cleanest comparison over time. The practical takeaway is simple: one borderline phosphorus value is a prompt to recheck and look at the trend with calcium and kidney markers, not a diagnosis on its own.
What phosphate actually does in the body
Phosphorus is easy to overlook, but it is one of the busiest minerals you have. Understanding its jobs explains why both a high and a low value can matter. Phosphate, the form phosphorus takes in the body, is involved in nearly every cell.
- Energy currency: phosphate is the “P” in ATP, the molecule cells use to store and spend energy. Almost every energy-requiring process depends on it, which is why severe depletion can weaken muscles and even breathing.
- Bone and teeth: about 85 percent of body phosphorus is locked in the skeleton as calcium phosphate, giving bone its hardness alongside calcium.
- Genetic material: phosphate forms the backbone of DNA and RNA, so it is essential for making new cells.
- Cell membranes: phospholipids, built around phosphate, make up the walls of every cell.
- Acid-base balance: phosphate acts as a buffer that helps keep blood at the right pH.
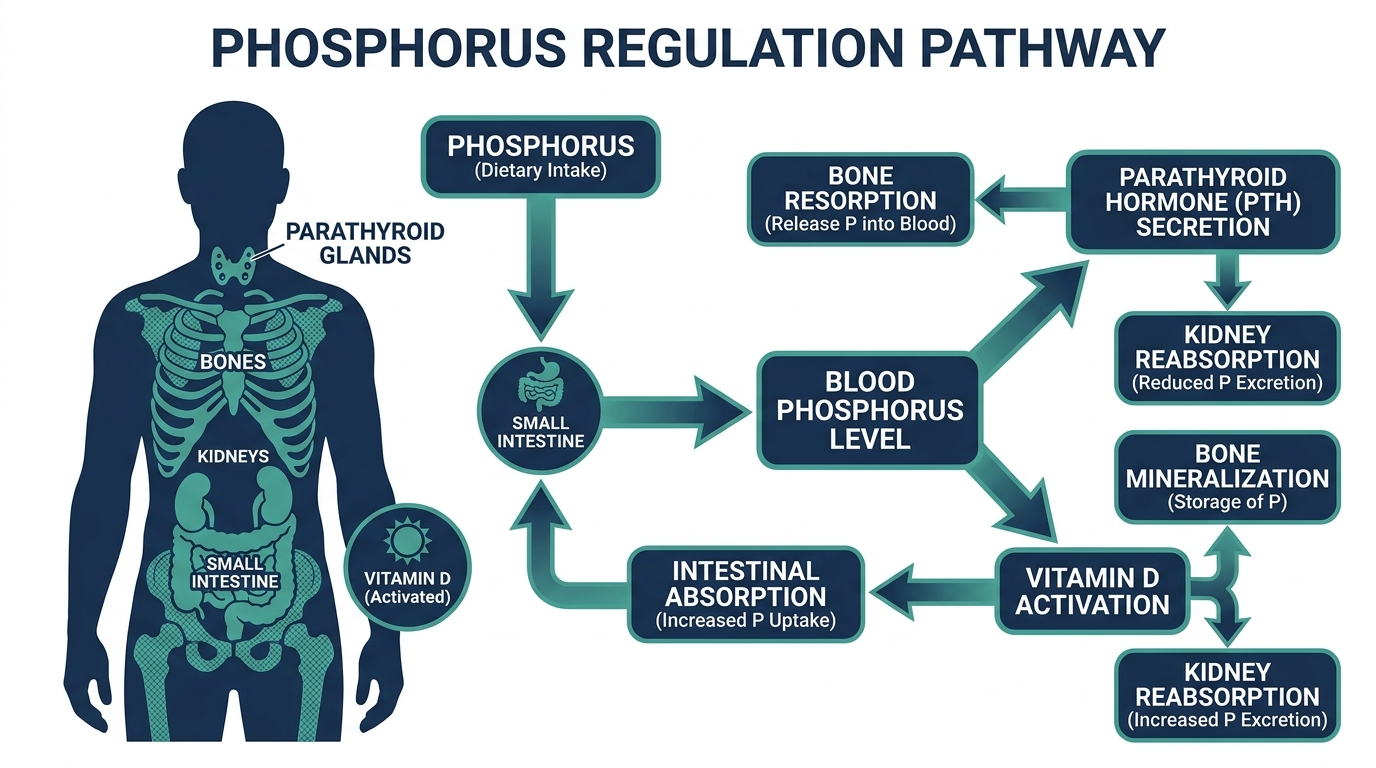
Because phosphate is spread across energy, bone, genetics, and cell structure, its level is tightly regulated. That regulation is exactly why a blood value shifts when the kidney, parathyroid, or nutrition status is disturbed, and why the number is read as a clue to those systems rather than a standalone figure.

How calcium and phosphate move together
The single most useful concept for reading a phosphorus result is its relationship with calcium. The two minerals are managed as a linked pair, and they often move in opposite directions. When one rises, the body tends to push the other down, coordinated by parathyroid hormone (PTH) and vitamin D (Cleveland Clinic).
