
Low phosphorus sits at the edge of a narrow normal range, so where does your number actually land? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
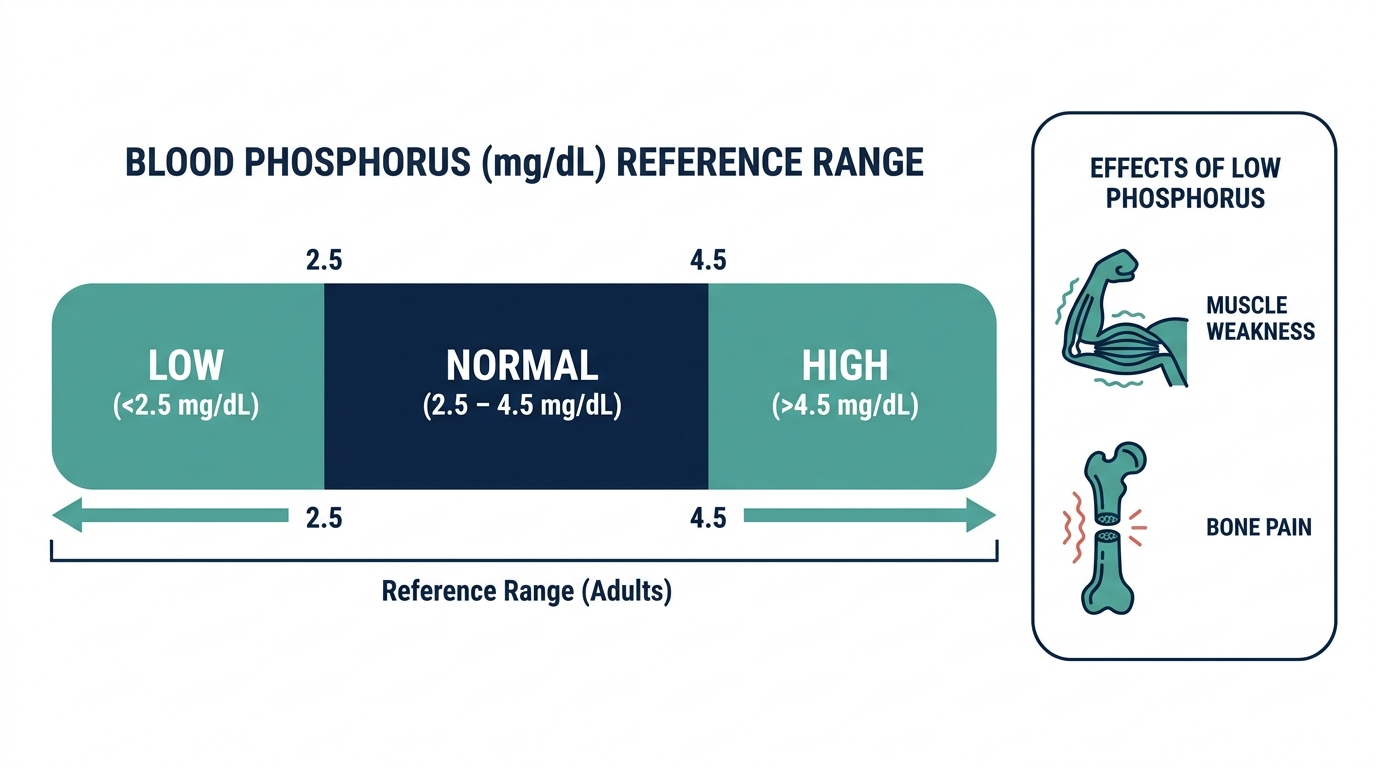
- Low phosphorus on a blood test (hypophosphatemia) means your serum phosphate is below 2.5 mg/dL, which is the lower edge of the normal adult range of 2.5 to 4.5 mg/dL reported by Cleveland Clinic and StatPearls.
- Most mild and moderate low phosphorus results (1.5 to 2.5 mg/dL) cause no symptoms at all, and common triggers include alcohol use, refeeding after malnutrition, and recovery from diabetic ketoacidosis.
