
High phosphorus has several common causes, so do you know what’s actually driving yours up? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
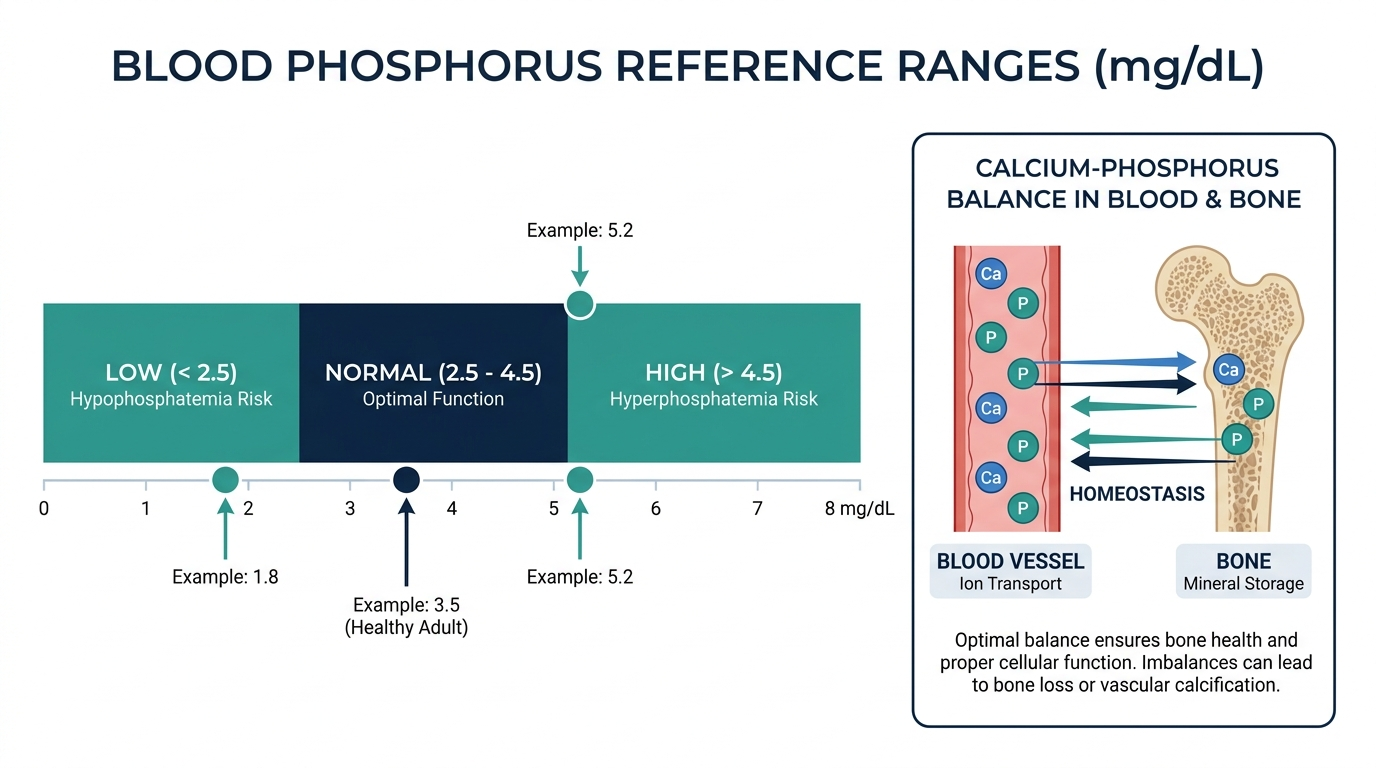
- A high phosphorus blood test, called hyperphosphatemia, means your serum phosphate is above 4.5 mg/dL, since the normal adult range is 2.5 to 4.5 mg/dL (StatPearls, NCBI).
