
You felt a vague worry, asked your doctor for “everything,” and walked out with a blood draw. Now you are staring at the results wondering the obvious thing: if cancer were hiding in there, would this catch it? It is one of the most common questions in oncology, and the honest answer is more layered than either “yes, of course” or “no, never.”
One blood test alone rarely spots cancer. Want a broader panel that screens for early warning signs? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Blood can carry real fingerprints of cancer. It also stays stubbornly quiet in many cases, and a clean panel can lull you into a false sense of safety. Here is what your blood can and cannot tell you, written the way a clinician would actually explain it.
Can cancer be identified with a blood test?
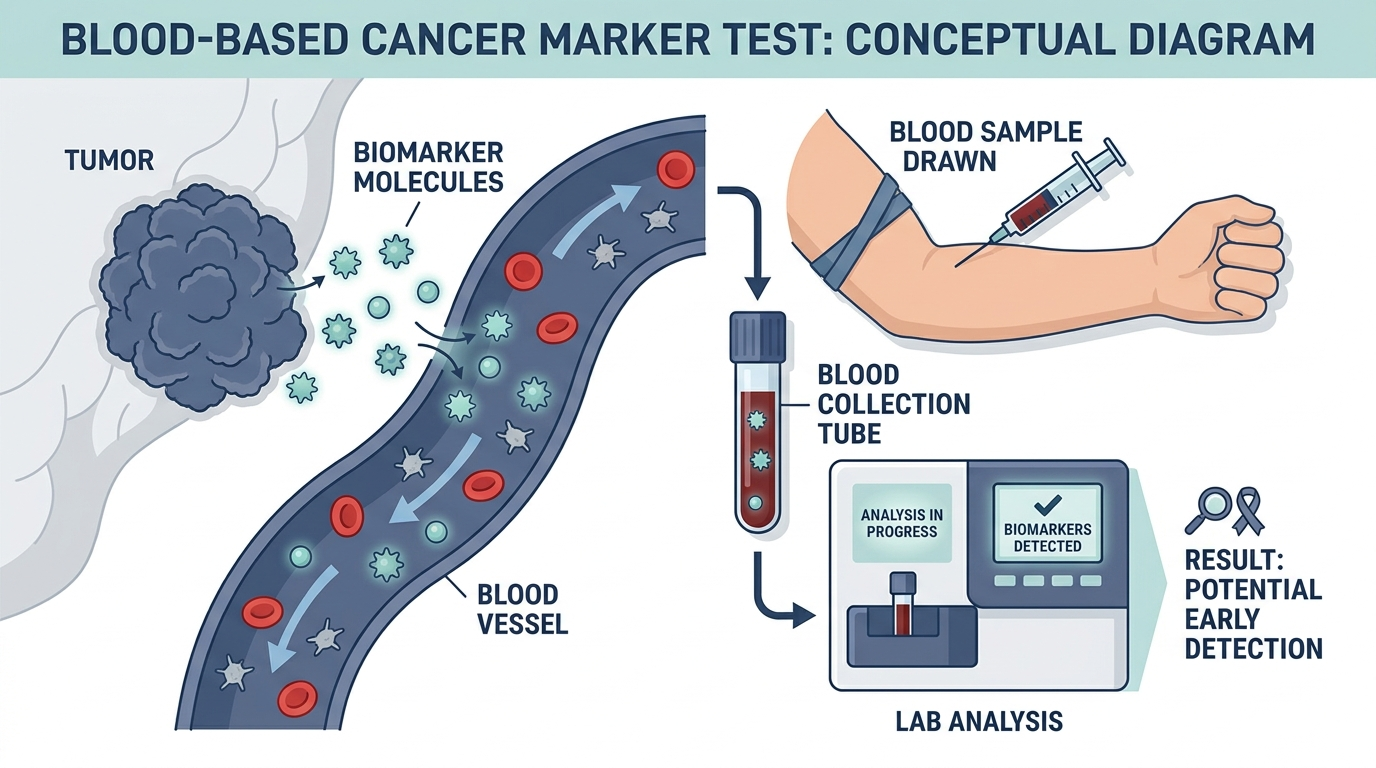
Sometimes, but rarely on its own. A blood test can raise a strong suspicion of cancer and can flat out diagnose certain blood cancers, but for most solid tumors it cannot deliver a diagnosis by itself. As Cleveland Clinic puts it plainly, blood work alone cannot detect most types of cancer, and a confirmed diagnosis usually needs imaging and a biopsy on top of the labs (Cleveland Clinic).