- Low phosphorus becomes dangerous when it falls below 1.0 mg/dL, when it can cause severe muscle weakness, confusion, seizures, and breathing or heart problems that need urgent care.
If your lab report flagged a low phosphorus (phosphate) value, you are probably wondering whether it is a minor blip or a real problem. The short answer is that it depends on how far below the normal range you fell and why. This guide explains what the number means, what tends to cause it, and when low phosphorus is worth acting on quickly.
What does low phosphorus mean and what is the cutoff?
Low phosphorus, called hypophosphatemia, means your serum phosphate level is below 2.5 mg/dL, the lower limit of the normal adult range of 2.5 to 4.5 mg/dL (Cleveland Clinic; StatPearls). Children normally run higher, at roughly 4.5 to 6.5 mg/dL, because they are actively building bone.
Phosphorus is a mineral your body uses to build bone and teeth, store and release energy through a molecule called ATP, and keep cell membranes working. Most of it lives in your skeleton, and only a small fraction circulates in blood, which is what the test measures. Because that blood pool is small and shifts quickly, a single low reading does not always mean your total body stores are depleted. Clinicians group results into ranges to gauge concern:
- Mild to moderate (1.5 to 2.5 mg/dL): Often no symptoms, frequently temporary (StatPearls).
- Severe (below 1.5 mg/dL): Can cause muscle, nerve, and organ problems.
- Critical (below 1.0 mg/dL): Serious symptoms become likely and prompt treatment is needed.

What causes low phosphorus?
Low phosphorus usually comes from one of three mechanisms: too little going in, too much leaving through the kidneys or gut, or phosphate shifting out of the blood and into cells (StatPearls). That last mechanism, an internal shift, is the most common cause of a sudden drop and explains why the blood number can fall even when total body phosphate is normal.
Frequently seen triggers include:
- Alcohol use disorder: One of the most common causes in hospitalized adults, through poor intake and increased urinary loss (Cleveland Clinic).
- Refeeding syndrome: When eating restarts after malnutrition or fasting, a surge of insulin pulls phosphate into cells.
- Recovery from diabetic ketoacidosis: Insulin treatment drives phosphate into cells.
- Severe burns or respiratory alkalosis: Often from hyperventilation, which shifts phosphate inward.
- Long-term issues: Vitamin D deficiency, overactive parathyroid glands, malabsorption, certain IV iron products, diuretics, and phosphate-binding antacids (Cleveland Clinic).
What are the symptoms, or is it silent?
Most mild and moderate low phosphorus results are silent. Patients with levels of 1.5 to 2.5 mg/dL are generally asymptomatic, and symptoms typically appear only once levels drop well below that, especially under 1.0 mg/dL (StatPearls). This is why low phosphorus is often discovered by accident on routine bloodwork rather than because someone felt unwell.
When symptoms do occur, they stem from cells running short on energy because phosphate is needed to make ATP. Possible signs include:
- Muscle problems: Weakness, muscle pain, and in severe cases muscle breakdown (rhabdomyolysis).
- Bone symptoms: Bone pain, and over time softened or weakened bone with chronic deficiency.
- Nervous system: Confusion, irritability, numbness, weak reflexes, and in extreme cases seizures.
- Heart and lungs: Severe deficiency can weaken the heart muscle and the diaphragm, affecting breathing (Cleveland Clinic).
When is low phosphorus dangerous?
Low phosphorus becomes dangerous when it drops below 1.0 mg/dL, the level at which serious clinical symptoms become likely (StatPearls). At that depth, the consequences can include metabolic encephalopathy, rhabdomyolysis, weakening of the heart muscle, and respiratory failure from a fatigued diaphragm.
Severe acute drops are the most worrying. When phosphate falls very rapidly to extremely low levels, people can develop disorientation, seizures, focal neurological changes, and heart failure. The speed of the fall matters as much as the absolute number, which is why a quickly dropping value in a hospitalized patient gets urgent attention even before symptoms appear. Context also raises the stakes: someone being refed after starvation, recovering from diabetic ketoacidosis, or withdrawing from alcohol can crash quickly, so these situations are monitored closely. If you have a known low phosphorus result alongside new confusion, severe weakness, trouble breathing, or a seizure, treat it as an emergency.

