
You have a swollen, achy calf, or a sudden shortness of breath, and somewhere in your head a quiet alarm goes off: could this be a clot? It is one of the few medical worries where the instinct to take it seriously is exactly right. Blood clots in the deep veins and lungs can turn dangerous fast, and the testing path to confirm or rule one out is more layered than most people expect.
A swollen calf or sudden shortness of breath deserves a real answer. See how bloodwork fits into ruling out a clot. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Here is what surprises people. There is no single blood test that simply lights up and says clot. The process is a sequence, and one of the most important tests in it is valued not for finding clots but for safely ruling them out.
How to test for blood clots
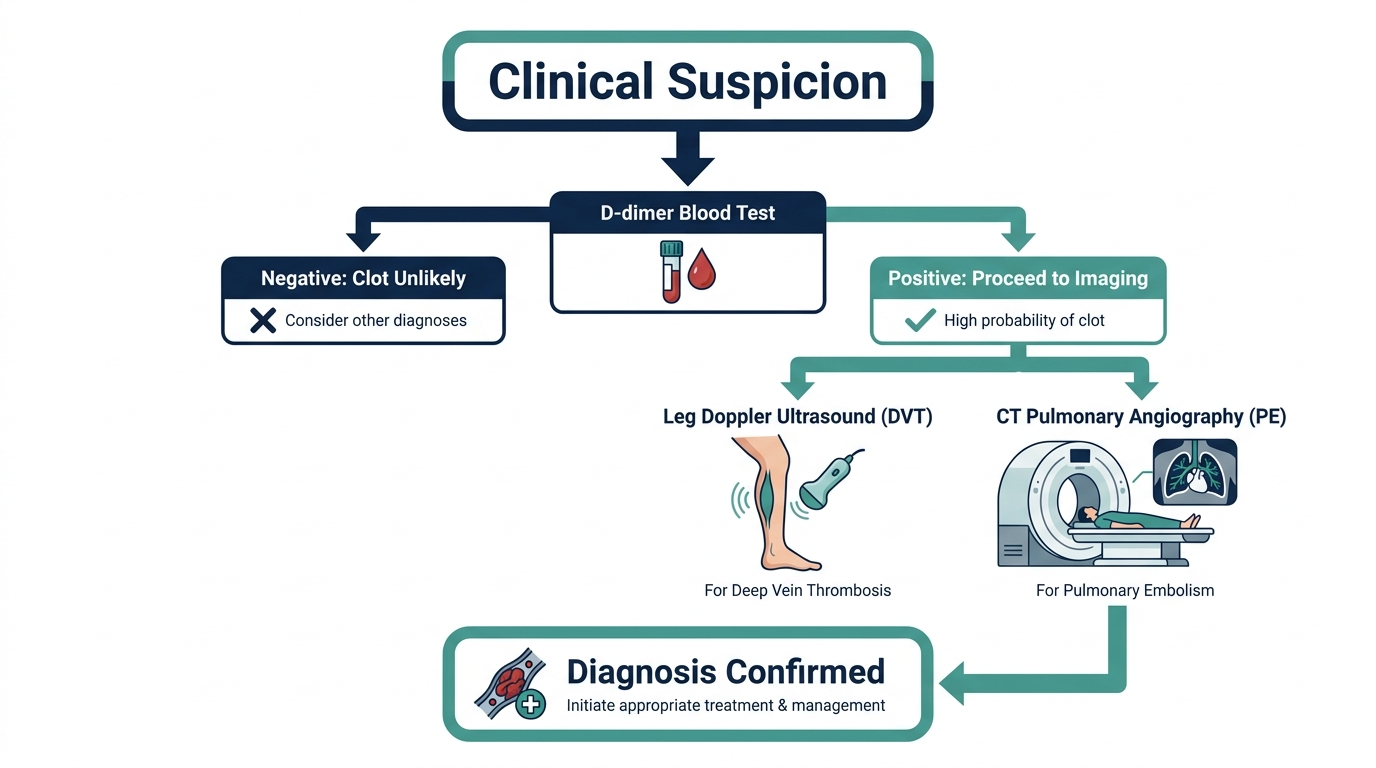
To test for blood clots, clinicians combine a clinical risk assessment, a blood test called D-dimer, and an imaging scan, usually an ultrasound or a CT scan. No one of these alone confirms a clot. They work as a funnel, each step narrowing down whether a dangerous clot such as a deep vein thrombosis (DVT) or pulmonary embolism (PE) is present (Mayo Clinic).
