
Last updated 18 June 2026. Educational content, not medical advice. Many peptides sold online are labeled “for research use only” and are not approved for human use. Talk to a licensed clinician before starting anything.
Short answer: In 2026, a legitimate peptide therapy program through a telehealth clinic runs roughly $150 to $400 a month for most single peptides, with the medication, a prescribing clinician, and follow-up usually bundled in. Sermorelin sits around $175 to $225 a month, a CJC-1295/ipamorelin stack around $325 for a five-week supply, NAD+ injections $150 to $400 a month, and a general BPC-157 or peptide-therapy program $200 to $500 a month. On top of that, budget $150 to $400 for baseline labs before your first dose. Grey-market “research” vials look far cheaper at $30 to $120, but that price is missing everything that makes the therapy safe, and none of it, in any lane, is covered by insurance.
Curious what a peptide protocol is actually doing inside your body? See your own hormone and metabolic markers first. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
That is the number most people came for. The rest of this page is the part the clinic pricing pages and the vendor checkout buttons both leave out: what you are actually paying for in each lane, where the cheap number hides its real cost, and why the gap between a $60 vial and a $300 program is mostly invisible until something goes wrong.
What is the real all-in cost of peptide therapy?
Here is the thing nobody frames correctly. The monthly subscription number is not the cost of peptide therapy. It is the cost of the medication plus part of the service. The true first-year number includes intake, baseline bloodwork, the peptide itself, the supplies, and follow-up labs, and those pieces are split across different invoices on purpose so each one looks small.
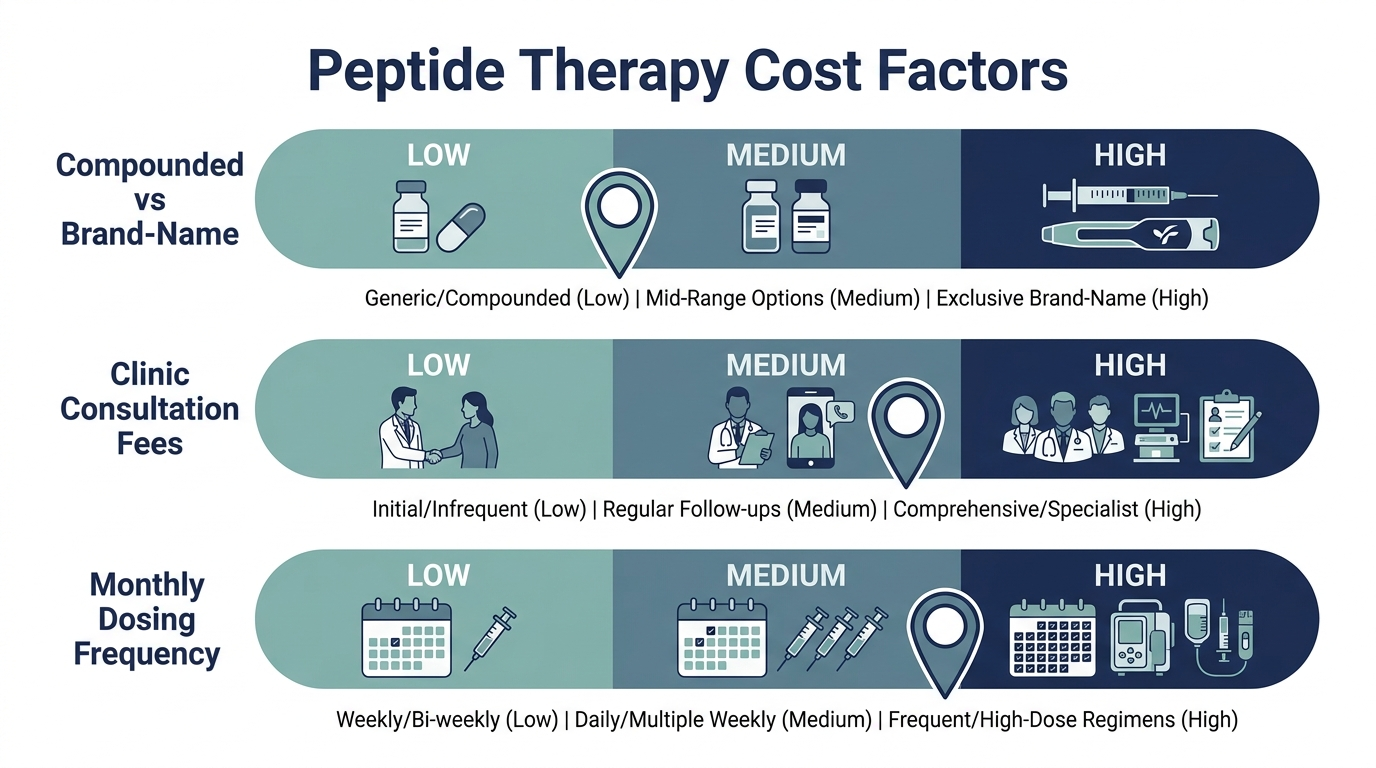
A realistic first six months on a mid-range clinic program lands around $1,900 to $3,200 all-in (PeakedLabs). That breaks down to roughly a $150 to $400 initial consult, $100 to $250 in baseline labs, $200 to $500 a month in medication, and periodic monitoring check-ins at $75 to $200 each.
