
Low cortisol can signal adrenal issues, so is your morning level actually in a healthy range? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
- Low cortisol in a blood test means your adrenal glands are not making enough of the body’s main stress hormone, and a morning level below 3 mcg/dL strongly suggests adrenal insufficiency (Cleveland Clinic).
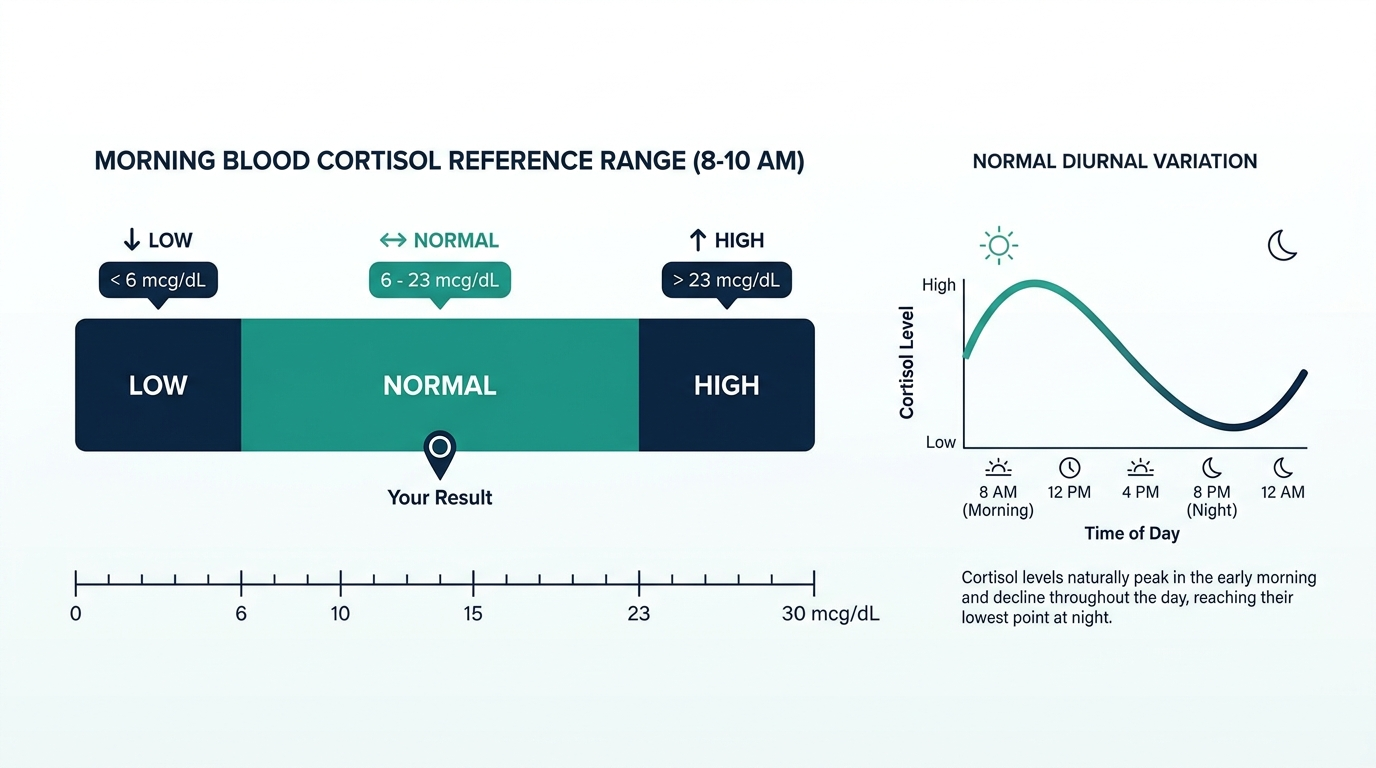
- A normal morning cortisol level is roughly 10 to 20 mcg/dL between 6 a.m. and 8 a.m., so a result well under this range is the threshold that prompts further testing (Cleveland Clinic).