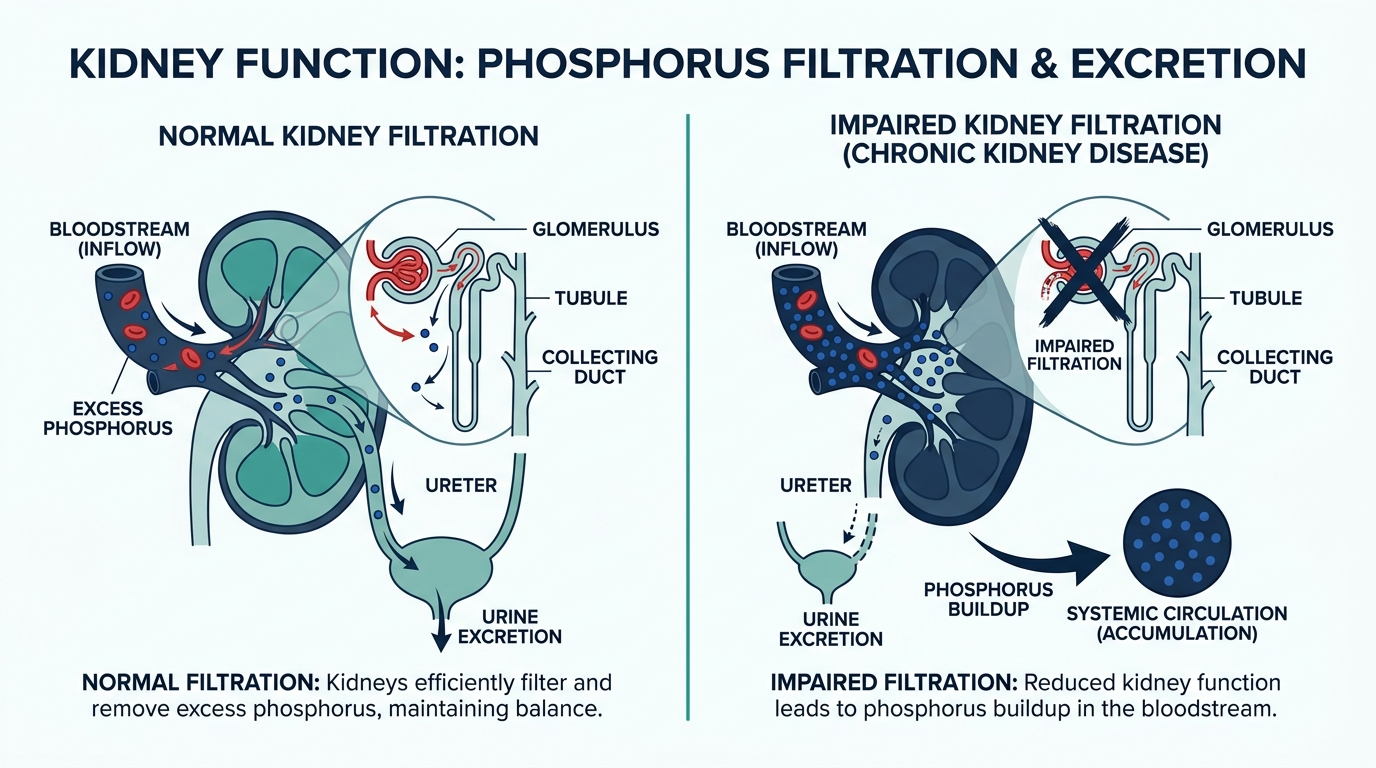
- The most common cause of high phosphorus is reduced kidney clearance, which becomes significant once kidney filtration drops below a GFR of 30 mL/min (StatPearls, NCBI).
- Most people with mildly high phosphorus feel nothing, but levels that stay high for years can drive blood vessel calcification, seen on CT in more than 80% of dialysis patients (StatPearls, NCBI).
What a high phosphorus result means and the cutoff
A high phosphorus result means your blood phosphate sits above the upper normal limit of 4.5 mg/dL. The reference range for adults is 2.5 to 4.5 mg/dL, and anything above that line is called hyperphosphatemia (Cleveland Clinic; StatPearls, NCBI). Children naturally run higher, with a normal range of roughly 4 to 7 mg/dL because growing bones use more phosphate.