Compare that to the grey-market math people quote in forums: a $40 to $150 four-week course of a research vial, supplies included (PeakedLabs). On a spreadsheet the gap is enormous. In reality you are comparing a finished, supervised therapy to a freeze-dried powder you reconstitute yourself with no one accountable for the dose. They are not the same product, and pretending they are is how people end up injecting something they never verified.
Full-body lab membership: 100+ biomarkers, doctor-reviewed, tracked over time.
How much does sermorelin cost per month?
Sermorelin is the most common entry point, because it is FDA-approved, available through telehealth, and far cheaper than the synthetic HGH it quietly replaced. Expect $175 to $225 a month through a reputable telehealth clinic. IvyRx, for example, prices it at $175/month on a six-month plan, $195 on quarterly, and $225 on a true month-to-month subscription (IvyRx).
The aggressive telehealth entrants have pushed the floor lower. Eden and similar platforms now advertise entry tiers under $100 a month, while in-clinic brick-and-mortar pricing climbs to $300 to $400 (HealingMaps). Telehealth runs 20 to 40% cheaper than a physical clinic for one boring reason: overhead.
Here is the insider context the sub-$100 ads do not volunteer. At that price, something is usually thinner: a lower dose, a longer prepaid commitment, fewer included visits, or no labs. The headline rate and the all-in rate diverge fastest at the bottom of the market. Read what the number actually includes before you anchor on it.
And do not skip the labs to save money. Reputable sermorelin prescribers require a baseline IGF-1, growth hormone, and metabolic panel before starting, at $150 to $400, with follow-ups every three to six months at $100 to $300 (IvyRx). That is not the clinic padding the bill. IGF-1 is the marker that tells you whether the protocol is working at all.
How much is a CJC-1295 / ipamorelin stack?
This is the most widely used growth-hormone-secretagogue stack, and it prices higher than sermorelin alone because it is two compounds. Protocole runs the CJC-1295 and ipamorelin combination at about $325 for a five-week supply (PeptidesExplorer). At a brick-and-mortar clinic like Perfect B in Doral, a standalone three-month cycle starts at $445 (PerfectB).
Through a guided telehealth platform like Marek Health, the stack is dispensed through a licensed compounding pharmacy as part of a membership that costs $225 to $350 a month and includes a 65 to 100+ biomarker panel (PeptidesExplorer). Defy Medical structures it differently: a $250 initial consult, $150 follow-ups, and peptide medication of $200 to $500 a month depending on what is prescribed (VirtualCareFinder).
The thing only people who have actually run this stack know: it requires fasted, timed dosing, typically before bed on an empty stomach, because food blunts the growth-hormone pulse. That detail matters for cost because it is exactly the kind of protocol guidance a clinic builds into the price and a research vial leaves you to guess at from a Reddit thread. You are not just buying molecules. You are buying the instructions that make them do anything.
How much do BPC-157, NAD+, and tesamorelin cost?
These three get grouped together a lot, but they price very differently.
BPC-157. A research vial is $30 to $120 for 5 mg, plus $10 to $30 in supplies. A clinic program is $150 to $500 a month, and a full supervised six-month course totals $1,900 to $3,200 (PeakedLabs). This is the single most-bought therapy peptide, and as you will see below, its legal status is the one shifting fastest in 2026.
