
You suspect you might be pregnant, you do not want to wait two more weeks for a drugstore test to feel sure, and you are wondering whether a blood draw at the clinic can give you an answer sooner. The short version: yes, a blood test is the earliest reliable way to confirm a pregnancy, and it can catch the pregnancy hormone before a home test ever turns positive.
Timing a pregnancy blood test is stressful enough. Ever wondered what else a single draw could tell you? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
But the honest answer comes with a few days of wiggle room that nobody on the box ever explains. The timing hinges less on the test itself and more on something happening quietly inside your body. Here is exactly how soon, and why the number is not as fixed as you might hope.
How soon can a blood test detect pregnancy?
A blood test can usually detect pregnancy about 10 days after ovulation, which is several days earlier than most home urine tests. Cleveland Clinic puts it plainly: a doctor’s blood test can find pregnancy roughly 10 days after you ovulate, and can identify it within about 7 to 10 days after conception because it is more sensitive than a urine test and can pick up very small levels of the pregnancy hormone (Cleveland Clinic).
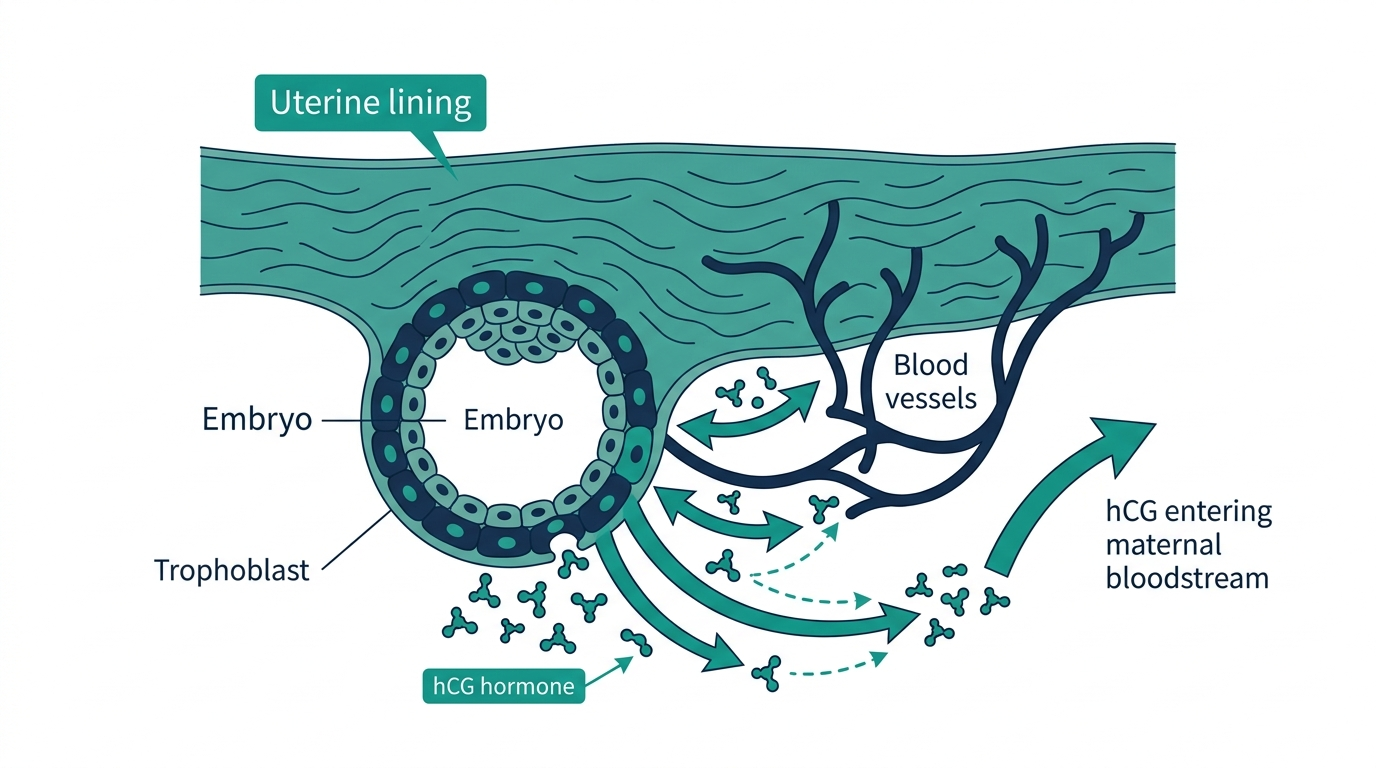
The hormone in question is human chorionic gonadotropin, or hCG. It is produced by the developing placenta only after a fertilized egg implants in the wall of the uterus. No implantation, no hCG, no positive test. That single fact is the key to the whole timeline, and it is why the answer to how soon can a blood test detect pregnancy is “earlier than a home test, but only after implantation has happened.”