- Low cortisol can be caused by damaged adrenal glands (Addison disease), a pituitary problem, or sudden withdrawal from long-term steroid medication, and severe cases can become a life-threatening adrenal crisis (Cleveland Clinic, NCBI StatPearls).
A low cortisol result on a blood test can be unsettling, especially when you have been feeling tired, dizzy, or weak for weeks. Cortisol is the hormone that helps you wake up, manage stress, keep blood pressure steady, and regulate blood sugar. When the number comes back low, it usually points to your adrenal or pituitary glands, not to something you did wrong. This guide explains what the result means, what causes it, the symptoms to watch for, when it becomes dangerous, and the exact next steps to take with your clinician.
What does a low cortisol result mean and what is the cutoff?
A low cortisol result means your body is not producing enough cortisol, the primary stress hormone made by your adrenal glands. A normal morning level is about 10 to 20 mcg/dL when measured between 6 a.m. and 8 a.m., and drops to roughly 3 to 10 mcg/dL by 4 p.m. (Cleveland Clinic). A morning value below 3 mcg/dL is consistent with adrenal insufficiency and often needs no further testing if symptoms match, while a value above 13 to 18 mcg/dL generally rules it out (Cleveland Clinic Journal of Medicine).
Timing matters enormously. Cortisol follows a daily rhythm, peaking in the early morning and falling at night, so a blood draw is normally scheduled around 8 a.m. A “low” afternoon reading can be completely normal because that is when cortisol naturally bottoms out. This is why your clinician interprets the number against the time of day, not against a single fixed line.

What causes low cortisol?
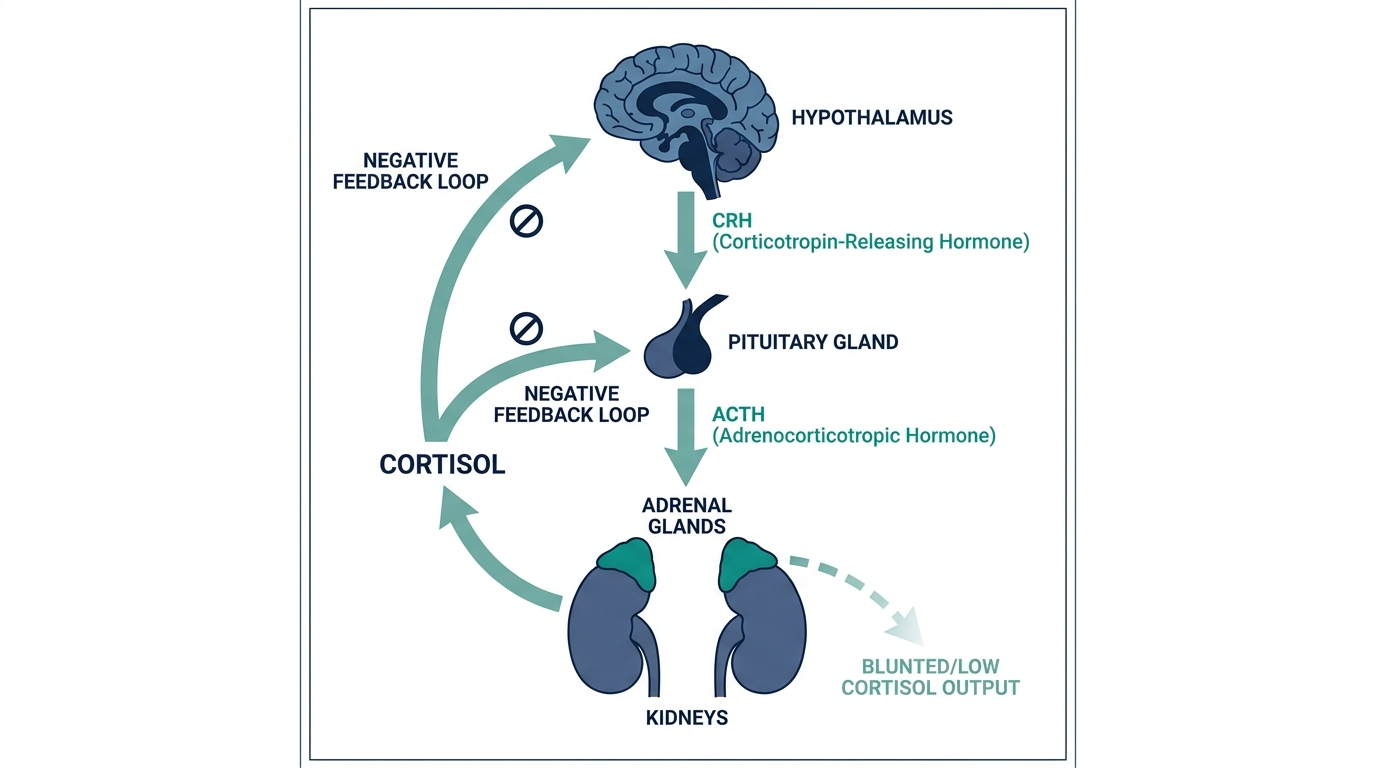
Low cortisol is most often caused by a problem in one of three places: the adrenal glands themselves, the pituitary gland that signals them, or sudden withdrawal from steroid medication. Primary adrenal insufficiency, also called Addison disease, occurs when the adrenal glands are damaged, and an ACTH level at or above 50 pg/mL paired with cortisol under 5 mcg/dL is diagnostic (NCBI StatPearls).
- Adrenal gland damage (Addison disease): autoimmune destruction, infection, or bleeding stops the glands from making cortisol.
- Pituitary problems (secondary): a tumor or underactive pituitary reduces ACTH, the signal that tells the adrenals to release cortisol (Cleveland Clinic).
- Steroid withdrawal (tertiary): stopping long-term prednisone or similar drugs too quickly leaves the adrenals temporarily suppressed.