NAD+. At-home injection programs run $150 to $400 a month, with most ongoing programs landing $180 to $250 including pharmaceutical-grade compound and physician oversight (Hone Health). IV drips at a clinic cost far more per session, which is why the injection route has taken over for anyone doing it monthly rather than as a one-off.
Tesamorelin. This one has the widest spread of any peptide on the list. A research vial is $30 to $80; a compounded telehealth program is $150 to $300 a month at standard dosing; and premium concierge providers charge up to $1,500 a month for the same molecule (PerfectB). When the same compound ranges from $80 to $1,500, price is telling you almost nothing about the molecule and almost everything about the channel.
That tesamorelin spread is the whole lesson of this article compressed into one peptide. The compound is the cheap, commoditized part. What you pay for is the lane.
What does GLP-1 (semaglutide / tirzepatide) cost now that the shortage is over?
This lane changed hard in 2025, and the old cheap prices are mostly gone. During the shortage, compounding pharmacies could legally sell low-cost copies of semaglutide and tirzepatide. Then the FDA declared the shortages resolved: tirzepatide on 2 October 2024 and semaglutide on 21 February 2025. The enforcement deadlines to stop mass compounding followed, with the 503A tirzepatide deadline on 18 February 2025 and semaglutide on 22 April 2025 (FDA).
So in 2026 the lawful basis for compounded GLP-1 is no longer “the shortage,” it is personalization: a 503A pharmacy compounds a dose tailored to a documented clinical need under physician oversight. Pricing now looks like this:
- Compounded, personalized: roughly $99 to $169 a month for semaglutide and $125 to $299 a month for tirzepatide on annual prepay, all-inclusive (Trimi).
- Brand medication through telehealth: Ro charges a ~$145/month membership on top of brand drug that climbs from $299 to $449 by dose, landing the real bill at $445 to $595 a month (Trimi).
- Hims is winding its compounded GLP-1 program down entirely.
Myth worth busting: the $99 compounded semaglutide ads still circulating are not automatically a scam, but they are no longer running on the simple shortage logic that made them cheap. In 2026 that price has to be justified by genuine personalization, and a platform that cannot explain why your formulation is patient-specific is the one I would walk away from.
Here is the full price map, by peptide and by lane
I have collapsed every number above into one table so you can see the lanes side by side. The three lanes are: a supervised telehealth program (medication plus clinician plus follow-up), a grey-market research vial (molecule only), and, for context, the legacy HGH path that several of these peptides replaced.
| Peptide / therapy | Telehealth program (bundled) | Research vial (molecule only) | Notes |
|---|---|---|---|
| Sermorelin | $175 to $225 / mo | n/a (Rx peptide) | Baseline + follow-up labs extra; replaced $600 to $1,200+ synthetic HGH |
| CJC-1295 + ipamorelin | ~$325 / 5 weeks; $445 / 3-mo cycle at clinic | $40 to $120 / vial each | Requires fasted, timed dosing; clinic bundles the protocol |
| BPC-157 | $150 to $500 / mo | $30 to $120 / 5 mg vial | Most-bought therapy peptide; legal lane shifting in 2026 |
| NAD+ (injection) | $150 to $400 / mo | not the common DIY route | $180 to $250/mo typical; IV drips cost more per session |
| Tesamorelin | $150 to $300 / mo (up to $1,500 concierge) | $30 to $80 / vial | Widest channel spread of any peptide here |
| GLP-1 (semaglutide / tirzepatide) | $99 to $299 compounded; $445 to $595 brand | not a safe DIY peptide | Shortage over; compounding now requires personalization |
| Initial consult | $150 to $400 one-time | $0 | You are the clinician on the DIY path |
| Baseline labs | $150 to $400 one-time | $0 (and that is the problem) | IGF-1, hormones, metabolic panel |
Two things jump out of that table. First, the bundled monthly numbers cluster tightly around $150 to $400 for most single peptides, which means once you choose the legitimate lane, the peptide you pick matters less to your budget than people expect. Second, every “$0” in the research-vial column is a job you have just assigned to yourself: prescriber, pharmacist, QC lab, and the only person accountable if any of them gets it wrong.