How soon can a blood pregnancy test detect pregnancy compared to a urine test?
A blood pregnancy test can detect pregnancy before you have missed your period, while most urine tests are only reliable around or after the missed period. Blood tests can find very small amounts of hCG and can show whether you are pregnant earlier than urine tests can (MedlinePlus).
The gap comes down to sensitivity. A lab can measure hCG concentrations in the single digits, whereas a home urine test generally needs a higher concentration before it flips to positive. So when people ask how soon does a blood test detect pregnancy versus a stick at home, the practical answer is a few days sooner, sometimes before you would even think to test.
Here is the timeline most clinicians work with:
- Around 10 days after ovulation: a blood test can typically confirm pregnancy (Cleveland Clinic).
- Before a missed period: a blood test may already be positive while a home test is still negative (MedlinePlus).
- A week or two after a missed period: home urine tests reach their best accuracy, around 97 to 99 percent (MedlinePlus).
What hCG level can a blood test pick up?
A blood test can detect hCG at very low levels, well below what indicates a confirmed pregnancy in a non pregnant person. A quantitative hCG blood test reports the exact concentration in milli international units per milliliter (mIU/mL), and the reference point matters: in people who are not pregnant, hCG is generally less than 5 mIU/mL (MedlinePlus).
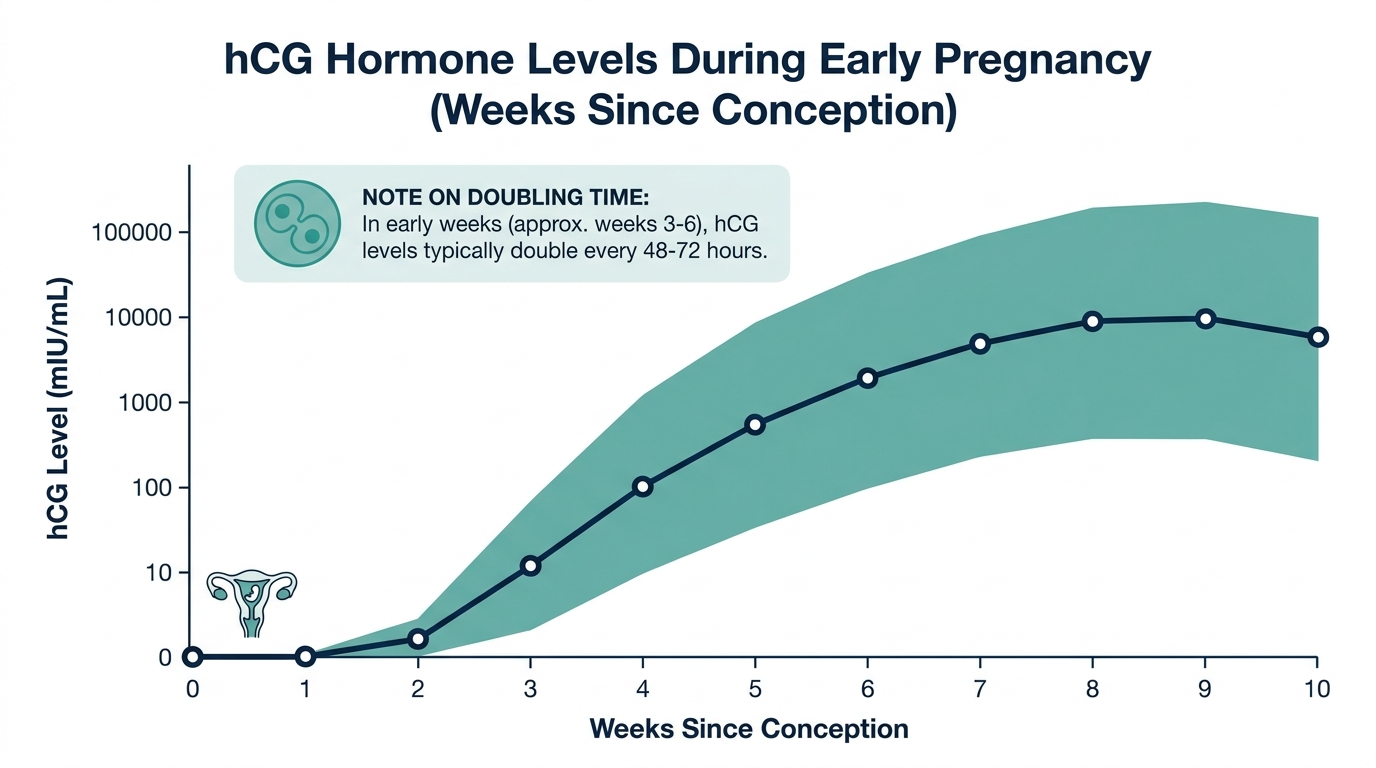
Once implantation occurs, the number climbs fast. By about the third week, hCG can run roughly 5 to 72 mIU/mL, and it keeps rising steeply through the first trimester (MedlinePlus). That early steep rise is exactly why timing is everything. Test a day or two too early, when hCG is still hovering near that 5 mIU/mL floor, and even a sensitive lab assay can read negative.