Less common causes include certain cancer immunotherapy drugs and infections that affect the adrenal glands. Identifying the location of the problem is what an ACTH test and stimulation test are designed to pinpoint.
What are the symptoms of low cortisol?
The symptoms of low cortisol build slowly and are easy to dismiss as ordinary tiredness, which is why adrenal insufficiency is often diagnosed late. The classic combination is persistent fatigue, unexplained weight loss, low blood pressure, and salt cravings, and in Addison disease the skin can darken in creases and scars (NCBI StatPearls).
Common signs include:
- Fatigue: deep, lasting tiredness that rest does not fix.
- Dizziness: lightheadedness on standing because blood pressure runs low.
- Weight loss and poor appetite: often with nausea or stomach upset.
- Muscle weakness and body aches.
- Salt craving and darkened skin: more specific to primary adrenal insufficiency.
Low cortisol is rarely silent once it is significant, but mild or early cases can show only vague fatigue and mood changes, so the blood test result often arrives before the picture is obvious.
When is low cortisol dangerous?
Low cortisol becomes a medical emergency when it triggers an adrenal crisis, also called an Addisonian crisis. This can develop within hours during physical stress such as infection, surgery, injury, or vomiting, and it is potentially fatal without immediate treatment (NCBI StatPearls). The body cannot mount its normal stress response, so blood pressure and blood sugar can collapse.
Warning signs of an adrenal crisis that need emergency care include sudden severe weakness, confusion, intense abdominal or leg pain, repeated vomiting or diarrhea, very low blood pressure, and loss of consciousness. Treatment is urgent intravenous hydrocortisone plus fluids. If you have known adrenal insufficiency, you and the people around you should recognize these signs and have an emergency steroid injection plan from your clinician. Do not wait to see if symptoms pass on their own.

What to do next and when to see a doctor
If your blood test shows low cortisol, the single most important step is to follow up with your clinician promptly rather than starting any supplement on your own. The standard next step is an ACTH stimulation test, which checks how your adrenal glands respond after a shot of synthetic ACTH and confirms or rules out adrenal insufficiency (Cleveland Clinic).
A practical sequence usually looks like this:
- Repeat the test correctly: a fresh morning draw around 8 a.m., since timing changes the number.
- Add an ACTH level: this separates an adrenal problem from a pituitary one.
- Stimulation test: the cosyntropin test is the reference standard for confirming the diagnosis.