So the better way to frame “can cancer be identified with blood test” is this: blood tests are excellent at flagging that something may be wrong and at narrowing the search, but the actual identification of a solid cancer almost always happens under a microscope, on a tissue sample. The blood gets you to the door. The biopsy opens it.

What kinds of blood tests are used for cancer?
There are four broad categories, and they do very different jobs. Lumping them together is exactly how people end up confused about whether a blood test “found” their cancer.
- Complete blood count (CBC). This counts your red cells, white cells, and platelets. It can directly point to blood cancers like leukemia and lymphoma, but it cannot detect solid organ cancers such as lung, breast, or colon cancer (Cleveland Clinic).
- Tumor marker tests. These measure substances made by cancer cells or by normal cells reacting to cancer. Familiar examples include PSA for prostate, CA-125 for ovarian, CEA for colorectal, and AFP for liver (MedlinePlus).
- Blood protein tests. These look for abnormal proteins, which are especially useful for blood cancers like multiple myeloma (Cleveland Clinic).
- Circulating tumor cell and liquid biopsy tests. These hunt for whole tumor cells or fragments of tumor DNA shed into the bloodstream (Cleveland Clinic).
The key distinction: blood cancers live in the blood, so blood tests can catch them directly. Solid tumors sit in an organ, and the blood only carries indirect clues they leave behind.
Can a blood test identify cancer in the blood, like leukemia?
Yes, and this is where blood testing shines. Cancers of the blood and bone marrow, such as leukemia, lymphoma, and multiple myeloma, often show up directly on a routine CBC because the abnormal cells are circulating where the test looks (Cleveland Clinic). An unexplained sky-high white cell count, a strange population of immature cells, or abnormal proteins can be the first hard signal.
That said, even here the CBC rarely closes the case alone. To confirm and subtype a blood cancer, doctors typically follow up with a bone marrow biopsy and specialized lab studies. The CBC is the alarm. The marrow exam is the verdict.
What are tumor markers, and why are they not a screening test?
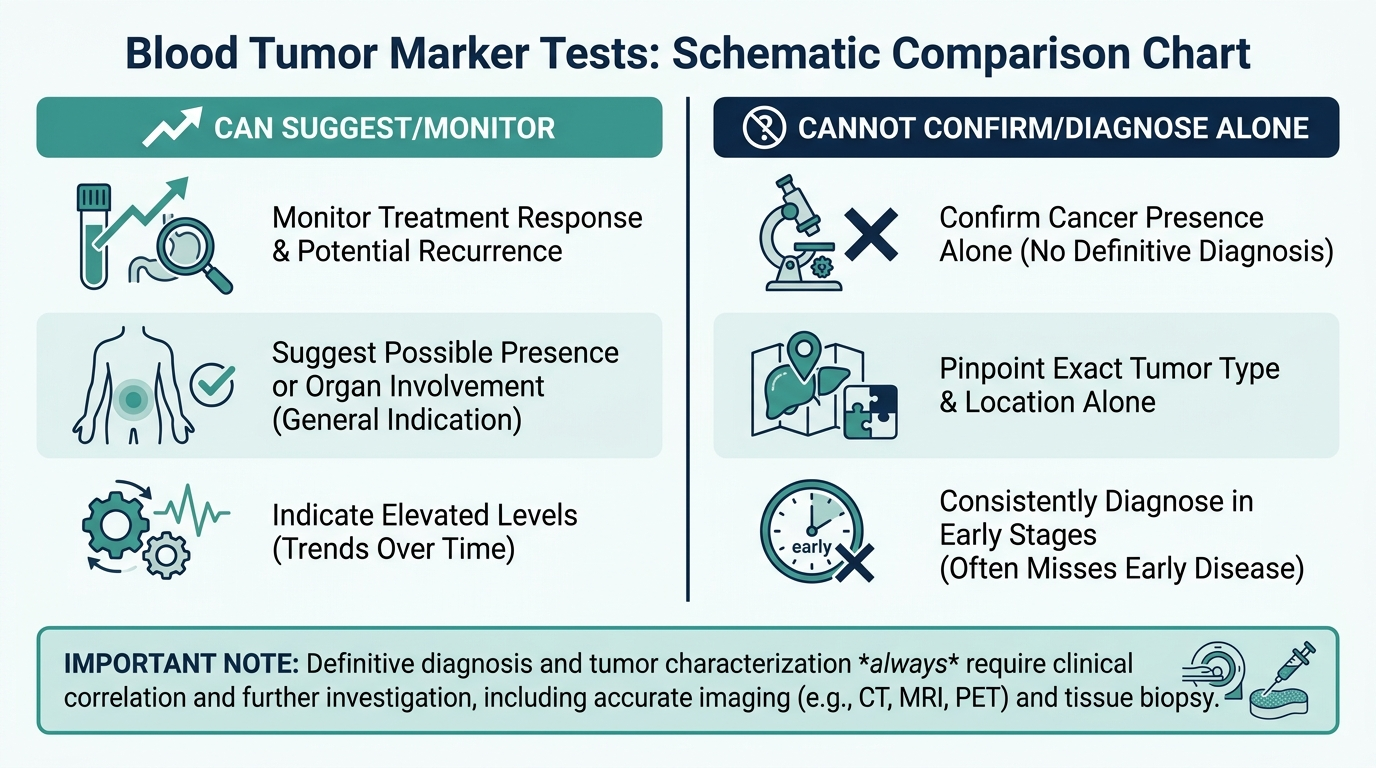
Tumor markers are substances that can rise when cancer is present, but they are poor tools for screening healthy people. A high level only means cancer is more likely, not that you have it, and a normal level does not rule cancer out (MedlinePlus). They are most often used after a diagnosis, to monitor whether treatment is working or whether a cancer has come back, rather than to find cancer in the first place.