Phosphorus is a mineral your body stores mostly in bones and teeth, with a small amount circulating in blood where it helps make energy, build cell membranes, and balance calcium. Because your kidneys are the main exit route for excess phosphate, a single high value is often rechecked. One borderline reading does not equal a diagnosis. Your clinician looks at the trend, your kidney function, and your calcium together before deciding it is real and meaningful.

What causes high phosphorus
The leading cause of high phosphorus is the kidneys clearing too little of it, which happens in chronic kidney disease and is most pronounced once filtration falls below a GFR of 30 mL/min (StatPearls, NCBI). High serum phosphate usually appears only in the later stages of kidney disease, which is why it is a red flag worth investigating.
Other recognized causes include:
- Decreased excretion: chronic kidney disease, acute kidney injury, and hypoparathyroidism, in which low parathyroid hormone lets phosphate build up (Cleveland Clinic).
- Increased intake or absorption: phosphate-containing laxatives or enemas, and vitamin D intoxication, which boosts intestinal absorption of phosphate (StatPearls, NCBI).
- Cell breakdown and shifts: conditions like diabetic ketoacidosis, lactic acidosis, tumor lysis, or muscle injury that release phosphate from inside cells.
- Pseudohyperphosphatemia: a lab artifact, not a real elevation, caused by high blood lipids, high globulins, or high bilirubin interfering with the assay (StatPearls, NCBI).
Symptoms, or why it is often silent
High phosphorus itself usually causes no symptoms. Most people with elevated phosphate feel completely normal and only learn about it from routine bloodwork (National Kidney Foundation; StatPearls, NCBI). That silence is exactly why it slips by for so long.
When symptoms do appear, they typically come from the falling calcium that high phosphate can trigger, not from the phosphate directly. Low calcium can cause muscle cramps, tingling around the mouth or in the fingers, twitching, and in severe cases tetany or seizures (StatPearls, NCBI). Over the long term, calcium and phosphate can deposit in soft tissues and skin, sometimes causing itching or, rarely, painful firm lumps near joints. If you notice persistent muscle cramping, numbness, or unexplained itching alongside a high phosphorus result, mention it to your clinician.
When high phosphorus is dangerous
High phosphorus becomes dangerous when it stays elevated for years, because it accelerates calcification of blood vessels and the heart. Vascular calcification is found on CT imaging in more than 80% of dialysis patients, and it links to systolic hypertension, a widened pulse pressure, and left ventricular hypertrophy (StatPearls, NCBI).
The acute danger is different. A sudden, very high phosphate spike, for example from a phosphate enema or tumor lysis, can crash your calcium fast enough to cause heart rhythm problems, seizures, or kidney damage, which is a medical emergency (StatPearls, NCBI). Chronic mild elevation is a slow cardiovascular risk that needs steady management, while a rapid severe spike with symptoms needs same-day care. Knowing which situation you are in shapes how urgently it must be addressed.

What to do next and when to see a doctor
The first step is to confirm the result and check your kidneys, because high phosphorus rarely travels alone. Your clinician will usually repeat the test and order kidney function (creatinine and GFR), calcium, and often parathyroid hormone to find the cause (Cleveland Clinic). Treatment targets that cause rather than the number itself.
Common next steps include reducing phosphate-heavy processed foods and additives, adjusting or stopping phosphate-containing supplements or laxatives, and, in kidney disease, using phosphate binders taken with meals (National Kidney Foundation). See a doctor promptly if your phosphorus is high and you have known kidney disease, or if it comes with muscle cramps, numbness, or twitching. Seek urgent care for severe symptoms such as seizures, fainting, or an irregular heartbeat after a phosphate enema or laxative.
Insider nuance: the calcium-phosphate product and food labels
Clinicians rarely look at phosphorus alone. They watch the calcium-phosphate product, calcium multiplied by phosphate, because a high combined value is what drives mineral deposits into arteries and soft tissue (StatPearls, NCBI). A phosphate of 5.5 with high calcium is treated more aggressively than the same phosphate with low calcium.