The hormone rises rapidly in the first weeks, almost doubling every three days (MedlinePlus). So a single day of patience can be the difference between a clear positive and a confusing borderline result.

Why does the exact day vary so much from person to person?
The biggest reason the timing shifts is that implantation itself does not happen on a fixed schedule. hCG production only begins once the embryo embeds in the uterine lining, and that event can occur anywhere from about 6 to 10 days after conception. Cleveland Clinic notes that the placenta starts releasing hCG roughly 11 days after the act that led to conception (Cleveland Clinic).
Layer on top of that the fact that ovulation does not always land on the textbook day 14 of a cycle. If you ovulated later than you assumed, your “days past ovulation” math is off, and a test that feels early to you is actually genuinely too early for your hormone level. This is the single most common reason an eager early blood test comes back negative in someone who turns out to be pregnant.
What is the difference between a qualitative and a quantitative blood test?
A qualitative hCG blood test answers a yes or no question, while a quantitative test reports an exact number. Both detect pregnancy, but they serve different purposes.
A qualitative hCG blood test simply checks whether the hormone is present in your blood and returns a positive or negative result, much like a home test but more sensitive (MedlinePlus). A quantitative hCG blood test, sometimes called a beta hCG, measures the precise concentration in mIU/mL (MedlinePlus).
That precise number is why the quantitative test does more than confirm a pregnancy. It can help estimate how far along you are, and it is used to investigate abnormal pregnancies including ectopic pregnancy, molar pregnancy, and possible miscarriage (MedlinePlus). If your provider wants to track whether a pregnancy is progressing normally, they will often order two quantitative draws a couple of days apart to see whether the number is doubling as expected.

The insider point: one early blood test rarely tells the whole story
Here is what experienced clinicians know that the home test box does not say. A single early hCG result, especially a low or borderline one, is often nearly meaningless on its own. What matters is the trend.
Because hCG rises steeply in early pregnancy, almost doubling every three days (MedlinePlus), the real diagnostic power of a blood test in those first uncertain days comes from comparing two draws, not from one snapshot. A value of, say, 12 mIU/mL means very different things depending on whether it was 6 two days ago or 40 two days ago. The first suggests a viable, rising pregnancy. The second suggests something is not progressing normally and deserves urgent attention.
This is also why a negative early blood test should be repeated rather than trusted as final. MedlinePlus advice for the qualitative test is explicit: if the result is negative but pregnancy is still suspected, repeat it in about a week (MedlinePlus). In other words, the earliest a blood test can detect pregnancy and the day you should fully trust a negative are not the same day. Chasing the earliest possible answer often just buys you a second test.
One more practical caution. A positive hCG is not always a confirmation of a healthy intrauterine pregnancy. The same hormone can show up with an ectopic pregnancy or certain tumors, which is why a positive result without proper implantation in the uterus still needs follow up (MedlinePlus). A number is a starting point for a conversation with your clinician, not the end of the story.
How to time an early blood test so you do not waste it
The single biggest predictor of a useful result is not the lab, it is the calendar. Because hCG only appears after implantation, and implantation can land anywhere from roughly 6 to 12 days after conception, the honest goal is to test after your hormone has had a chance to climb off the floor rather than to test as physically early as possible. Testing on day 8 past ovulation and testing on day 12 past ovulation are two very different bets, even though they feel only four days apart.
A few practical anchors help you pick the day:
- Count from ovulation, not from your last period. If you tracked ovulation with basal body temperature, an LH surge kit, or cervical mucus changes, count days past ovulation. If you only know your period date, remember that the fertile window and the true ovulation day can drift by several days in an ordinary cycle.
- Give implantation a buffer. Many people aim for around 10 days past ovulation for a blood draw, which leaves room for a slightly late implantation to still register.