The problem is twofold. Tumor markers are not sensitive enough, so they miss many true cancers, and they are not specific enough, so noncancerous conditions can push them up and trigger false alarms (National Cancer Institute). CA-125, for example, can rise from endometriosis, fibroids, or even normal menstruation, none of which is cancer. That is why a single elevated marker in an otherwise healthy person sets off a hunt rather than a diagnosis.

Can cancer be identified in a blood test before symptoms appear?
Increasingly, yes, and this is the most exciting frontier. A newer class of tools called multi cancer early detection (MCED) tests, sometimes called liquid biopsies, scan a single blood sample for tiny fragments of tumor DNA. Because tumors shed these fragments into the circulation early, these tests can in principle detect cancer before you have symptoms and before a tumor is large enough to show up on imaging (PMC, early cancer detection blood tests).
The performance can be striking in research settings. One study reported a blood test detecting cancer up to four years before a clinical diagnosis with high sensitivity in the samples tested (PMC, early cancer detection blood tests). MCED tests have flagged signals in people later diagnosed with cancers of the ovary, kidney, and head and neck, cancers that currently have no recommended screening test at all (PMC, MCED detects cancers lacking standard screening). That is genuinely new. For the first time, a blood draw can hint at cancers we previously had no easy way to look for.
The part most people miss: a normal blood test does not mean no cancer
This is the single most important thing to internalize, and it is the trap that catches smart, careful people. Most early solid tumors do not move your standard blood work at all. You can have a completely normal CBC and a normal chemistry panel and still have an early breast, lung, or colon cancer growing quietly.
Here is the clinician’s mental model. Routine blood tests are built to catch derangements in your blood and organ function, not to spot a small lump in an organ. By the time many solid cancers reliably disturb the bloodstream, they are no longer early. So a clean panel is reassuring about your blood and organs in the moment. It is not a cancer all clear.
Even the new MCED tests carry the same caveat in reverse. They can miss cancers (a negative result is not a guarantee), and they can flag a signal that turns out to be nothing, sending people down a stressful and expensive cascade of scans and procedures (PMC, early cancer detection blood tests). They are promising, but they do not yet replace the screening tests proven to save lives, such as mammograms, colonoscopy, and low dose CT for high risk smokers. This is why Mayo Clinic and others stress that cancer blood tests are used alongside, not instead of, imaging and biopsy (Mayo Clinic).
The practical takeaway: if you have a worrying symptom, do not let a normal blood test talk you out of getting it looked at. The blood being fine and the organ being fine are two different questions.