Telehealth GLP-1 program with provider visits and pharmacy coordination.
Why is a research vial so much cheaper than a clinic?
Because the vial is only the molecule. Everything that turns a molecule into a therapy is unbundled and shifted onto you, and most of it is invisible until you need it.
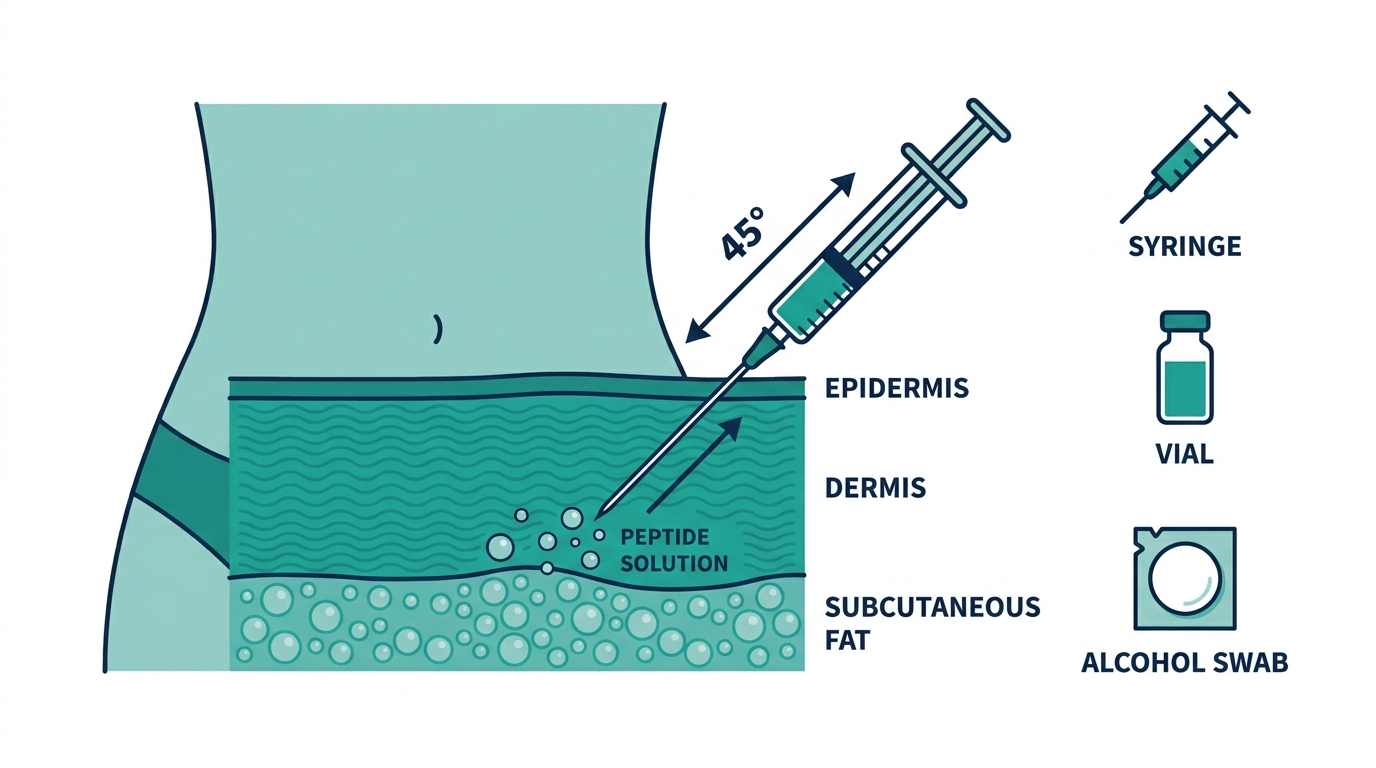
A research peptide does not arrive ready to inject. It arrives as a lyophilized (freeze-dried) powder you reconstitute yourself with bacteriostatic water you buy separately. You do the concentration math, you measure the dose on a U-100 insulin syringe, and you discard the vial after about 30 days. Get a decimal wrong in that math and you are not slightly off, you are off by a factor of ten.