- Assume you ovulated later than you think, not earlier. Late ovulation is the most common reason an early test disappoints. When in doubt, adding two or three days to your plan almost always improves the odds of a clear answer.
There is no ritual you can perform to make hCG appear before your body produces it. The value of understanding the timeline is that it turns a frustrating negative into useful information: a negative on day 8 tells you almost nothing, while a negative on day 14 after a truly known ovulation date is far more meaningful.

What can throw off an early hCG result
An hCG blood test is sensitive and specific, but a handful of situations can produce a confusing or misleading number. Knowing them ahead of time keeps you from over-reading a single result.
Reasons a test can read falsely low or negative
- Testing too early. By far the most common cause. If hCG is still hovering near the roughly 5 mIU/mL threshold, even a lab assay can read negative on one day and positive two days later.
- Later than expected ovulation. This shifts your entire timeline and is easy to miss if you assumed a textbook day 14 ovulation.
Reasons a positive can be misleading
- A very early pregnancy that does not continue. A biochemical pregnancy, also called a chemical pregnancy, is an early loss where hCG rises modestly and then falls before anything can be seen on ultrasound. This pattern is common: chemical pregnancies make up a large share of all miscarriages, and most people go on to have healthy pregnancies afterward (Cleveland Clinic).
- hCG from a source other than a healthy uterine pregnancy. A positive hCG can occur with an ectopic pregnancy or, rarely, with certain tumors, which is why a positive without confirmed implantation in the uterus still needs follow up (MedlinePlus).
- Recent fertility treatment. If you received an hCG trigger injection as part of fertility care, residual hormone from that shot can register for several days and should not be confused with a pregnancy signal. Tell your provider if this applies to you.
Unlike some panels, a standard hCG measurement does not require fasting, and ordinary foods, exercise, or hydration do not meaningfully change it. The variables that matter are timing and biology, not lifestyle on the morning of the draw.
What providers do with the number after a positive
A first positive is a starting point, not a finish line. In early, uncertain pregnancies, clinicians rely on the trend and on a well known ultrasound landmark rather than on any single value.
Two tools do most of the work:
- Serial quantitative draws. Because hCG roughly doubles every two to three days in a healthy early pregnancy, providers often repeat the quantitative test about 48 hours later. A rise in that range is reassuring; a flat, slowly rising, or falling value raises concern for an abnormal or non viable pregnancy and prompts closer evaluation.
- The discriminatory zone. This is the approximate hCG level at which a normal intrauterine pregnancy should be visible on ultrasound. With transvaginal ultrasound, that threshold is commonly cited around 1,500 to 2,000 mIU/mL. If hCG is above this range but no pregnancy is seen inside the uterus, that combination is an important flag for a possible ectopic pregnancy and warrants urgent attention.
This is exactly why chasing the earliest possible positive rarely changes what happens next. Whether your first clear positive lands on day 10 or day 13, the meaningful information comes from the second draw and, a bit later, from imaging.
When early testing matters most, and when to get help fast
For most people with no risk factors, a day or two of difference in when a pregnancy is confirmed changes very little. There are, however, situations where testing early and acting on the result genuinely matters:
- A history of ectopic pregnancy. Early confirmation lets your provider track the location and the hCG trend before symptoms develop.
- Fertility treatment or recurrent loss. Serial hCG values are often part of the plan, and early baselines make the trend interpretable.
- Medication or imaging decisions. If you are about to start a medication or have a scan that is unsafe in pregnancy, an early answer protects the pregnancy.
Regardless of what your number says, certain symptoms are red flags that should never wait for the next scheduled test. Seek care promptly for severe or one sided lower abdominal or pelvic pain, heavy vaginal bleeding, shoulder tip pain, dizziness or fainting. In an early pregnancy these can signal an ectopic pregnancy, which is a medical emergency. A reassuring hCG number does not cancel out worrying symptoms; when the two disagree, the symptoms win.
Common misconceptions about early blood pregnancy tests
A few beliefs come up again and again in clinics, and each one can lead to unnecessary worry or false reassurance.
- “A blood test can confirm pregnancy the day after sex.” It cannot. hCG does not exist in your blood until after implantation, which is typically about a week or more after conception. There is nothing to detect before then, no matter how sensitive the assay.
- “A higher hCG number means a healthier or further along pregnancy.” A single value is a poor stand-in for how far along you are, because the normal range at any given day is wide and overlaps heavily between people. Two healthy pregnancies at the same stage can have very different numbers. The trend across two draws is far more informative than one figure.