The order matters. A doctor first estimates how likely a clot is based on your symptoms and risk factors. If the suspicion is low to moderate, a D-dimer blood test comes next. If that is negative, a clot is usually off the table. If it is positive, or if suspicion was high to begin with, imaging confirms where the clot actually is (NCBI StatPearls).
What warning signs should send you to get tested?
The simplest way to actually get this done
Superpower is a full-body lab membership that runs 100+ biomarkers, has each result reviewed by a doctor, and tracks your numbers year over year (about $199/year). It is what we point readers to when they would rather get one clean, complete draw than chase single tests one at a time. Here is superpower reviewed in full.
Knowing the symptoms is what gets people to testing early, while a clot is most treatable. A deep vein clot, usually in the calf or thigh, tends to announce itself in one leg rather than both. The classic signs are swelling, a deep ache or cramp that will not ease, warmth over the area, and skin that looks reddened or discolored. Pain that worsens when you stand or walk, in a single leg, is a pattern worth taking seriously.
A clot that has traveled to the lungs is a different and more urgent picture. Sudden shortness of breath, sharp chest pain that gets worse when you breathe in, a fast heartbeat, lightheadedness or fainting, and a cough that may bring up blood are the red flags. These are a reason to seek emergency care immediately rather than wait for a scheduled appointment. A pulmonary embolism can be life threatening, and the testing described below happens quickly in that setting for exactly that reason.
Who is more likely to develop a blood clot?
Testing decisions lean heavily on risk, so it helps to know where you sit. The single biggest everyday trigger is immobility: long flights or car trips, bed rest, or the weeks after an operation, when blood pools in still legs. Surgery itself, especially orthopedic procedures, and any major trauma raise the odds sharply.
Several ongoing factors matter too. Cancer and its treatments, pregnancy and the weeks after delivery, estrogen-containing birth control or hormone therapy, obesity, smoking, and increasing age all push clotting risk up. A personal or family history of clots is a strong signal, and some people carry inherited clotting disorders, such as factor V Leiden, that raise the risk across a lifetime. The more of these that stack up, the more a clinician leans toward imaging rather than resting on a single blood test.
What blood test shows blood clots?
The main blood test used to screen for blood clots is the D-dimer test. D-dimer is a small protein fragment released when a blood clot in your body starts to break down (MedlinePlus). In healthy blood, there is very little of it. When your body is actively forming and dissolving clots, the level climbs, which is why it is the go-to blood test when DVT, PE, or disseminated intravascular coagulation (DIC) is suspected.
So when people ask what blood test is for blood clots or what test for blood clots their doctor will order, the answer in almost every case is D-dimer first. It is fast, widely available, and needs only a standard blood draw (Cleveland Clinic). But the way it is used is counterintuitive, and that is the part worth understanding.
Do blood tests show blood clots, or just hint at them?
Blood tests hint at clots rather than prove them. A D-dimer test cannot tell your doctor whether you actually have a clot, where it is, or why it formed. It only tells them whether clot breakdown products are present in your blood (Cleveland Clinic). That distinction is the whole reason imaging exists.
This is the most common misunderstanding patients have. A positive D-dimer feels like a diagnosis, but it is not. Plenty of everyday situations raise D-dimer without any dangerous clot at all: recent surgery, trauma, infection, pregnancy, heart disease, rheumatoid arthritis, and simply being older (MedlinePlus). That is why a positive result almost always triggers a follow-up scan instead of immediate treatment.
How do doctors judge the odds before any test?
The first step in the funnel is not a needle, it is a structured judgment. Clinicians estimate the pretest probability of a clot from your symptoms and risk factors, often with a scoring tool such as the Wells criteria that tallies findings like leg swelling, recent immobility, active cancer, and whether a clot is the most likely explanation for what you are feeling. That score sorts you into low, moderate, or high likelihood before a single lab is drawn.
This step is what makes the D-dimer useful rather than confusing. A negative D-dimer means something very different in a low-probability patient, where it can close the case, than in a high-probability one, where it is not trusted on its own. Understanding that your result is always read against your pretest risk explains why two people with the same D-dimer number can be sent down completely different paths.
What is the normal D-dimer level, and what does a result mean?
A conventional normal D-dimer is below 500 ng/mL (0.50 micrograms/mL). A value of 500 ng/mL or higher is considered positive (NCBI StatPearls). That said, labs use different methods and units, so there is no single universal cutoff, and you should always read your result against the reference range printed on your own report (Cleveland Clinic).
Here is how to read it in plain terms. A negative D-dimer, in someone whose symptoms already pointed to low or moderate risk, is powerful. It effectively rules out a clot, and no scan may be needed (NCBI StatPearls). A positive D-dimer is much weaker on its own. It means clotting activity is possible, and the next step is imaging to actually look for the clot (MedlinePlus).