- See a doctor urgently if you have severe weakness, vomiting, confusion, or fainting, which can signal an adrenal crisis.
Bring a list of all medications, especially any steroids, because they directly affect cortisol readings.
Insider nuance: why one low number rarely settles the diagnosis
Here is what experienced clinicians know that lab reports do not spell out: a single low cortisol value is a screening signal, not a verdict. The cutoff that “rules out” adrenal insufficiency ranges from 13 to 18 mcg/dL depending on which assay your lab uses, and newer assays tend to read lower, so the same blood could be flagged differently between two hospitals (Cleveland Clinic Journal of Medicine).
Two other traps catch people. First, oral estrogen and pregnancy raise cortisol-binding globulin, which can make total cortisol look falsely reassuring or falsely low. Second, recent steroid use, including inhaled or joint-injection steroids, can suppress your own cortisol temporarily. This is why the stimulation test, not a one-off morning blood draw, is what endocrinologists rely on to commit to a diagnosis.
How the cortisol test is actually run
Understanding how the sample is collected explains why timing and method change your result so much. Cortisol can be measured in several ways, and each answers a slightly different question.
- Morning blood cortisol: the workhorse screen, drawn between 6 a.m. and 8 a.m. to catch the natural peak. This is the number most people see first.
- ACTH stimulation (cosyntropin) test: the reference standard. A synthetic ACTH shot is given, and cortisol is measured 30 and 60 minutes later. A healthy adrenal gland climbs above roughly 18 to 20 mcg/dL. A flat response confirms adrenal insufficiency.
- Salivary cortisol: often collected late at night to assess the low point of the rhythm, useful in evaluating the opposite problem (excess cortisol) but sometimes used to map the daily curve.
- 24-hour urinary free cortisol: captures total daily output rather than a single moment, smoothing out the effect of the daily rhythm.
The takeaway is that a low morning blood cortisol is a doorway, not a diagnosis. Endocrinologists lean on the stimulation test because it measures reserve capacity, meaning what your glands can do under demand, rather than what they happen to be doing at one quiet moment.

Reading cortisol alongside its partner markers
A cortisol value gains most of its meaning from the markers read next to it, because those partners reveal where in the chain of command the problem sits.
| Marker | What it adds |
|---|---|
| ACTH | High ACTH with low cortisol points to the adrenal glands (primary, Addison disease). Low or normal ACTH with low cortisol points to the pituitary (secondary). |
| Sodium and potassium | In Addison disease, aldosterone also falls, so sodium tends to run low and potassium high. This electrolyte pattern is a classic clue. |
| Aldosterone and renin | Low aldosterone with high renin supports primary adrenal failure, separating it from a pituitary cause where aldosterone is usually preserved. |
| Glucose | Cortisol supports blood sugar, so low cortisol can show up with a tendency toward low glucose, especially when fasting or ill. |
| Thyroid hormones | Autoimmune adrenal disease often travels with autoimmune thyroid disease, so a paired abnormality can hint at a broader autoimmune picture. |
This is why a single low cortisol rarely stands alone on the order sheet. The electrolytes, ACTH, and glucose around it turn a lonely number into a coherent story your clinician can act on.
What can throw off a cortisol result
Cortisol is one of the more easily distorted lab values because it responds to time of day, stress, hormones, and medication. Knowing the common distortions helps you and your clinician avoid a false conclusion.
- Time of day: the single largest factor. An afternoon or evening draw naturally reads low and can look alarming when it is simply normal for the hour.
- Acute stress or illness: pain, infection, or the stress of the blood draw itself can transiently raise cortisol, sometimes masking a real deficiency.
- Estrogen and pregnancy: oral estrogen and pregnancy raise cortisol-binding globulin, inflating total cortisol and potentially hiding a true deficiency, since most assays measure total, not free, cortisol.
- Steroid medications: prednisone, dexamethasone, inhaled steroids, steroid creams, and joint injections all suppress your own cortisol production and can mimic adrenal insufficiency. Some synthetic steroids also cross-react with the assay.