- “A faint or low first result is bad news.” Not on its own. A low value simply may mean you tested early. What matters is whether it climbs appropriately on a repeat draw.
- “A negative blood test rules out pregnancy for good.” A single early negative does not. If your period does not arrive and you still suspect pregnancy, the standard advice is to repeat testing in about a week (MedlinePlus).
- “Twins always show a dramatically higher hCG.” Multiples can be associated with higher levels, but the overlap with singleton pregnancies is large enough that hCG alone cannot confirm twins. That answer comes from ultrasound, not a blood number.
The throughline behind all of these is the same lesson experienced clinicians keep coming back to: one early number is a snapshot, and pregnancy in its first days is a moving picture. Timing, repetition, and imaging together tell the real story, and any single result is best read as one frame, not the whole film.
Questions people ask most about early blood pregnancy testing
The first question is almost always whether a blood test can confirm pregnancy before a missed period. It can, because a lab can measure hCG in the single digits while a home urine strip needs a higher concentration to turn positive. In practice that buys you a few days, sometimes enough to get an answer before you would normally think to test. The catch is that the earliest a test can turn positive and the point where you can fully trust a negative are not the same moment, so a very early negative is a reason to retest rather than a final answer.
People also ask whether a blood test can be wrong. False positives are uncommon but possible, usually from certain medications that contain hCG, recent pregnancy loss, or rare conditions that produce the hormone. False negatives are more often a timing problem than a lab error: the blood was drawn before hCG had climbed high enough to register. When the result does not fit the clinical picture, providers repeat the test rather than accept a single reading, which is why one number is treated as a starting point rather than a verdict.
Another frequent question is how long the results take. A qualitative blood test, which simply answers yes or no, often comes back the same day or within a day. A quantitative test that reports the exact hCG concentration can take a little longer depending on the lab, and it is the version used when a provider wants to track whether the number is rising as expected across repeat draws. Knowing which test was ordered tells you what kind of answer to expect and how soon.
Cost, access, and how the results actually reach you
A home urine test is inexpensive, sold over the counter, and gives you a private answer in minutes on your own bathroom schedule. A blood test is a different kind of tool. It requires a provider order in most settings, a trip to a clinic or lab for the draw, and a wait for results to be processed and reported. That extra effort is the tradeoff for its earlier detection and, in the quantitative form, its exact number. For most people confirming an expected pregnancy after a missed period, the home test is genuinely the practical first step, and the blood test earns its place when timing is urgent or when a provider needs to track the number.
The situations where the added cost and effort clearly pay off are specific. If you are undergoing fertility treatment, a clinic will typically schedule a quantitative blood test on a set day and follow it with repeat draws, because the trend guides the next decision. If there is a history of ectopic pregnancy or miscarriage, or if you have symptoms like one sided pelvic pain or unusual bleeding, the exact number and its rate of change carry information a yes or no strip cannot provide. In those cases the blood test is not just an earlier version of the home test, it is answering a different and more detailed question.
However the test is run, results are meant to be read with a provider rather than in isolation. A quantitative hCG value only becomes meaningful next to your dates, your symptoms, and often a second draw or an ultrasound. That is why even a clear positive on an early blood test is usually the beginning of a short sequence of checks, not the end of the story, and why the person ordering the test is the right one to interpret what the number means for your particular situation.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
How soon can you detect pregnancy with a blood test?
Usually about 10 days after ovulation, and within roughly 7 to 10 days after conception, because blood tests are more sensitive than urine tests and can pick up very small amounts of hCG (Cleveland Clinic). The exact day depends on when implantation happens.
Is a blood test more accurate than a home pregnancy test?
A blood test is more sensitive and can detect pregnancy earlier, often before a missed period, while home urine tests reach about 97 to 99 percent accuracy a week or two after a missed period (MedlinePlus). Both are reliable when done at the right time.
What hCG level confirms a pregnancy?
In a person who is not pregnant, hCG is generally below 5 mIU/mL, and levels rise to roughly 5 to 72 mIU/mL by about the third week of pregnancy and climb steeply from there (MedlinePlus). A rising trend across two draws is more telling than a single value.
Can a blood test be negative and you still be pregnant?
Yes, if it is done too early, before hCG has risen above the detection threshold, especially if you ovulated later than expected. If a result is negative but pregnancy is still suspected, the test should be repeated in about a week (MedlinePlus).
What is the difference between qualitative and quantitative hCG tests?
A qualitative test gives a positive or negative answer, while a quantitative test measures the exact hCG level in mIU/mL and can help estimate gestational age and flag abnormal pregnancies such as ectopic or molar pregnancy (MedlinePlus).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