What should you do next and when should you see a doctor?
For a mild low phosphorus result with no symptoms, the next step is usually a recheck rather than treatment, because many cases are temporary and self-correct (Cleveland Clinic). Your clinician will look at the trend and the likely cause before deciding anything.
Practical steps to discuss with your provider:
- Ask why: The cause guides everything. Mention alcohol use, recent dieting or fasting, antacid or diuretic use, and IV iron.
- Check related labs: Calcium, magnesium, vitamin D, and kidney function often need to be reviewed together.
- Repeat the test: A single value, especially if drawn after a meal or fasting, may not reflect your true status.
- Replacement when needed: Mild to moderate cases are treated with oral phosphate or diet, while severe cases need IV phosphate, usually in a hospital (Cleveland Clinic).
See a doctor promptly for a level under 1.5 mg/dL, or sooner if you have muscle weakness, confusion, or breathing problems. Go to emergency care for a known very low level with seizures, severe confusion, or breathing difficulty.
Insider nuance: timing and diet can fake a low result
Phosphate levels follow a daily rhythm and respond fast to food, so a low reading is sometimes a timing artifact rather than true depletion. Serum phosphate is lowest in the morning and after carbohydrate-rich meals, because both insulin release and the body clock push phosphate into cells (StatPearls).
This matters in two ways. First, a borderline low value drawn after breakfast or a sugary drink may simply reflect a temporary internal shift, which is why clinicians often repeat the test, sometimes fasting, before acting. Second, a normal blood number does not guarantee normal stores, because the circulating pool is tiny compared with what is locked in bone. The opposite is also true: aggressive carbohydrate or glucose infusions can drop the number quickly. The takeaway is to interpret one phosphorus value in context, including when blood was drawn, what you recently ate, and the clinical situation, rather than treating a single figure as the whole story.
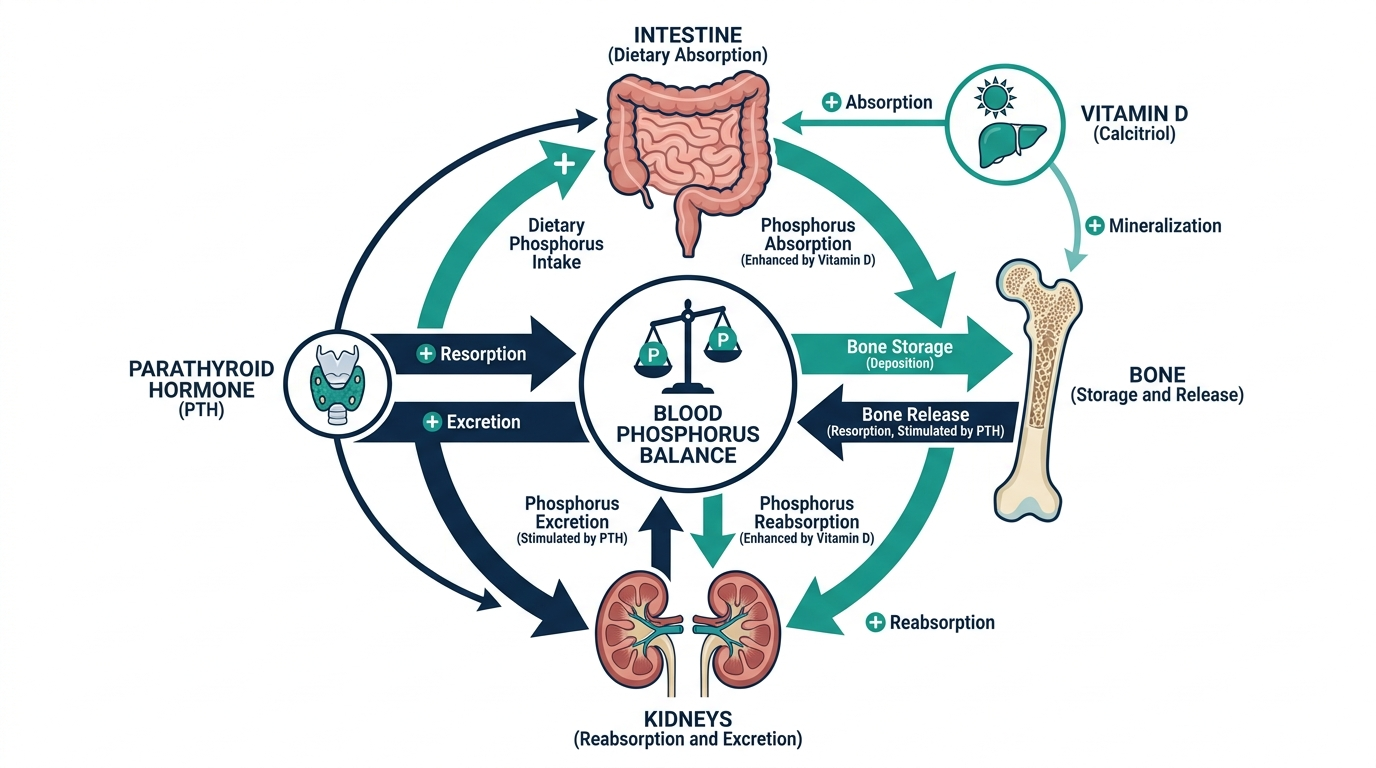
How your body regulates phosphorus
Low phosphorus makes more sense once you see the system that normally keeps it steady. Phosphate is controlled by a tight interplay between the gut, the kidneys, bone, and three key hormones, and a disturbance anywhere in that loop can drop the blood level.