- Shift work and disrupted sleep: a scrambled sleep schedule shifts the cortisol rhythm, so the usual morning peak may not fall where the clock expects it.
Bring a complete medication list, including creams and inhalers, and make sure any repeat test is a properly timed morning draw. These two steps prevent most of the confusion that low cortisol results create.
Living with low cortisol: sick-day rules and daily management
If testing confirms adrenal insufficiency, the condition is highly manageable, but it requires you to become an active partner in your own care. The core of treatment is replacing the cortisol your body cannot make, usually with hydrocortisone taken to mimic the natural daily rhythm, sometimes with a mineralocorticoid such as fludrocortisone in primary disease.
The concept that saves lives is stress dosing, often called sick-day rules. Because your body cannot ramp up cortisol on its own during illness or injury, you and your clinician plan to increase the dose temporarily when your body is under stress.
- Minor illness with fever: the maintenance dose is typically doubled or tripled for the duration, then tapered back.
- Vomiting or diarrhea: oral pills may not absorb, so an emergency injection plan matters here.
- Surgery, major injury, or childbirth: higher intravenous doses are arranged in advance with your care team.
- Everyday practicalities: carrying a medical alert bracelet and an emergency hydrocortisone injection kit, and teaching a family member how to use it, are standard precautions.
With this framework in place, people with adrenal insufficiency live full, active lives. The danger is not the condition itself but a missed stress dose during illness, which is exactly what the sick-day plan is designed to prevent.

Sample scenarios: how the same low number is read differently
Because cortisol depends so heavily on context, it helps to see how identical numbers lead to different conclusions. These scenarios are illustrative teaching cases, not descriptions of specific patients.
- Low morning cortisol, high ACTH, low sodium, high potassium: this pattern strongly suggests primary adrenal insufficiency (Addison disease), where the glands themselves have failed and aldosterone has dropped too. Next step is confirmation and starting both glucocorticoid and mineralocorticoid replacement.
- Low morning cortisol, low or normal ACTH, normal electrolytes: this points toward a pituitary cause (secondary adrenal insufficiency). The workup turns toward the pituitary, and mineralocorticoid replacement is usually not needed because aldosterone is preserved.
- Low afternoon cortisol, no symptoms: often simply the normal daily trough. A properly timed morning draw usually returns a reassuring value, and no treatment is needed.
- Low cortisol during recent prednisone taper: the adrenals are suppressed but likely recoverable. Management focuses on a careful, supervised taper with stress-dose coverage until the glands restart.
Seeing these side by side makes the central lesson concrete: the same low cortisol can mean an emergency, a recoverable suppression, or nothing at all, depending entirely on the timing and the markers that accompany it.
Who should get tested and how often to monitor
Cortisol testing is not a routine screen for everyone. It is aimed at people whose symptoms or history raise the possibility that the stress-hormone system is underperforming. Consider evaluation if you have unexplained, persistent fatigue with any of the following: low blood pressure or dizziness on standing, unintended weight loss, salt craving, darkening skin, or recurrent low blood sugar. Testing is also warranted for anyone tapering off long-term steroid therapy, since the adrenal glands may not have fully restarted, and for people with known pituitary disease or prior pituitary surgery or radiation.
Once a diagnosis is made, monitoring shifts from making the diagnosis to fine-tuning treatment. Follow-up is usually based on symptoms and clinical signs rather than chasing a specific blood cortisol on replacement therapy, because timing the pill against the draw makes the number hard to interpret. Your clinician will watch for signs of too little replacement (fatigue, nausea, low blood pressure) or too much (weight gain, high blood pressure, poor sleep), and in primary disease will also track sodium, potassium, and renin to judge the mineralocorticoid dose. A yearly review is typical for stable patients, with extra checks after any major life or medication change.
Common misconceptions about low cortisol
Low cortisol sits at the center of a lot of online confusion, some of it harmful. Separating fact from myth protects you from both false alarm and false reassurance.
- “Adrenal fatigue explains my low cortisol.” The term adrenal fatigue is not a recognized medical diagnosis. True adrenal insufficiency is a specific, testable condition; vague tiredness with a normal stimulation test is not it.