So the price difference is not markup. It is the cost of five jobs the clinic does and the vendor does not: a clinician’s prescription, a named compounding pharmacy, baseline and follow-up labs, correct dosing, and accountability when something goes wrong. With a research vial you perform all five yourself for free, and “free” is doing a lot of quiet work in that sentence.
Personally, I think the cleanest way to see it is this: the clinic is not charging you $300 for $60 of peptide. It is charging you $60 for the peptide and $240 for the part that keeps you out of trouble. Whether that is worth it depends entirely on how much you value the four jobs you would otherwise be doing at 2 a.m. with a calculator.
Is peptide therapy covered by insurance?
No, and this is the one line clinics will tell you straight while vendors stay quiet. Compounded peptides used for longevity, recovery, or optimization are classified as elective or experimental, so you pay out of pocket regardless of how solid your clinical rationale is.
There is one narrow exception worth knowing. The FDA-approved peptides used for an approved indication can sometimes be covered: GLP-1s like semaglutide and tirzepatide for diagnosed obesity or type 2 diabetes, or tesamorelin for HIV-associated lipodystrophy. The moment you step outside the approved use into general optimization, coverage disappears.
Don’t believe a clinic that implies it can get your longevity peptides reimbursed. In 2026 that is essentially never true, and a provider hinting otherwise is either confused or selling. Budget for the full out-of-pocket cost before you start, not after the first invoice clears.
How will the 2026 regulatory changes affect cost?
This is the part that changes the math going forward, and it broke wide open this spring. On 22 April 2026 the FDA removed BPC-157 and a batch of other peptides from its 503A Category 2 list, the list that had effectively banned them from compounding (Loti Labs).
The full group pulled off Category 2 in April 2026 includes BPC-157, LL-37, DiHexa, DSIP (Emideltide), Epitalon, injectable GHK-Cu, KPV, PEG-MGF, Melanotan II, MOTs-C, Semax, and TB-500 (PeptideWise). Then the Pharmacy Compounding Advisory Committee meets on 23 to 24 July 2026 to evaluate whether seven of them, BPC-157, KPV, MOTs-C, Emideltide, Epitalon, Semax, and TB-500, should be formally added to the Section 503A bulks list that licensed pharmacies can legally compound (PeptideWise).
Read the cost implication carefully, because the headlines are getting it wrong. Removal from Category 2 is not FDA approval, and it does not yet let a pharmacy legally make BPC-157. The FDA still has to add it to the bulks list through formal rulemaking after the July review (Loti Labs). But the direction is clear: the door slammed in 2023 is being pried open through licensed pharmacies.
What that does to price: as the popular therapy peptides re-enter legal compounding, supervised access gets easier and more competitive, which over the next year should pull the legitimate-lane price down toward the grey-market lane while keeping the supervision. The smart read is that the safe lane and the cheap lane are converging, and they are converging in the safe lane’s direction. Buying a grey vial today to save money is paying a discount to skip the supervision that is about to become legally available anyway.
What would I actually budget?
Personally, if I were starting from zero, I would not anchor on the monthly subscription at all. I would budget the first six months as one number: roughly $2,000 to $3,200 all-in for a mid-range supervised program, baseline and follow-up labs included. That number feels higher than the $60 vial until you remember it is the only version of the cost that has someone other than you accountable for the dose.
If that figure is a stretch, the honest move is not to drop to the grey vial. It is to start narrower: one FDA-approved peptide like sermorelin through telehealth at $175 to $225 a month, with the labs, and add from there. The peptide you can actually afford to do correctly beats the stack you can only afford to do blind.
One line to take from this page: price the lane, not the molecule. The molecule is the cheap, commoditized part, as the $80-to-$1,500 tesamorelin range proves. Everything that makes peptide therapy safe, the prescription, the pharmacy, the dose, the labs, the accountability, is what the price actually buys. In 2026, with the regulatory door swinging back toward licensed compounding, that bundle is finally about to cost what it should.
Turn what you just learned into action.
Superpower lets you test 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
How much does peptide therapy cost per month in 2026?
Most single peptides run $150 to $400 a month through a legitimate telehealth clinic, with the medication, prescriber, and follow-up bundled. Sermorelin is $175 to $225, a CJC-1295/ipamorelin stack about $325 per five-week supply, NAD+ injections $150 to $400, and a general BPC-157 program $150 to $500. Budget another $150 to $400 once for baseline labs.