- Parathyroid hormone (PTH): when PTH rises, it tells the kidneys to dump more phosphate into the urine. An overactive parathyroid gland can therefore push phosphorus low.
- Vitamin D (active form, calcitriol): it increases phosphate absorption from the gut, so vitamin D deficiency reduces how much phosphate you take in from food.
- FGF23: a hormone made by bone that lowers phosphate by increasing urinary loss. Some rare inherited and tumor-related conditions raise FGF23 and cause stubborn phosphate wasting.
- The kidneys: the main gatekeeper, reclaiming or excreting phosphate to hold the balance. When kidney handling is disrupted, phosphate can spill into the urine.
This is why phosphorus is so often interpreted alongside calcium, vitamin D, PTH, and kidney function. A low phosphate rarely travels alone; the surrounding hormones usually reveal whether the loss is from the gut, the kidney, or a shift into cells.

Refeeding syndrome: the most important cause to understand
Of all the causes of low phosphorus, refeeding syndrome deserves special attention because it is common, predictable, and dangerous, yet often preventable. It happens when nutrition is restarted, especially with carbohydrates, after a period of starvation, prolonged fasting, severe illness, alcohol use disorder, or an eating disorder.
The mechanism is a rapid metabolic switch. During starvation the body runs low on phosphate stores even if the blood level looked normal. When food, particularly carbohydrate, arrives, insulin surges and drives glucose, phosphate, potassium, and magnesium out of the blood and into cells all at once. The blood phosphate can then plummet within a day or two, sometimes to dangerous levels, causing muscle weakness, heart strain, breathing problems, and confusion.
The people at highest risk include those with little or no intake for many days, very low body weight, significant recent weight loss, chronic alcohol use, or a history of an eating disorder. In hospitals, this is why nutrition is often reintroduced slowly, with phosphate, potassium, and magnesium checked frequently and replaced before and during refeeding. The practical lesson for anyone recovering from a long period of poor eating is that starting to eat again is not automatically safe; it should be done gradually and, in high-risk cases, under medical supervision.
