
You had a possible exposure, the worry set in, and now you are staring at a calendar trying to figure out the one thing that actually matters: when a blood test will tell you the truth. Here is the part that trips most people up. There is no single answer, because there are three very different HIV blood tests, and each one wakes up at a different point after infection. Test too early on the wrong one and a negative result means almost nothing.
Worried about timing after a possible exposure? Once you’re past the window, see your full health picture too. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
The good news is that the timelines are well defined, and once you understand which test detects what, the anxiety gets a lot more manageable. Let us walk through it the way a clinician actually thinks about it.
How soon can HIV be detected by a blood test?
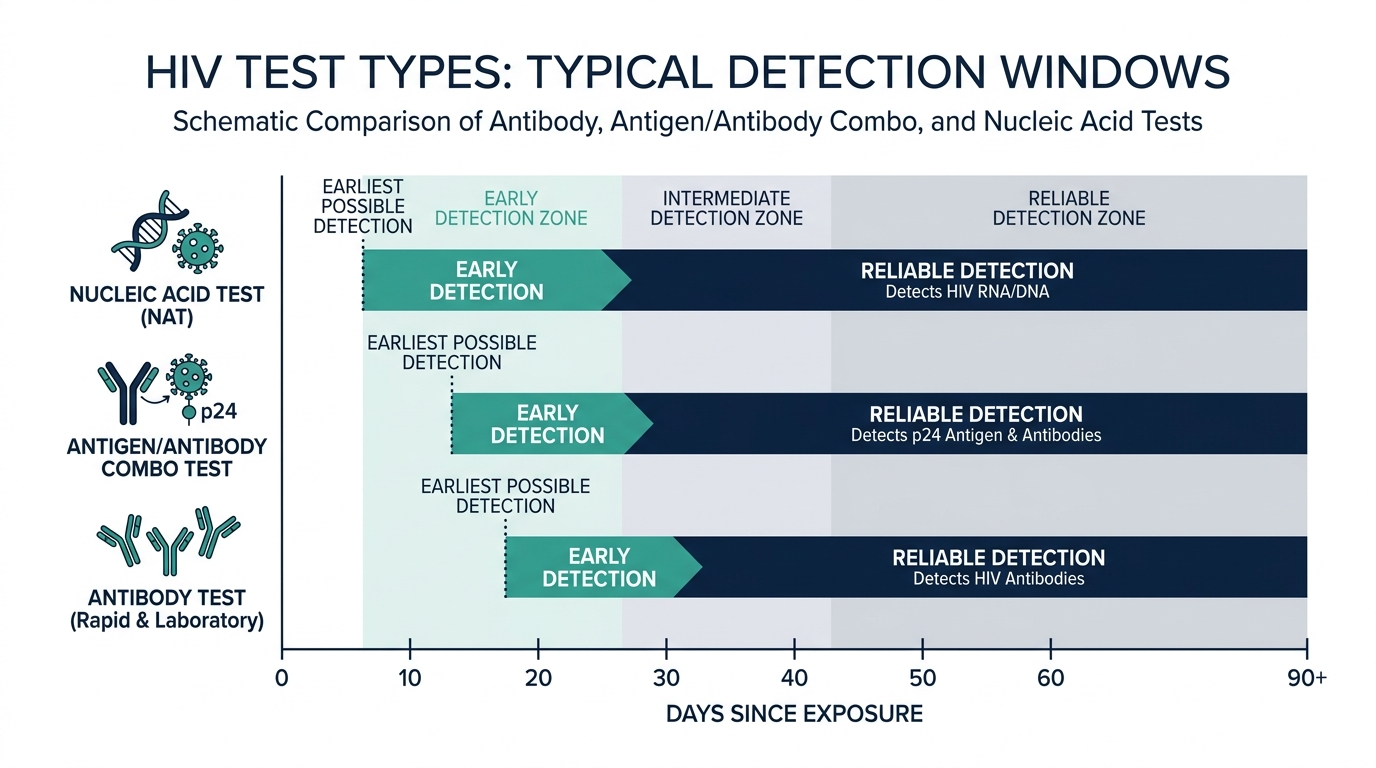
How soon HIV can be detected by a blood test depends entirely on which test you take. The earliest detection comes from a nucleic acid test (NAT), which can usually find HIV roughly 10 to 33 days after infection. A laboratory antigen/antibody (Ag/Ab) blood test, drawn from a vein, typically detects HIV about 18 to 45 days after exposure. A pure antibody test, including most rapid and at-home kits, can take anywhere from 23 to 90 days (MedlinePlus).