Common tumor markers and what each is actually used for
Because tumor markers are so often misunderstood, it helps to see the main ones side by side, along with the noncancerous conditions that can raise them. The recurring theme is that almost every marker can climb for benign reasons, which is exactly why none is a standalone screening test.
| Marker | Most associated with | Typical use | Can also rise from |
|---|---|---|---|
| PSA | Prostate | Screening in some men, monitoring known prostate cancer | Benign prostate enlargement, prostatitis, recent ejaculation |
| CA-125 | Ovarian | Monitoring known ovarian cancer, workup of a pelvic mass | Endometriosis, fibroids, menstruation, pregnancy |
| CEA | Colorectal | Monitoring treatment and recurrence | Smoking, inflammatory bowel disease, liver disease |
| AFP | Liver, some testicular | Diagnosis support and monitoring in specific cancers | Pregnancy, hepatitis, cirrhosis |
| CA 19-9 | Pancreatic | Monitoring known pancreatic cancer | Bile duct blockage, pancreatitis, liver disease |
Notice that most of these appear in the monitoring column, not the screening column. That placement is the whole point. Tumor markers earn their keep after a diagnosis, tracking whether a cancer is responding to treatment or returning, far more than they help find a cancer in someone who feels well. PSA is the partial exception, used in shared-decision screening for prostate cancer, and even it carries a well-known risk of false alarms.

Indirect blood clues doctors watch for
Even though standard blood work cannot see a solid tumor, certain patterns can act as smoke that prompts a search for fire. None of these proves cancer, but a clinician takes them seriously, especially when unexplained.
- Unexplained anemia: a low red blood cell count with no obvious cause, particularly iron-deficiency anemia in a man or a postmenopausal woman, can prompt a look for a slow bleed from a gastrointestinal cancer.
- High calcium: some cancers raise blood calcium, so an unexplained elevation can be part of a cancer workup.
- Abnormal liver enzymes: a rise can reflect many things, but in the right context it can signal that cancer has spread to the liver.
- Elevated LDH: this general marker of cell turnover is nonspecific, but it can be part of the picture in lymphoma and other cancers.
- Abnormal blood cell counts or proteins: a strange white cell population, very high or low counts, or abnormal proteins can point toward a blood cancer directly.
The consistent message is that these are clues, not conclusions. Each has many benign explanations, and the value lies in the pattern plus your symptoms, which is what guides the next test rather than any single number.
How doctors work up a suspicious blood result
Understanding the sequence removes a lot of fear when a result comes back abnormal. Clinicians move in deliberate steps rather than jumping to the worst case.
- Repeat and confirm: a single abnormal value is often rechecked, since lab variation and temporary conditions are common causes.
- Put it in context: the clinician weighs your age, symptoms, family history, and the rest of your labs before deciding anything is worrying.
- Targeted imaging: if suspicion is real, imaging such as ultrasound, CT, MRI, or a mammogram looks at the organ in question.
- Biopsy for confirmation: for a solid tumor, a tissue sample examined under a microscope provides the definitive answer, because only tissue reveals whether cells are truly cancerous and what type they are.
This stepwise path is why one flagged blood value rarely means what people fear in the moment. It opens an investigation, and most investigations that start with a mildly abnormal lab do not end in a cancer diagnosis.
Where multi-cancer early detection tests stand today
The multi-cancer early detection tests generating headlines are a genuine advance, but their current status deserves an honest, careful framing. As of now, these liquid biopsy screening tests are largely offered without full regulatory approval as a general screening tool, and major guideline bodies have not adopted them as a replacement for proven screening. They are being studied intensively in large trials to answer the question that ultimately matters, which is whether finding cancer signals earlier this way actually helps people live longer.
Two limitations are important to hold in mind. First, a negative MCED result does not guarantee you are cancer-free, because these tests can miss cancers, especially early or low-shedding ones. Second, a positive signal is not a diagnosis, and it can send a person through a stressful, costly cascade of scans and procedures that sometimes finds nothing. For now, the responsible way to view them is as a possible add-on to discuss with a clinician, not a substitute for the screening tests with proven mortality benefit: mammography, colonoscopy, cervical screening, and low-dose CT for eligible people with a heavy smoking history.

Who should talk to a doctor about cancer blood testing
Rather than asking for every test, the useful question is whether your situation warrants a specific conversation. Reasonable prompts include:
- Persistent, unexplained symptoms such as unintended weight loss, ongoing fatigue, a lump, unusual bleeding, or a change in bowel or bladder habits that has not resolved.
- A strong family history of a particular cancer, which may change what screening and testing make sense for you and at what age.
- Being due for a proven screening test based on age and risk, such as mammography, colonoscopy, or low-dose CT, which remain the highest-value tools.
- Curiosity about newer liquid biopsy tests, which is best explored as a shared decision that weighs the benefits, limits, and possible follow-up procedures.