Why is the research vial so much cheaper, at $30 to $120?
Because it is only the molecule. The clinic price bundles a clinician’s prescription, a named compounding pharmacy, baseline and follow-up labs, correct dosing, and accountability if something goes wrong. With a research vial you do all five jobs yourself, including reconstituting a freeze-dried powder and calculating the dose, where a single decimal error changes the dose tenfold.
How much does sermorelin cost?
Roughly $175 to $225 a month through telehealth, with aggressive entry tiers advertised under $100 and brick-and-mortar clinics charging $300 to $400. It largely replaced synthetic HGH, which ran $600 to $1,200+ a month. Baseline and follow-up labs (IGF-1, GH, metabolic panel) are extra at $150 to $400.
Is peptide therapy covered by insurance?
Almost never for longevity or optimization use, which is classified as elective or experimental and paid out of pocket. The narrow exception is FDA-approved peptides for an approved diagnosis, such as a GLP-1 for obesity or type 2 diabetes, or tesamorelin for HIV-associated lipodystrophy. Step outside the approved use and coverage disappears.
How much do compounded GLP-1s cost now that the shortage is over?
Compounded, personalized semaglutide is roughly $99 to $169 a month and tirzepatide $125 to $299 on annual prepay. Brand medication through a platform like Ro lands at $445 to $595 a month with the membership. The shortage-era mass compounding ended in 2025, so 2026 pricing depends on genuine patient-specific personalization.
Will the 2026 FDA changes make peptides cheaper?
Probably, in the legitimate lane. The FDA removed BPC-157 and about a dozen peptides from 503A Category 2 on 22 April 2026, and a Pharmacy Compounding Advisory Committee meets 23 to 24 July 2026 to decide whether seven of them can be legally compounded. As popular peptides re-enter licensed compounding, supervised access should get more competitive and pull the safe-lane price down.
What is the cheapest safe way to start peptide therapy?
Start with one FDA-approved peptide, usually sermorelin, through a reputable telehealth clinic at $175 to $225 a month, with baseline labs included, rather than dropping to a grey-market vial. The peptide you can afford to do correctly under supervision beats the stack you can only afford to do blind.
Author: Vital Signs Today Editorial Team, [credential]”]. Educational content, not medical advice. Sources linked inline.
Primary sources (verify live before publish):
– FDA, “FDA clarifies policies for compounders as national GLP-1 supply begins to stabilize”: https://www.fda.gov/drugs/drug-alerts-and-statements/fda-clarifies-policies-compounders-national-glp-1-supply-begins-stabilize
– Loti Labs, “BPC-157 Legal Status 2026: FDA Category 2 Removal, PCAC Review”: https://lotilabs.com/resources/bpc-157-legal-status-2026-fda-update/
– PeptideWise, “FDA Peptide Reclassification 2026 503A List”: https://www.getpeptidewise.com/blog/fda-peptide-reclassification-2026/
– IvyRx, “Sermorelin Cost and Monthly Pricing Guide (2026 Update)”: https://www.ivyrx.com/blog/sermorelin-cost
– HealingMaps, “How Much Does Sermorelin Cost? The 2026 Pricing Guide”: https://healingmaps.com/sermorelin-cost-guide/
– PeakedLabs, “BPC-157 Cost (2026)”: https://peakedlabs.com/blog/bpc-157-cost-guide-2026
– Hone Health, “What Are NAD+ Injections? Benefits, Cost & Safety”: https://honehealth.com/edge/nad-injections/
– Perfect B, “Tesamorelin Cost: 2026 Pricing Guide”: https://www.perfectb.com/tesamorelin-cost/
– Perfect B, “CJC-1295/Ipamorelin Cost”: https://www.perfectb.com/cjc-1295-ipamorelin-cost/
– PeptidesExplorer, “Marek Health Reviews 2026” / “How Much Do Peptides Cost? 2026”: https://peptidesexplorer.com/blog/marek-health-reviews
– VirtualCareFinder, “Defy Medical Review (2026)”: https://virtualcarefinder.com/providers/defy-medical
– Trimi Health, “GLP-1 Cost Guide 2026” / “Cheapest Tirzepatide Providers 2026”: https://trytrimi.com/cost-guide
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