That gap between exposure and reliable detection has a name: the window period. It is the stretch of time when you may already carry HIV but the virus, or your body’s response to it, has not yet built up to a level the test can register (Cleveland Clinic). The whole game of HIV testing is knowing where you are inside that window.

What is the HIV window period?
The window period is the gap between the moment you are exposed to HIV and the moment a given test can actually detect it. No test can find HIV the day after exposure, because the virus needs time to multiply and your immune system needs time to react (Cleveland Clinic). During this gap, you can be infected and still get a negative result.
Think of it like a footprint in fresh snow. Right after the step, there is barely a mark. Give it a moment and the impression deepens until it is unmistakable. HIV testing works the same way. The marker each test hunts for has to accumulate before the test can call it.
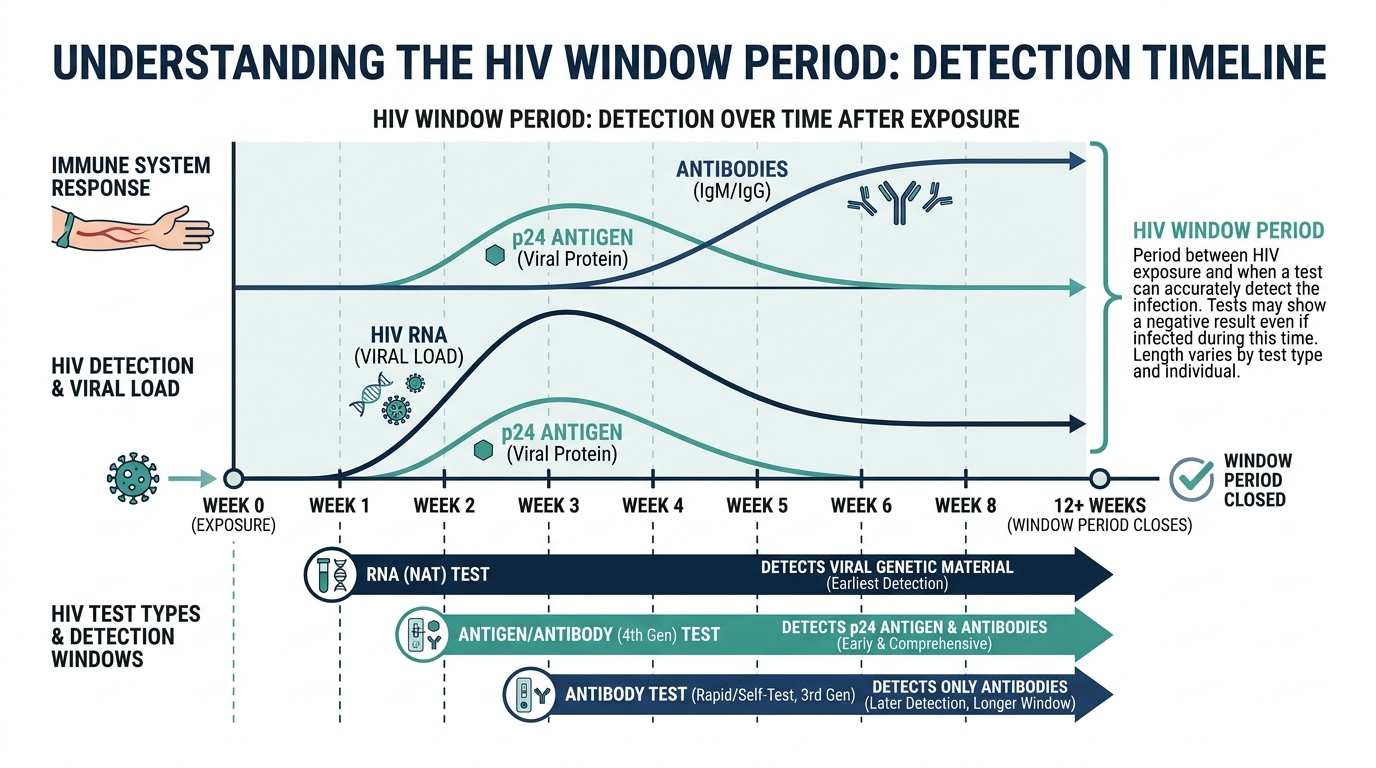
What is being measured shifts over time, and that is why the three test types have such different timelines. First the virus itself appears in the blood as genetic material (RNA). Next comes a viral protein called the p24 antigen. Last, your immune system produces antibodies. Each test targets a different one of these signals, and they show up in that order (StatPearls, NCBI).