A second practical point: not all dietary phosphorus behaves the same. The inorganic phosphate added to processed foods, colas, and packaged meats is absorbed far more efficiently than the natural phosphorus in beans or dairy, so cutting additives often lowers blood phosphate more than counting milligrams from whole foods (National Kidney Foundation). Scan ingredient lists for words containing “phos,” such as phosphoric acid or sodium phosphate. That label habit is one of the highest-yield changes for anyone managing this result.
How your body keeps phosphate in range
Phosphate is not left to drift. Three hormones hold it inside a narrow band, and understanding them explains why a high result rarely means one simple thing. The three regulators are parathyroid hormone (PTH), active vitamin D, and fibroblast growth factor 23 (FGF23), a hormone made by bone cells called osteocytes (Regulation of Phosphate Homeostasis by PTH, Vitamin D, and FGF23, PMC).
Here is how the loop works in plain terms. When blood phosphate rises, bone releases more FGF23. FGF23 travels to the kidney and tells it to dump phosphate into the urine, and at the same time it lowers active vitamin D so your gut absorbs less phosphate from food. PTH also pushes phosphate out through the urine. Active vitamin D does the opposite, raising absorption in the gut. In a healthy person these signals cancel out and phosphate stays put.
This matters for reading your result because a high phosphorus almost always means the kidney arm of that system has stalled. When kidney filtration drops, the FGF23 and PTH signals can no longer force enough phosphate into the urine, so it backs up in the blood. That is why a phosphorus value is never interpreted alone. It is read as a window into how well the kidney and its hormones are coping.

The panel phosphorus is read with, and why
Phosphorus almost never appears on a lab report by itself. It rides on a metabolic or renal panel, and the surrounding numbers change its meaning completely. These are the values a clinician scans next to it and what each one adds.
| Marker read with phosphorus | Why it changes the interpretation |
|---|---|
| Creatinine and eGFR | Estimate kidney filtration. High phosphorus with a low eGFR points straight at reduced kidney clearance, the most common cause. |
| Calcium | Phosphate and calcium move in a linked pair. High phosphate often pulls calcium down, and the combined load is what damages arteries. |
| Parathyroid hormone (PTH) | Low PTH (hypoparathyroidism) lets phosphate build up. High PTH is the body fighting back against retained phosphate in kidney disease. |
| Vitamin D (25-OH) | Vitamin D excess raises gut absorption of phosphate. Very low vitamin D shifts calcium and PTH, indirectly moving phosphate. |
| Magnesium | Often disturbed alongside phosphate in kidney disease and in refeeding, and it affects PTH activity. |
The single most useful companion is kidney function. If your eGFR is normal and your phosphorus is only slightly high, the story is usually benign, often a timing or diet effect. If your eGFR is falling, a high phosphorus becomes a marker to act on.
Reading real result combinations
A number on its own is a poor guide. Clinicians think in patterns. Here are the common combinations and what each typically signals, so you can see how the same phosphorus value can mean very different things.
- High phosphorus, low eGFR, high PTH: the classic picture of chronic kidney disease. The kidney cannot clear phosphate, and the parathyroid glands ramp up to try to force it out. This is the pattern that needs steady, long-term management.
- High phosphorus, high calcium, low PTH: suggests too much vitamin D or a phosphate load from supplements or laxatives, since low PTH means the body is not driving the calcium up on its own.
- High phosphorus, low calcium, low PTH: points toward hypoparathyroidism, where missing PTH lets phosphate rise and calcium fall together.
- High phosphorus, normal everything else, feeling fine: often a lab artifact or a timing effect. A repeat fasting morning draw frequently comes back normal.
- Sharply high phosphorus after chemotherapy or a crush injury: raises concern for tumor lysis or muscle breakdown releasing phosphate from inside cells, which can be urgent.
The lesson is simple. A high phosphorus is a question, not an answer. The surrounding panel supplies the answer.
How to prepare for the test and what throws it off
Phosphorus is one of the more easily distorted blood tests, and a surprising number of high readings are not real. Knowing the pitfalls helps you avoid a false alarm.