- “A supplement can boost my cortisol.” No over-the-counter supplement reliably treats genuine adrenal insufficiency, and delaying real treatment can be dangerous. Some glandular supplements contain hidden steroids, which carry their own risks.
- “One low reading means I have Addison disease.” A single low value, especially an afternoon one, is a screening signal. Confirmation needs a properly timed test plus ACTH and often a stimulation test.
- “If I feel fine, I can skip doses.” Skipping replacement steroids can trigger an adrenal crisis, particularly during illness. Consistency is essential.
- “Stress is draining my cortisol.” Ordinary stress raises cortisol. Persistently low cortisol reflects a gland or signaling problem, not everyday pressure.
Questions patients ask most about a low cortisol result
A few questions come up again and again once someone sees a low cortisol on their report, and the honest answers tend to defuse a lot of worry. The first is whether a low morning cortisol always means adrenal insufficiency. It does not. A single low reading can reflect the time of the draw, poor sleep the night before, a recent steroid inhaler or joint injection, or simply the wide bounce cortisol shows from hour to hour. The value earns its meaning only when it is repeated under the right conditions and paired with the pituitary signal, ACTH.
The second common question is whether stress can lower cortisol. Most people expect stress to raise it, and in the short term it does. What surprises them is that a long, grinding illness or a period of very heavy steroid use can leave the adrenal glands underactive afterward, so the number reads low precisely when life has been hardest. That is a pattern worth naming to your clinician rather than dismissing.
People also ask whether they can fix a low cortisol with diet, salt, or supplements sold for “adrenal fatigue.” There is no credible evidence that over the counter adrenal support products correct a true cortisol deficiency, and leaning on them can delay a diagnosis that actually matters. If the low value is real and symptomatic, the treatment is medical, not nutritional. Salt cravings and lightheadedness on standing are clues to mention, not problems to self treat.
Finally, many want to know how to track the number sensibly over time rather than testing on impulse. The useful rhythm is to draw cortisol at the same early morning window each time, note any steroid exposure in the prior weeks, and bring the trend to the same clinician so one person is reading the whole arc. A steady low that tracks with fatigue, weight loss, and low blood pressure tells a very different story than a one off dip after a bad night, and only a series of readings can separate the two.
Curious where your cortisol really sits?
Baseline cortisol and 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
What level of cortisol is considered too low?
A morning blood cortisol below 3 mcg/dL is strongly consistent with adrenal insufficiency, while a level above 13 to 18 mcg/dL usually rules it out (Cleveland Clinic). Values in between often need an ACTH stimulation test to confirm.
Can stress cause low cortisol?
Short-term stress raises cortisol, not lowers it. However, very long-term illness, sudden withdrawal from steroid medication, or pituitary and adrenal damage can leave cortisol low. Persistently low cortisol is a medical issue, not ordinary daily stress, and should be evaluated.
What is the difference between Addison disease and secondary adrenal insufficiency?
Addison disease is primary adrenal insufficiency, where the adrenal glands themselves are damaged, often with high ACTH and skin darkening. Secondary adrenal insufficiency comes from a pituitary problem that reduces the ACTH signal. An ACTH blood level helps tell them apart (NCBI StatPearls).
Why was my afternoon cortisol low but my doctor was not worried?
Cortisol naturally peaks in the early morning and falls to roughly 3 to 10 mcg/dL by 4 p.m. (Cleveland Clinic). A low afternoon reading can be entirely normal. Diagnosis relies on a properly timed morning draw, usually around 8 a.m.
Can low cortisol be cured?
Most adrenal insufficiency is managed, not cured, with daily steroid replacement that restores normal cortisol levels and lets people live full lives. The exact treatment depends on the cause. Steroid withdrawal cases may recover once the adrenals restart, under medical supervision.
Sources
- Cleveland Clinic, Cortisol Test: What It Is, Purpose, Types and Results
- NCBI StatPearls, Addison Disease
- Cleveland Clinic Journal of Medicine, Primary adrenal insufficiency in adults
- NCBI Endotext, Adrenal Insufficiency
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Related: best at-home thyroid and hormone tests.
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