What are the three types of HIV blood tests?
There are three blood tests for HIV, and they differ in what they look for and how early they catch infection. Knowing which one you are getting is the single most useful thing for interpreting a result.
- Nucleic acid test (NAT). This looks directly for HIV genetic material (RNA) in blood drawn from a vein. It is the earliest detector, finding infection around 10 to 33 days after exposure, but it is expensive and not used for routine screening (MedlinePlus).
- Antigen/antibody (Ag/Ab) combination test. The current standard fourth-generation test. It detects both the p24 antigen and HIV antibodies. From a lab blood draw it finds infection about 18 to 45 days out; from a finger-prick rapid version it can stretch to 18 to 90 days (Cleveland Clinic).
- Antibody-only test. Most rapid tests and at-home kits fall here. They detect only antibodies, which appear last, so the range is 23 to 90 days after exposure (MedlinePlus).
The takeaway is simple. The closer a test gets to the virus itself, the earlier it can detect infection. NAT looks at the virus, the Ag/Ab test looks at an early viral protein plus antibodies, and the antibody test waits for your slowest signal.

Why does each HIV test detect infection at a different time?
Each test detects infection at a different time because each one targets a different biological signal, and those signals appear in a fixed sequence after infection. Detection speed simply follows the order in which the markers show up in your blood (StatPearls, NCBI).
Right after transmission there is a brief stretch, sometimes called the eclipse phase, where even sensitive tests find nothing. Then HIV RNA becomes detectable first, as early as 5 to 10 days after transmission in some cases, which is why a NAT can call infection so early (StatPearls, NCBI). The p24 antigen, a protein from the virus’s core, can appear roughly two weeks after exposure, and that is what lets a fourth-generation Ag/Ab test catch infection sooner than an antibody test (StatPearls, NCBI). Antibodies, your immune system’s response, take longest, and most people will test positive on a fourth-generation assay within about three weeks while some do not seroconvert for up to three months (StatPearls, NCBI).
So the difference is not random. RNA, then antigen, then antibody. A test is only as fast as the marker it is built to find.
What does a negative HIV test mean during the window period?
A negative HIV test during the window period does not reliably rule out infection. It can mean you do not have HIV, or it can mean the test was done too soon for the marker to show up yet (MedlinePlus). This is the most misunderstood point in all of HIV testing, and it is where people get falsely reassured.
The practical rule is to match the test to the timeline. If you test before the window for that specific test has closed, a negative result needs to be confirmed with a repeat test after enough time has passed. For a standard antigen/antibody test, that usually means retesting at around 45 days, and for an antibody-only test, retesting out to 90 days to be confident (Cleveland Clinic).
If you had a recent high-risk exposure and want the earliest possible answer, a NAT is the test that can give it, because it does not wait for your antibody response (MedlinePlus). That said, a single early negative still warrants a follow-up screen, because the very earliest days can fall inside even the NAT window.

The part most people miss: catching acute HIV before antibodies appear
Here is the insider point that changes how clinicians approach a fresh exposure. The most dangerous moment, both for the individual and for transmission, is acute HIV infection, the first few weeks when the virus is multiplying explosively and the blood is highly infectious, yet antibodies have not formed. An antibody-only test taken in this window will read negative even though the person is profoundly contagious.
This is precisely why the testing strategy matters more than the test result. When acute infection is suspected within the first two weeks after exposure, the right first move is an HIV RNA (NAT) test rather than a standard antibody screen, because viral RNA shows up before antibodies do (StatPearls, NCBI). Clinicians also learn to read mononucleosis-like symptoms, fever, sore throat, swollen glands, and rash after a possible exposure, as a flag to order viral load testing instead of relying on a single antibody result (PMC, acute HIV during the window period).