- Time of day matters. Blood phosphate follows a daily rhythm, sitting lowest in the early morning and peaking in the late afternoon and evening, with a swing of roughly 0.5 to 1.0 mg/dL (Phosphate reference range, Medscape). A late-day draw can read high simply from timing. Morning collection gives the most consistent result.
- Fasting reduces noise. A phosphate-rich meal transiently lifts the level. Drawing fasting, at the same time of day, cuts the natural person-to-person variation roughly in half.
- Hemolysis inflates it. Phosphate lives mostly inside cells. If red cells rupture during a difficult draw or delayed processing, they spill phosphate and can falsely raise the reading substantially (Phosphate, eClinpath). A note of hemolysis on the report is a reason to repeat.
- Supplements and medicines. Vitamin D at high doses, phosphate-containing laxatives or enemas, and some intravenous treatments can push the number up. Tell your clinician everything you take.
If your only high value is phosphorus and everything else looks normal, the right move is usually a repeat fasting morning draw before drawing any conclusion.

Phosphorus across the stages of kidney disease
Because retained phosphate is such a strong signal of kidney function, it helps to see when in the course of kidney disease it tends to rise. Phosphate is one of the later abnormalities to appear, which is exactly why it deserves attention when it does.
In the early stages of chronic kidney disease, phosphate usually stays normal. The body compensates by raising FGF23 and PTH, which force more phosphate out through the remaining kidney tissue. This hidden compensation is why FGF23 rises before phosphate does. Only when filtration falls substantially, generally once eGFR drops below about 30 mL/min, does the blood phosphate itself climb above range (Hyperphosphatemia, StatPearls, NCBI). A newly high phosphorus in someone with known kidney disease often signals that the disease has advanced, and it triggers a review of diet, binders, and dialysis timing.
How high phosphorus is managed, step by step
Treatment never targets the number in isolation. It targets the cause and the total mineral load, and it is layered from the least invasive step upward. Here is the usual order.
- Confirm it is real. Repeat the test fasting, in the morning, and rule out hemolysis. A large share of isolated high readings resolve here.
- Find the driver. Check kidney function, calcium, PTH, and vitamin D, and review medicines and supplements for hidden phosphate sources.
- Cut absorbed phosphate. The highest-yield diet move is removing inorganic phosphate additives, the “phos” ingredients in processed food, colas, and packaged meats, rather than eliminating whole foods. Absorbed phosphate, not total phosphate, is what matters.
- Add phosphate binders when needed. In kidney disease, binders taken with meals grab phosphate in the gut before it is absorbed. They only work if taken with food, a detail people often miss (National Kidney Foundation).
- Treat the underlying disease. That may mean adjusting vitamin D, managing parathyroid problems, or optimizing dialysis. The phosphorus follows once the driver is controlled.
Notice that diet and binders sit in the middle, not at the top. Confirming the value and identifying the cause come first, because chasing a falsely high or single reading with restrictions helps no one.
Who should test phosphorus, and how often
Phosphorus is not a screening test for the general healthy population the way cholesterol or glucose is. It earns its place when there is a reason to watch mineral balance. You have a stronger case to track it if you fall into one of these groups.
- Anyone with chronic kidney disease. Phosphate is monitored routinely as kidney function declines, because it is a modifiable driver of cardiovascular risk. The frequency rises as the disease advances and is set by your nephrologist.
- People on dialysis. Phosphate is checked regularly, often monthly, because control directly affects vessel calcification and outcomes.
- Anyone with a parathyroid or vitamin D disorder. Both shift phosphate, so it is followed alongside calcium and PTH.
- People taking phosphate-containing laxatives or high-dose vitamin D. A one-time check makes sense if use is heavy or prolonged.
For a healthy adult with normal kidneys, an isolated high phosphorus on a routine panel is most often a timing or collection effect. The right response is a careful repeat, not immediate alarm. For anyone with a kidney, parathyroid, or vitamin D condition, a rising trend over several tests is the signal that carries weight, not any single value.
Common misconceptions about a high phosphorus result
Several beliefs about high phosphorus are wrong or oversimplified, and they lead people to worry about the wrong things.