Here is the practical version. PTH lowers blood phosphate by making the kidneys excrete more of it, while raising calcium. Active vitamin D raises absorption of both minerals from the gut. In health these signals balance. When they fail, characteristic patterns appear:
- High phosphate with low calcium and high PTH: the classic picture of advanced kidney disease, called secondary hyperparathyroidism.
- High phosphate with low calcium and low PTH: points toward hypoparathyroidism, where missing PTH lets phosphate build up.
- Low phosphate with high calcium and high PTH: suggests overactive parathyroid glands (primary hyperparathyroidism) driving phosphate out.
This is why a phosphorus value alone is hard to act on. Read with calcium and PTH, it becomes a precise diagnostic signal.
Dietary phosphorus and why the source matters
Phosphorus is abundant in food, so a low level almost never comes from diet alone in a healthy person, and a high level in kidney disease is heavily shaped by which kind of phosphorus you eat. There are three practical categories.
| Source type | Examples | How well it is absorbed |
|---|---|---|
| Organic, animal | Meat, poultry, fish, dairy, eggs | Moderately to well absorbed. |
| Organic, plant | Beans, nuts, whole grains, seeds | Less well absorbed, because much is bound as phytate that humans digest poorly. |
| Inorganic additives | Processed foods, colas, packaged meats (ingredients with “phos”) | Very efficiently absorbed, often 90 percent or more. |
The takeaway that matters for anyone limiting phosphorus is that the additive phosphate in processed foods is absorbed far more completely than the natural phosphorus in beans or whole grains. Scanning ingredient lists for words containing “phos,” such as phosphoric acid or sodium phosphate, is often more effective than counting total milligrams. For a healthy person, none of this causes a high blood level, because working kidneys clear the excess easily.
Refeeding syndrome: a key reason phosphate drops
One of the most important causes of a dangerously low phosphorus is refeeding syndrome, and it deserves its own explanation because it is both serious and often missed. It happens when nutrition is restarted, too quickly, in someone who has been starved or severely malnourished, such as after prolonged fasting, anorexia, or major illness.
The mechanism is a rapid shift, not a true shortage of body phosphorus. When carbohydrate hits the bloodstream after starvation, insulin surges and drives glucose, potassium, magnesium, and phosphate rapidly into cells. Blood phosphate can plummet within days of feeding, and because phosphate powers the energy the body needs to handle the new fuel, a sudden drop can cause muscle weakness, breathing failure, heart rhythm problems, and confusion. This is why people at risk are refed slowly, with phosphate, potassium, and magnesium monitored and replaced. If you or a family member is recovering from severe undernutrition, this is the reason clinicians watch phosphate so closely in the first days.

Reading real phosphorus result combinations
The same phosphorus value can mean very different things depending on context. These are the patterns to recognize.
- High phosphate, low eGFR: reduced kidney clearance, the most common cause of a high result.
- High phosphate, normal kidneys, feeling fine: often a timing effect, a non-fasting draw, or hemolysis. A repeat fasting morning sample frequently normalizes.
- Low phosphate after restarting nutrition: a red flag for refeeding syndrome that needs prompt attention.
- Low phosphate with high calcium: points toward overactive parathyroid glands.
- Low phosphate with heavy alcohol use: a common and often overlooked cause through poor intake and cellular shifts.
In every case the phosphorus number is the opening question, and the kidney, calcium, and nutritional context supplies the answer.
Preparing for the test and avoiding false readings
Phosphorus is easily distorted, so a few precautions prevent a false alarm.
- Fast and draw in the morning. Phosphate follows a daily rhythm, dipping in the morning and rising later, and a recent carbohydrate meal can pull it into cells and lower the reading. A fasting morning sample gives the cleanest comparison over time (MedlinePlus).
- Watch for hemolysis. If red cells rupture during a difficult draw or delayed handling, they leak phosphate and falsely raise the result. A note of hemolysis is a reason to repeat.
- Report medicines and supplements. Phosphate-containing laxatives, vitamin D, antacids that bind phosphate, and some intravenous treatments can move the number in either direction.
If phosphorus is your only abnormal value and you feel well, the right response is a repeat fasting draw and a look at the trend alongside calcium and kidney function, not an immediate conclusion.
Common misconceptions about a phosphorus result
Several beliefs about phosphorus lead people to worry about the wrong things.
- “An abnormal phosphorus means I ate wrong.” In a healthy person, diet rarely moves the blood level much, because the kidneys handle the excess. Persistent abnormality usually involves the kidney, parathyroid, or nutrition.
- “A child’s high phosphorus is a problem.” Children normally run higher than adults because of bone growth, so a value must be read against the age-specific range.
- “All food phosphorus is the same.” It is not. Additive phosphate is absorbed far more efficiently than the phosphorus in beans and grains.
- “One reading is a diagnosis.” Timing, a non-fasting draw, or hemolysis can each create a falsely abnormal value. A single result is a prompt to repeat, not a verdict.
Seeing these clearly helps you respond to a phosphorus result with context rather than alarm.
How phosphorus imbalances are corrected
Treatment always follows the cause, and the two directions call for very different approaches.