What is the test for blood clots that actually confirms one?
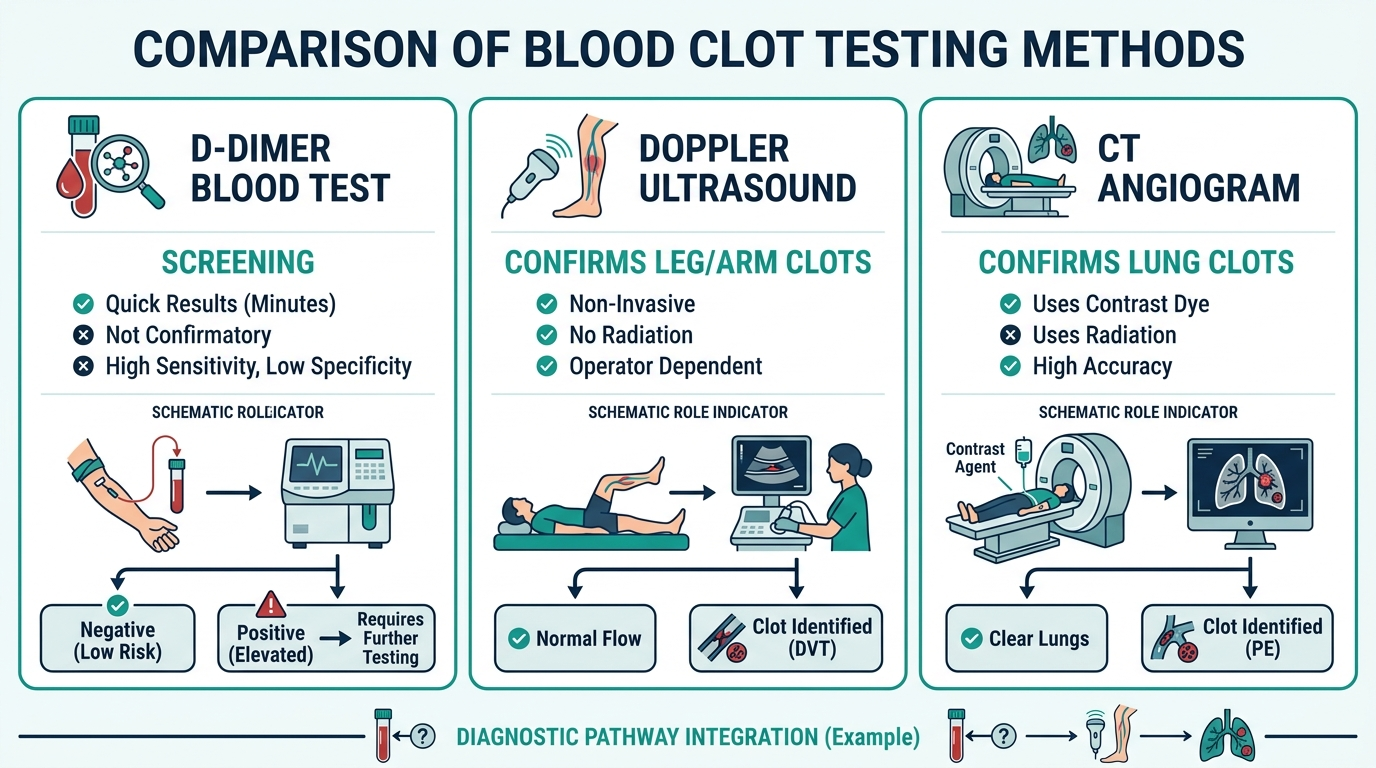
Imaging confirms a blood clot, not a blood test. For a suspected clot in the leg, the first-choice test is a duplex (Doppler) ultrasound, which uses sound waves to watch blood flow through the veins and is the standard test for diagnosing DVT (Mayo Clinic). It is painless, uses no radiation, and can usually pinpoint a clot in the deep thigh veins quickly.
For a suspected clot in the lungs, the workhorse is CT pulmonary angiography, a special CT scan with contrast dye that shows the blood vessels in the lungs. It is the most common test used to diagnose pulmonary embolism (Mayo Clinic). Two other tools fill specific gaps:
- V/Q scan (ventilation-perfusion scan). Measures air and blood flow in the lungs, often used for PE when CT contrast dye is not a good option, such as in pregnancy or kidney problems (MedlinePlus).
- Venography. An older test using x-rays and injected dye to map the leg veins. It is invasive and now used rarely, mostly when ultrasound is inconclusive (Mayo Clinic).