The markers read alongside phosphorus
A phosphate result becomes far more useful when read with its usual companions, because the pattern points to the cause.
| Marker | What it reveals |
|---|---|
| Calcium | Calcium and phosphate move in a linked, often opposite, relationship. Low phosphate with high calcium can suggest an overactive parathyroid. |
| PTH | High PTH drives phosphate into the urine; checking it helps separate a parathyroid cause from other reasons. |
| Vitamin D (25-OH) | Deficiency reduces phosphate absorption from the gut, a common and correctable contributor. |
| Magnesium and potassium | These often fall together with phosphate in refeeding, alcohol use, and diarrhea, so they are checked as a group. |
| Creatinine and eGFR | Kidney function shapes how phosphate is handled and guides safe replacement dosing. |
| Urine phosphate | Measuring phosphate in the urine separates renal wasting (high urine phosphate) from an internal shift or poor intake (low urine phosphate). |
The urine phosphate test is a particularly powerful tie-breaker. If the blood is low but the kidneys are still spilling phosphate into the urine, the problem is renal wasting; if the urine phosphate is appropriately low, the body is holding on and the loss is from intake or a shift into cells.
Dietary phosphorus and who is at risk of running low
Phosphorus is abundant in the food supply, which is why poor intake alone rarely causes deficiency in someone eating normally. It is found in dairy, meat, fish, eggs, nuts, beans, and whole grains, and it is added to many processed foods and colas as a preservative. For most people, the diet delivers plenty.
Deficiency instead clusters in specific situations where intake, absorption, or handling breaks down:
- Chronic alcohol use: combines poor intake, vomiting, diarrhea, and increased urinary loss, making it one of the leading causes in hospitalized adults.
- Malnutrition and eating disorders: depleted stores plus refeeding risk.
- Malabsorption: conditions such as chronic diarrhea, celiac disease, or after certain gastrointestinal surgeries reduce absorption.
- Overuse of phosphate-binding antacids: aluminum-, calcium-, or magnesium-based binders taken frequently can block phosphate absorption.
- Certain medications and treatments: some diuretics, certain intravenous iron products, and recovery from diabetic ketoacidosis can all lower phosphate.
Recognizing which of these applies to you is the single most useful thing you can bring to the conversation with your clinician, because the cause dictates whether the fix is dietary, a change in medication, or something that needs closer monitoring.

How replacement is handled
Treatment of low phosphorus is guided by how low the level is, whether you have symptoms, and what caused it, rather than by the number alone. The approach ranges from doing very little to intensive hospital care.
- Mild, no symptoms: often no active treatment beyond a recheck and addressing the cause, since many cases self-correct once the trigger passes.
- Mild to moderate: oral phosphate supplements and phosphate-rich foods such as dairy and milk. A common practical tip clinicians use is that milk is an inexpensive, well-tolerated phosphate source.
- Severe or symptomatic (generally below 1.0 mg/dL): intravenous phosphate given carefully in a hospital, because replacing too fast can drop calcium and cause other electrolyte problems.
- Underlying cause: equally important, whether that means treating vitamin D deficiency, stopping a phosphate-binding antacid, slowing a refeed, or managing an overactive parathyroid.
Because aggressive replacement carries its own risks, especially in kidney disease, phosphate is one of the electrolytes where slow and monitored correction is the rule, not the exception.
Preparing for the test and getting a reliable result
Because phosphate shifts so quickly with food and the time of day, how and when your blood is drawn has a real effect on the number. Getting a trustworthy result comes down to a few practical points you can raise with the lab or your clinician.
- Timing: serum phosphate is naturally lowest in the morning and tends to be higher later in the day. A borderline value drawn first thing may read lower than the same person would show in the afternoon.
- Recent meals: a carbohydrate-rich meal or sugary drink triggers insulin, which pushes phosphate into cells and can transiently lower the blood level. Many clinicians prefer a fasting or consistently timed draw when the result is borderline.
- Sample handling: phosphate can rise falsely if red blood cells break during a difficult draw or if the sample sits too long before processing, so an unexpectedly abnormal value is sometimes rechecked.
- Medications and supplements: phosphate-binding antacids, some diuretics, vitamin D, and recent IV iron all influence the result, so a current medication list helps interpret it.
The single most useful habit is consistency. Comparing values drawn at similar times of day, under similar conditions, gives your clinician a far cleaner trend than isolated readings taken whenever was convenient. When a result surprises everyone, a repeat under controlled conditions is usually the smartest next step before any treatment decision.
Common misconceptions about low phosphorus
A few misunderstandings can make a low phosphorus result more alarming or more confusing than it needs to be.