- For high phosphorus: the focus in kidney disease is limiting absorbed phosphate. That means cutting inorganic phosphate additives in processed foods first, and using phosphate binders taken with meals so they trap phosphate in the gut before it is absorbed. Binders only work when taken with food, a detail people often get wrong (National Kidney Foundation).
- For low phosphorus: mild cases are corrected by treating the underlying cause, such as reducing alcohol or fixing malnutrition. Severe or symptomatic cases are replaced carefully, sometimes intravenously, with the level rechecked often to avoid overshooting into a high value.
In both directions, the number is corrected by addressing the reason behind it, whether that is kidney clearance, parathyroid activity, or nutrition. Chasing the value without the cause rarely works.
Who should have phosphorus checked
Phosphorus is not part of every routine screen, so it helps to know who benefits from having it measured.
- People with chronic kidney disease, in whom it is monitored routinely as function declines.
- Anyone on dialysis, where phosphate control directly affects heart and vessel health.
- People with parathyroid or vitamin D disorders, where it is read with calcium and PTH.
- Those recovering from severe malnutrition or starvation, to catch refeeding-related drops.
- People with heavy alcohol use or conditions that impair absorption.
For a healthy adult with normal kidneys, an isolated abnormal phosphorus on a routine panel is most often a timing or collection effect, and a careful repeat is the right first move. The value carries the most weight when read with kidney function, calcium, and a trend over time rather than as a single figure.
Phosphorus ranges by age and life stage
The normal range for phosphorus is not the same at every age, which is a frequent source of confusion when a parent sees a child’s result.
- Adults: roughly 2.5 to 4.5 mg/dL (Cleveland Clinic).
- Children and teenagers: normally higher, often up to about 4.5 to 6.5 mg/dL, because growing bones actively pull in phosphate (MedlinePlus). A value that would be high for an adult can be perfectly normal for a growing child.
- Infants: higher still, reflecting rapid bone growth.
This is why the reference range printed on the report is set for the person’s age. Comparing a child’s phosphorus to an adult range, or the reverse, is a common mistake that leads to needless worry. Always read the value against the range provided for that individual.
Phosphorus in chronic kidney disease: why the target changes
Chronic kidney disease is the single most common reason a phosphorus result matters over a lifetime, and it is where interpretation shifts the most. Healthy kidneys clear excess phosphate through urine with room to spare. As kidney function declines, that clearance falls, phosphate begins to accumulate, and the level on a report starts to climb even when nothing about the diet has changed. This is why nephrologists watch phosphorus closely in anyone with reduced kidney function, often long before the number leaves the standard reference range.
The guidance from kidney specialists is to keep serum phosphate near the normal range in advanced kidney disease and dialysis, because persistently high levels drive the calcium and phosphate deposits that stiffen blood vessels and strain bone over time. In practice this target is hard to hit. Research on hemodialysis patients has found that a large majority struggle to hold phosphorus below the recommended threshold across several months, which tells you how much daily effort control takes (Patient education for phosphorus management in CKD).
Management leans on three levers working together. More effective dialysis removes phosphate mechanically. A lower phosphorus diet limits the load coming in, with special attention to the inorganic phosphate additives in processed foods, which absorb far more completely than the phosphorus bound up in whole foods. And phosphate binders, taken with meals, trap dietary phosphate in the gut so less reaches the blood. If you or a family member has kidney disease, this is the context that turns a phosphorus number from a passing lab value into a figure worth tracking at every visit.
Curious where your phosphorus really sits?
Baseline phosphorus and 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
What is a normal phosphorus level in a blood test?
For adults, a normal serum phosphorus level is roughly 2.5 to 4.5 mg/dL, according to Cleveland Clinic. Children normally run higher because of bone growth. Exact cutoffs vary by laboratory, so check the reference range printed on your own report.
Do I need to fast before a phosphorus blood test?
Often yes. Many clinicians ask for a fasting morning sample because recent meals, especially carbohydrates, can temporarily lower phosphate by shifting it into cells. Always follow the specific instructions your ordering provider or lab gives you.
Is high phosphorus dangerous?
It can be, mainly in kidney disease. Persistently high phosphorus pulls calcium from bones and can deposit calcium in blood vessels, raising cardiovascular risk. That is why kidney patients manage it with diet and phosphate binders, per the National Kidney Foundation.
What foods are high in phosphorus?
Dairy products, meat, poultry, fish, nuts, beans, and whole grains are naturally high in phosphorus. Processed foods and many sodas contain added phosphate that the body absorbs easily, which is why kidney patients are often told to limit them.
Can low phosphorus be serious?
Mild low phosphorus is often harmless and silent. Severe hypophosphatemia, below about 2.5 mg/dL and dropping further, can cause muscle weakness, confusion, and in extreme cases breathing or heart problems, so it is treated promptly under medical supervision (Cleveland Clinic).
Sources
- Cleveland Clinic, Hyperphosphatemia
- Cleveland Clinic, Hypophosphatemia
- MedlinePlus, Phosphate in Blood
- MSD Manual Professional, Hyperphosphatemia
- NIH PMC, Hyperphosphatemia of Chronic Kidney Disease
- National Kidney Foundation, High Phosphorus
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