So how do you test for blood clots in practice? Blood draw for D-dimer, then ultrasound for the legs or CT for the lungs. The blood test screens, the scan confirms.
The insider point: a negative D-dimer is worth more than a positive one
This is the part that even many patients who have had the test never grasp. D-dimer has high sensitivity but low specificity (NCBI StatPearls). In plain language, it almost never misses a real clot, but it raises a lot of false alarms. That lopsided profile is not a flaw. It is exactly why the test is used the way it is.
Because it rarely misses, a negative D-dimer in a low to moderate risk patient effectively excludes both DVT and pulmonary embolism, often sparing that person a CT scan, radiation, and contrast dye (NCBI StatPearls). The test earns its place by ruling clots out, not ruling them in. A skilled clinician orders D-dimer hoping it comes back negative, because that single result can safely close the case.
There is a refinement clinicians use that patients almost never hear about. For people over 50, an age-adjusted cutoff (age in years multiplied by 10 ng/mL) is increasingly used, because D-dimer naturally drifts upward with age (NCBI StatPearls). Using the older fixed 500 cutoff in a 75-year-old generates far more false positives and unnecessary scans. If you are older and your result sits just above 500, that context is worth asking your doctor about.
The trap to avoid is reading a positive D-dimer in isolation and panicking. Out of context, it means very little. Out of context with a negative result, though, you can usually exhale.
When should you not rely on a blood test alone?
You should never rely on D-dimer alone when clinical suspicion of a clot is high. If your symptoms strongly suggest a clot, for example a swollen, painful leg plus sudden breathlessness, doctors often skip straight to imaging, because a falsely reassuring blood test in a high-risk patient is dangerous (NCBI StatPearls). D-dimer is most useful in the low to moderate risk window, not at the extremes.
It also has real limits in specific groups. Blood thinner medication can produce a falsely low D-dimer, masking clotting activity (MedlinePlus). And in pregnancy, recent surgery, active infection, or cancer, D-dimer is so often elevated for unrelated reasons that a positive result tells you almost nothing without imaging (Cleveland Clinic). This is why providers typically run D-dimer in an emergency or hospital setting where a scan can follow quickly if needed.
What happens after a clot is confirmed?
Confirming a clot is the start of treatment, not the end of testing. Most deep vein clots and pulmonary emboli are treated with anticoagulants, blood-thinning medication that stops the clot from growing and lets the body break it down over time. The type of medication and how long you stay on it depend on where the clot is, how severe it is, and what caused it.
That last part, the cause, often drives a second round of questions. If a clot appears without an obvious trigger, or keeps coming back, clinicians may look for an underlying reason, from an inherited clotting tendency to another condition that raises risk. This is also where a broader look at your health can matter, since clotting risk overlaps with heart, metabolic, and inflammatory markers. The immediate job is treating the clot safely, but the follow-up question of why it formed is what protects you from the next one.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
What blood test for blood clots will my doctor order first?
Almost always a D-dimer test. It measures protein fragments left behind when clots break down and is the standard first blood test when DVT or pulmonary embolism is suspected (MedlinePlus). It is used to decide whether you need imaging, not to confirm a clot by itself.
Do blood tests show blood clots directly?
No. A D-dimer test cannot show where a clot is or confirm one exists. It only signals that clotting activity may be present, which is then checked with an ultrasound or CT scan (Cleveland Clinic).
What is a normal D-dimer level?
A conventional normal D-dimer is below 500 ng/mL, with 500 ng/mL or higher considered positive, though labs vary in method and units (NCBI StatPearls). Always compare to the reference range on your own report.
What is the test for blood clots in the legs versus the lungs?
For the legs, a duplex (Doppler) ultrasound is the standard test for DVT. For the lungs, CT pulmonary angiography is the most common test for pulmonary embolism (Mayo Clinic).
Can a D-dimer be high without a blood clot?
Yes, often. Pregnancy, recent surgery, trauma, infection, heart disease, and older age can all raise D-dimer with no dangerous clot present, which is why a positive result needs imaging to interpret (MedlinePlus).
How long does a D-dimer test take?
The blood draw itself takes only a minute, and because D-dimer is used in urgent settings, labs typically turn the result around quickly, often within hours. That speed is part of why it works as a first screen before imaging (Cleveland Clinic).
Can you have a blood clot with a normal D-dimer?
It is uncommon but possible. D-dimer rarely misses a clot, which is its strength, yet blood thinner medication can produce a falsely low result, and a small clot may not raise the level much (MedlinePlus). When suspicion is high, doctors go straight to imaging regardless of the D-dimer (NCBI StatPearls).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