- “High phosphorus means I ate too much phosphorus.” Diet alone rarely pushes a healthy person over the line, because working kidneys clear the excess. Persistent high phosphate almost always involves the kidney or a hormone problem, not just food.
- “All dietary phosphorus is equal.” It is not. The inorganic phosphate added to processed foods and colas is absorbed far more efficiently than the natural phosphorus bound up in beans, nuts, and dairy, so additives matter more than raw milligrams.
- “A single high reading is a diagnosis.” It is not. Timing, a non-fasting draw, or hemolysis can each create a falsely high value. One reading is a prompt to repeat and check kidney function, nothing more.
- “If I feel fine, a high phosphorus does not matter.” Mild elevation is usually silent yet still meaningful, because years of high phosphate quietly calcify blood vessels. The absence of symptoms is not the absence of risk.
- “Only people on dialysis need to care.” Dialysis patients face the highest risk, but rising phosphate in earlier kidney disease is an early warning that management can still change.
How to track phosphorus over time and read the trend
A single high phosphorus reading tells you far less than a series of them, because the number swings with what you ate before the draw, how hydrated you were, and even the time of day. The value worth watching is the trend, and the way to build a trend that means something is to standardize the conditions. Draw at roughly the same time of day, keep the fasting state consistent from one test to the next, and avoid a large protein or dairy heavy meal right before a scheduled draw. When the conditions match, a rising line across several months is a real signal rather than noise.
The trend also has to be read alongside its partners rather than in isolation. Phosphorus that climbs while calcium drifts down and PTH rises is the classic picture of failing kidney control, and it deserves closer attention than phosphorus alone. Phosphorus that spikes once, then returns to baseline on a repeat, usually points to a meal or a supplement rather than a disease. For anyone with reduced kidney function, the practical habit is to log each result with the date, the lab, and any recent change in diet or medication, then bring that log to the same clinician so one person can see the whole arc. A number that creeps up slowly over a year is easy to miss on a single sheet and obvious on a chart.
One caution when comparing results: make sure the readings come from the same laboratory where possible, since methods and reference ranges differ slightly between labs and a change in provider can look like a change in your body when it is really a change in the ruler. If you must switch labs, note it, and give the new baseline a chance to establish itself before reacting to a single value.
Turn what you just learned about phosphorus into action.
Superpower lets you test phosphorus and 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
What is a dangerously high phosphorus level?
Any level above 4.5 mg/dL is high, but levels are considered seriously elevated when they climb well above that, especially with symptoms or low calcium. Sudden severe spikes from phosphate enemas can be life threatening and need emergency care (StatPearls, NCBI).
Can dehydration cause high phosphorus?
Dehydration can mildly concentrate blood and nudge several lab values, but it is not a typical cause of true hyperphosphatemia. The main drivers are reduced kidney clearance, excess intake, and cell breakdown (StatPearls, NCBI). Persistent high phosphorus warrants a kidney workup.
What foods are highest in phosphorus?
Processed and packaged foods with phosphate additives are the biggest source, since that inorganic phosphate is absorbed very efficiently. Colas, processed meats, cheese, and some baked goods rank high. Natural sources include dairy, beans, nuts, and meat (National Kidney Foundation).
Does high phosphorus always mean kidney disease?
No. Kidney disease is the most common cause, but high phosphorus can also come from hypoparathyroidism, vitamin D excess, certain laxatives, or cell breakdown. A lab artifact called pseudohyperphosphatemia can mimic it too (StatPearls, NCBI). Your doctor confirms the cause.
How do you lower high phosphorus?
Treatment depends on the cause. Common steps include cutting phosphate additives in processed foods, stopping phosphate-containing supplements or laxatives, and, in kidney disease, taking phosphate binders with meals (National Kidney Foundation). Always follow your clinician’s specific plan.
Sources
- Cleveland Clinic, Hyperphosphatemia: Causes, Symptoms and Treatment
- StatPearls, NCBI Bookshelf, Hyperphosphatemia
- National Kidney Foundation, High Phosphorus (Hyperphosphatemia)
- MedlinePlus, Phosphate in Blood
- American Kidney Fund, High Phosphorus (Hyperphosphatemia)
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