The numbers back this up at the population level. When researchers added pooled nucleic acid testing to a fourth-generation antigen/antibody algorithm, they detected 38 percent more acutely infected people than the antigen/antibody test caught on its own (PubMed, NAT versus Ag/Ab for acute HIV). That is the gap a savvy clinician is trying to close. A negative rapid test after a recent exposure is not a clean bill of health. It is a reason to ask which test you took and whether the timing was right.
PEP: the 72-hour window that runs alongside the testing window
Before you fixate on when to test, there is an earlier clock that matters even more after a genuine high-risk exposure. Post-exposure prophylaxis, known as PEP, is a short course of HIV medication that can stop an infection from taking hold if you start it fast enough. The rule is blunt: PEP is unlikely to work if you begin it more than 72 hours after exposure, and the sooner you start inside that window, the better (CDC).
Here is what most people never connect. The 72-hour PEP window opens the moment you are exposed, long before any test can detect infection. So if you are counting days to your first blood test, you have already missed the window that could have prevented the infection in the first place. That is why clinicians treat a recent high-risk exposure as an emergency, not a scheduling question.
- Timing. Start within 72 hours of exposure. Go to an emergency room, urgent care, or sexual health clinic the same day. Do not wait for symptoms and do not wait for a test.
- Duration. PEP is taken every day for 28 days. Skipping doses lowers its protection, so adherence for the full course matters (NIH HIVinfo).
- Effectiveness. Observational research suggests PEP can reduce the risk of acquiring HIV by more than 80 percent when started promptly and taken correctly (CDC).
One important wrinkle for testing: if you take PEP, it can delay your seroconversion and push your window period out. After finishing a 28-day PEP course, follow-up HIV testing is typically extended, so plan on retesting further out than the standard timelines. Tell whoever runs your test that you were on PEP, because it changes how they interpret an early negative.

What can lengthen or shorten your personal window period?
The ranges you see quoted, 10 to 33 days, 18 to 45 days, 23 to 90 days, are population estimates, not a promise about you specifically. Where you land inside that range depends on several factors, and knowing them helps you decide when a negative result is trustworthy.
- The route and size of exposure. A larger viral inoculum, such as a needle-stick with fresh blood, can lead to faster viral replication and earlier detection than a lower-risk exposure. This is not something you can measure at home, but it is one reason clinicians ask exactly what happened.
- PEP or PrEP use. Any antiretroviral medication in your system slows viral replication, which can blunt the antigen and antibody signals and stretch your window period. This is the single most common reason a test comes back negative later than expected.
- Your immune response. Some people mount a fast, strong antibody response and seroconvert in two to three weeks; others take the full three months. There is normal person-to-person variation in how quickly antibodies build.
- The specimen type. A finger-prick or oral-fluid rapid test generally detects infection later than the same generation of test run on blood drawn from a vein, because the marker concentration is lower in those fluids (CDC).
The practical lesson: if any of these apply to you, especially recent antiretroviral use, treat the longer end of the range as your real deadline for a confident negative.
At-home and rapid tests: what they detect and what they miss
At-home HIV tests are a genuine advance for access, but they trade a little detection speed for convenience, and understanding that trade-off prevents false reassurance. Most at-home kits and many clinic rapid tests are antibody-only tests, which means they detect your slowest signal and carry the widest window, up to 90 days (MedlinePlus).
There are two broad kinds of at-home testing:
- Rapid self-tests use oral fluid or a finger-prick drop and give a result in about 20 minutes. They are antibody tests, so a negative in the first few weeks after exposure means little. Their strength is that a person who would never visit a clinic will test at home.
- Mail-in collection kits let you collect a dried blood spot from a finger-prick and mail it to a lab, where a more sensitive antigen/antibody or nucleic acid test may be run. These can detect infection earlier than an oral rapid test because a lab is doing the analysis.
A crucial rule for all self-testing: a positive or reactive result at home is not a diagnosis. It is a preliminary result that must be confirmed with laboratory testing, because rapid tests can occasionally produce a false reactive result. A reactive home test means you go get a confirmatory lab test, not that you have HIV.
How labs confirm a positive result: the testing algorithm
A single reactive test never stands alone in modern HIV diagnosis. Laboratories follow a stepwise algorithm designed to catch both false positives and very early infection, and understanding it explains why you might get a call back for more testing even after an initial reactive screen (StatPearls, NCBI).