The unifying principle across all of it is that blood testing supports a cancer evaluation but does not stand in for the whole of it. If you have a symptom that worries you, a normal blood panel is not a reason to wait, since the blood being fine and the organ being fine are two separate questions.
Common misconceptions that cause real harm
A few widespread beliefs about cancer and blood tests lead people to make decisions they later regret. Correcting them is some of the most valuable information in this article.
- “My blood work was normal, so I do not need that scan.” This is the most dangerous myth. Most early solid cancers do not disturb routine blood work at all, so a clean panel is not a reason to skip a mammogram, colonoscopy, or the evaluation of a persistent symptom.
- “A high tumor marker means I have cancer.” Many benign conditions raise tumor markers, and a single elevated value prompts a search, not a diagnosis. Panic here often causes more harm than the number itself.
- “A liquid biopsy can replace my regular screening.” These tests are promising but unproven as a substitute, and they can both miss cancers and raise false alarms. They may add to, but do not replace, screening with proven benefit.
- “If I just get enough blood tests, I will catch anything early.” More testing in a healthy person often produces false positives that lead to unnecessary procedures. Targeted, guideline-based screening beats a scattershot approach.
The theme running through all four is that context and proven tools matter more than volume of testing. A thoughtful conversation with a clinician about your specific risk almost always serves you better than trying to test your way to certainty.
Why tissue, not blood, delivers the final word
It is worth understanding why a biopsy remains the gold standard for most cancers, because it explains the entire structure of a cancer workup. Blood can carry indirect signals, a shed protein here, a fragment of DNA there, but those signals cannot show a pathologist the one thing that defines cancer: cells growing and behaving abnormally within tissue.
A biopsy lets a specialist look directly at the cells, confirm whether they are malignant, identify the exact type, and often test them for the specific features that guide treatment. That level of detail simply is not available from a tube of blood in most cases. This is why clinicians describe blood tests as the tools that raise suspicion and narrow the search, while the biopsy is what opens the door to a definitive answer and a treatment plan. Seen this way, the two are partners in a sequence, not competitors, and each does a job the other cannot.
Where tumor markers genuinely shine: monitoring, not diagnosis
It is easy to walk away thinking tumor markers are useless because they make poor screening tests. That misses their real value. Their strength is not finding cancer in a healthy person, it is tracking a cancer that has already been diagnosed, where the same test finally becomes reliable.
Once a cancer is confirmed and a person’s marker level is known, the trend over time carries real meaning. A marker that falls after surgery or during treatment suggests the therapy is working, while a marker that starts climbing again after remission can be an early clue of recurrence, sometimes before symptoms or scans catch it. Because the comparison is now against that person’s own earlier values rather than a population range, the noise that makes markers unreliable for screening matters far less.
This reframes how to read a tumor marker result on your own report. In someone without a cancer diagnosis, a single elevated value is a prompt to look further, not a verdict, since benign conditions commonly raise these proteins. In someone under cancer care, the shape of the curve across repeated draws is what the oncology team watches. The practical takeaway is to ask what a given marker is actually being used for in your situation. Screening, monitoring, and confirming are three different jobs, and tumor markers are far better at the middle one than at the other two.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Can a routine blood test detect cancer?
Usually not by itself. A routine CBC can point to blood cancers like leukemia, but it cannot detect most solid tumors such as lung, breast, or colon cancer, and a normal result does not rule cancer out (Cleveland Clinic).
Can cancer be identified in a blood test before there are symptoms?
Newer multi cancer early detection blood tests can sometimes flag a cancer signal before symptoms appear, in some studies years before diagnosis, but they can still miss cancers and produce false alarms, so they do not replace standard screening (PMC, early cancer detection blood tests).
Are tumor markers a good way to screen for cancer?
No. Tumor markers are not sensitive or specific enough for screening healthy people. They miss many cancers and can be raised by noncancerous conditions, so they are mainly used to monitor a known cancer rather than to find one (National Cancer Institute).
If my blood test is normal, am I in the clear from cancer?
Not necessarily. Many early solid cancers do not change standard blood results at all, so a normal panel is reassuring about your blood and organ function but is not a cancer all clear. Persistent symptoms still deserve evaluation (Mayo Clinic).
What confirms a cancer diagnosis if a blood test cannot?
For solid tumors, diagnosis almost always requires imaging plus a biopsy, where a tissue sample is examined under a microscope. Blood tests help raise suspicion and narrow the search, but the biopsy provides the definitive answer (MedlinePlus).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