- “A low blood level means my body is badly depleted.” Not necessarily. Only a small fraction of phosphate circulates in blood, so a low reading can reflect a temporary shift into cells rather than true whole-body depletion.
- “I just need to eat more phosphorus-rich food.” Diet helps in mild cases, but if the cause is renal wasting, an internal shift, or a medication, food alone will not fix it.
- “Starting to eat normally again after not eating is always safe.” Refeeding after prolonged starvation can crash phosphate dangerously; high-risk people need a slow, monitored reintroduction.
- “One low value means I need treatment.” A borderline reading drawn after a carbohydrate meal may simply reflect the daily rhythm and often warrants a repeat test before any action.
- “Phosphorus problems are always about the kidneys.” Hormones, vitamin D, alcohol, and internal shifts are frequently the real drivers, which is why the full pattern matters.
How the picture differs by age and situation
A phosphorus value that looks low on paper does not carry the same weight for everyone, because normal physiology and typical causes shift across life stages and circumstances.
- Infants and children: healthy children normally run higher than adults, roughly 4.5 to 6.5 mg/dL, because growing bone constantly pulls phosphate from the blood. A value that would be flagged as high in an adult can be perfectly normal in a toddler, so pediatric results are read against age-specific ranges.
- Older adults: the causes here often cluster around medications and nutrition. Long-term antacid use, diuretics, poor appetite, and reduced vitamin D from limited sun exposure are common contributors, and several of these can stack together quietly.
- Hospitalized and critically ill patients: this is where the sharpest, most dangerous drops appear, driven by refeeding, insulin treatment for high blood sugar, and recovery from alcohol withdrawal. Phosphate is watched closely in these settings precisely because it can fall fast.
- Endurance athletes and heavy exercisers: intense or prolonged exertion, along with hyperventilation and large carbohydrate loads around training, can shift phosphate into cells and produce a transient dip that resolves with rest and normal eating.
The practical point is that context changes the meaning of the same number. A borderline reading in a healthy young adult after a big carbohydrate meal is usually nothing, while the same value in someone being refed after weeks of poor intake is a signal to act. When you discuss a low result, telling your clinician your age, medications, recent eating pattern, and activity level does more to clarify the picture than the digit on the report by itself.
Don’t just read about phosphorus, track it.
A single result is a snapshot. Superpower re-tests phosphorus and 100+ markers over time so you can watch them move as you change sleep, food, and training.
Frequently asked questions
Is low phosphorus serious?
It depends on how low. Mild results of 1.5 to 2.5 mg/dL are often harmless and temporary. It becomes serious below 1.0 mg/dL, when muscle weakness, confusion, seizures, and breathing or heart problems can develop and prompt treatment is needed (StatPearls).
What is the normal range for phosphorus in a blood test?
The normal adult range is 2.5 to 4.5 mg/dL, according to Cleveland Clinic and StatPearls. Children normally run higher, around 4.5 to 6.5 mg/dL. Ranges vary slightly between labs, so check your own report and ask your clinician what is normal for you.
What is the most common cause of low phosphorus?
An internal shift of phosphate from blood into cells is the most common cause of a sudden drop, often from insulin surges. Frequent specific triggers include alcohol use disorder, refeeding after malnutrition, and recovery from diabetic ketoacidosis (StatPearls; Cleveland Clinic).
Can diet cause low phosphorus?
Poor intake alone rarely causes it, because phosphorus is common in food. Diet matters more through refeeding after starvation, heavy alcohol use, and overuse of phosphate-binding antacids, which block absorption. A carbohydrate-rich meal can also temporarily lower the blood number (Cleveland Clinic).
How is low phosphorus treated?
Mild cases often need only a recheck or oral phosphate and dietary changes, since many resolve on their own. Severe cases, generally below 1.0 mg/dL or with symptoms, are treated with intravenous phosphate, usually in a hospital. Treatment also targets the underlying cause (Cleveland Clinic).
Sources
- Cleveland Clinic, Hypophosphatemia: Causes, Symptoms and Treatment
- StatPearls (NCBI Bookshelf), Hypophosphatemia
- Merck Manual Consumer Version, Hypophosphatemia
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