- Initial screen. A fourth-generation antigen/antibody test is run first. If it is nonreactive and you are past the window, testing usually stops there.
- Differentiation test. If the screen is reactive, a second test distinguishes HIV-1 from HIV-2 antibodies. This confirms and classifies the infection.
- Nucleic acid test as tie-breaker. If the screen is reactive but the antibody differentiation test is negative or indeterminate, that pattern suggests very early, acute infection where antibodies have not fully formed. A NAT is run to look directly for the virus. A positive NAT here confirms acute HIV.
This is why the phrase “my test was positive” is not the end of the story. The algorithm exists precisely so that a single reactive result, which can happen for benign reasons, is not treated as a diagnosis until it is confirmed.
Acute HIV symptoms and when to seek care immediately
During acute infection, many people develop a flu-like or mononucleosis-like illness as the immune system reacts to a surge of virus. Recognizing this pattern after a possible exposure is one of the strongest reasons to seek early testing, because it can prompt a NAT before antibodies would ever show up. Commonly reported symptoms include fever, sore throat, swollen lymph nodes, a rash, muscle and joint aches, mouth ulcers, and night sweats.
These symptoms are nonspecific, meaning they overlap with many ordinary viral illnesses, so they cannot diagnose HIV on their own. What matters is the combination: a compatible symptom picture in the two to four weeks after a genuine exposure. Treat the following as reasons to seek care quickly rather than waiting out a testing timeline:
- Flu-like symptoms appearing one to four weeks after a known high-risk exposure.
- A recent exposure where you are still inside the 72-hour PEP window, regardless of symptoms.
- A reactive home or rapid test result that needs laboratory confirmation.
- Repeated high-risk exposures, where ongoing screening rather than a single test is the right approach.
Who should test, how often, and what happens after a positive result
HIV testing is not only for people who think they had a single risky moment. Routine screening catches infections that would otherwise go undiagnosed for years, and the guidance is broader than most people assume. Public health bodies recommend that everyone between roughly 13 and 64 be tested at least once as part of routine care, with more frequent testing for those at higher ongoing risk (CDC).
A reasonable framework:
- At least once for all adolescents and adults as a baseline.
- At least once a year for people with ongoing risk factors, including those with multiple partners or partners of unknown status, and people who inject drugs.
- More often, every three to six months, for people at high ongoing risk, which is also the interval used to monitor people taking PrEP.
If a confirmed positive result comes back, the modern reality is very different from decades past. HIV is now a manageable chronic condition. Starting antiretroviral therapy promptly can suppress the virus to undetectable levels, which both protects your own long-term health and, when the viral load stays undetectable, means the virus is not transmitted to sexual partners. The next step after a positive result is linkage to an HIV care provider, not panic. Early diagnosis is precisely what makes those outcomes possible, which loops back to the whole point of understanding the window period: testing at the right time so a real infection is not missed.
Turn what you just learned into action.
Superpower lets you test 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
How soon can HIV be detected by a blood test after exposure?
It depends on the test. A nucleic acid test (NAT) can usually detect HIV 10 to 33 days after exposure, a lab antigen/antibody blood test about 18 to 45 days, and an antibody-only test 23 to 90 days (MedlinePlus). The NAT detects infection earliest because it looks for the virus directly.
Can an HIV test be negative and still be wrong?
Yes, if it is done during the window period. A negative result can mean you are not infected or that it is simply too soon for the test to detect HIV (MedlinePlus). That is why a negative test taken soon after a possible exposure should be repeated after the window closes.
What is the earliest HIV test available?
The nucleic acid test (NAT) is the earliest, detecting HIV RNA roughly 10 to 33 days after exposure, and sometimes sooner in acute infection (Cleveland Clinic). It is more expensive than standard tests and is usually reserved for recent high-risk exposures or confirming early infection.
When should I retest after a negative HIV result?
If you tested during the window period, retest after enough time has passed for your test type. A standard antigen/antibody test is typically repeated around 45 days, and an antibody-only test out to 90 days for confidence (Cleveland Clinic).
Why do antibody tests take longer than other HIV tests?
Antibodies are the last marker to appear after infection. Viral RNA shows up first, then the p24 antigen, and only later does your immune system make enough antibodies to register, which can take up to 90 days (StatPearls, NCBI).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


