
Your doctor ordered an ANA test, the result came back positive, and now you are convinced something is seriously wrong. Take a breath. Here is the thing almost nobody explains before they hand you this result. A positive ANA is one of the most common, most misread numbers in all of lab medicine, and on its own it usually means far less than people fear.
A positive ANA result is usually not the emergency it feels like. See it in context with your full panel. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
The ANA test is genuinely useful, but only when you understand what it can and cannot tell you. Get that backward and a harmless result can spiral into months of needless worry.
What is an ANA blood test?
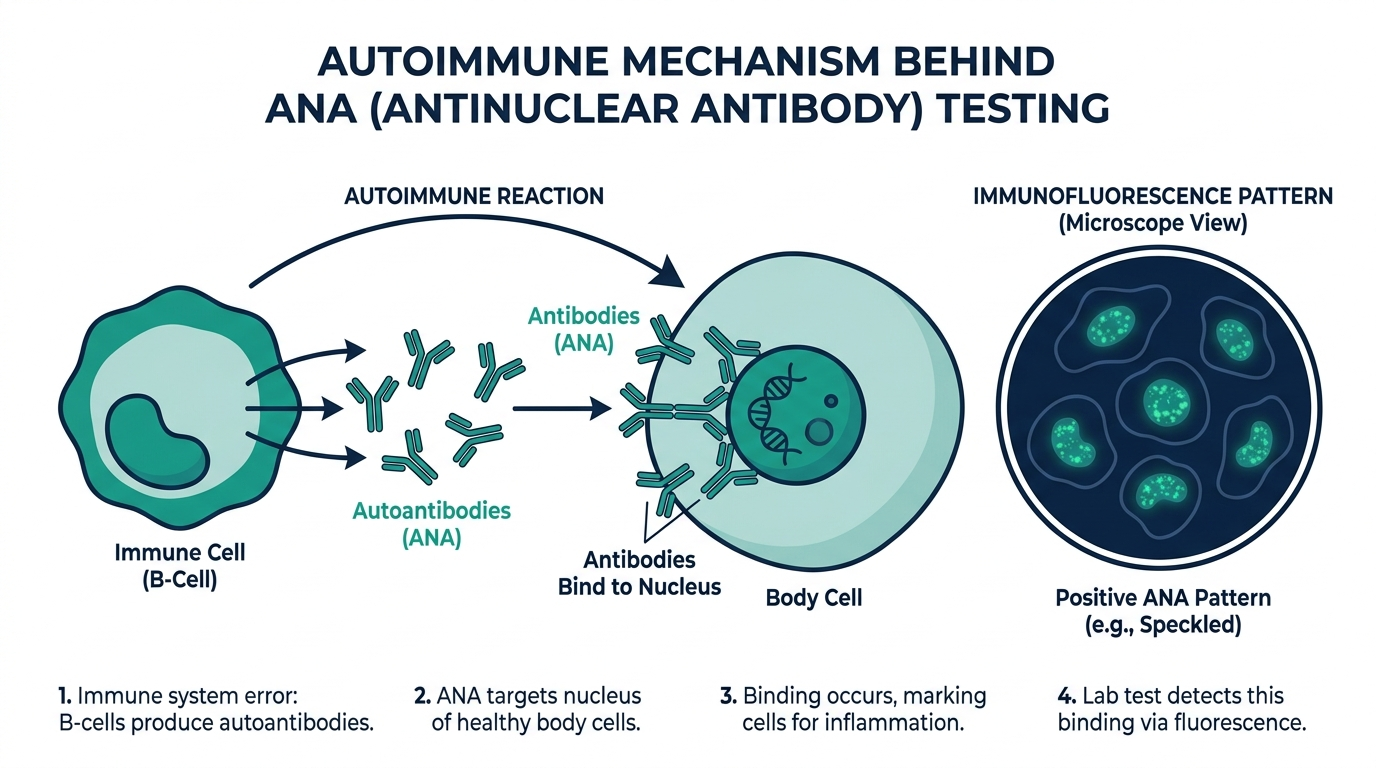
An ANA blood test is a blood test that looks for antinuclear antibodies, which are antibodies your immune system makes against the nuclei of your own cells (MedlinePlus). Normal antibodies hunt down foreign invaders like bacteria and viruses. Antinuclear antibodies turn that machinery inward and label your own healthy cells for attack, which is why a high level can be a clue to an autoimmune disease (Cleveland Clinic).
In plain terms, the ANA test is a screening tool. It asks one broad question: is your immune system showing signs of attacking your own tissues? It does not name a disease by itself. It simply raises a flag that, in the right clinical context, points your clinician toward conditions like lupus.

What does an ANA blood test show?
An ANA blood test shows whether you have antinuclear antibodies in your blood and, if so, how much and in what pattern. A full result has three parts: a positive or negative interpretation, a titer that reflects the concentration, and a fluorescent pattern seen under the microscope (MedlinePlus).
The most common way labs run the test is indirect immunofluorescence, where your blood sample is applied to cells and any antinuclear antibodies make the cell nuclei glow under a fluorescent microscope (Cleveland Clinic). What an ANA test shows, then, is a yes-or-no signal plus two pieces of texture, strength and shape, that help a specialist decide whether the signal is worth chasing. It is the starting point of an investigation, not the verdict.
What does a positive ANA blood test mean?
A positive ANA means antinuclear antibodies were detected in your blood, but it does not automatically mean you have an autoimmune disease (MedlinePlus). This is the single most important sentence in this whole article. A positive result is common, and most people who have one are perfectly healthy.
How common? Up to 3 in 10 people without any autoimmune disease still test positive for ANA (Cleveland Clinic). The American College of Rheumatology puts the figure another way: up to 15 percent of completely healthy people have a positive ANA, and only about 11 to 13 percent of people with a positive ANA actually turn out to have lupus or another autoimmune connective tissue disease (American College of Rheumatology).
Several things besides autoimmune disease can push an ANA positive, including viral infections, certain medications, and simply getting older (MedlinePlus). The level of antinuclear antibodies tends to rise with age, and a positive result is especially common in healthy women over 65 (MedlinePlus).
So a positive ANA is best read as an invitation to look closer, not a diagnosis. Your clinician will weigh it against your symptoms, a physical exam, your history, and follow-up blood tests before drawing any conclusion (American College of Rheumatology).
What does a negative ANA blood test mean?
A negative ANA means no antinuclear antibodies were detected, which makes an autoimmune disorder less likely (MedlinePlus). For a condition like systemic lupus erythematosus, that is reassuring. More than 95 percent of people with lupus test positive for ANA, so a negative result makes lupus very unlikely (American College of Rheumatology).
A negative ANA does not completely rule out every autoimmune disorder, however (Cleveland Clinic). Some autoimmune conditions are not driven by antinuclear antibodies, so a person can still be unwell with a clean ANA. The test is most powerful as a tool for ruling lupus out, and weaker as a way to rule everything else out.

What does the ANA titer mean?
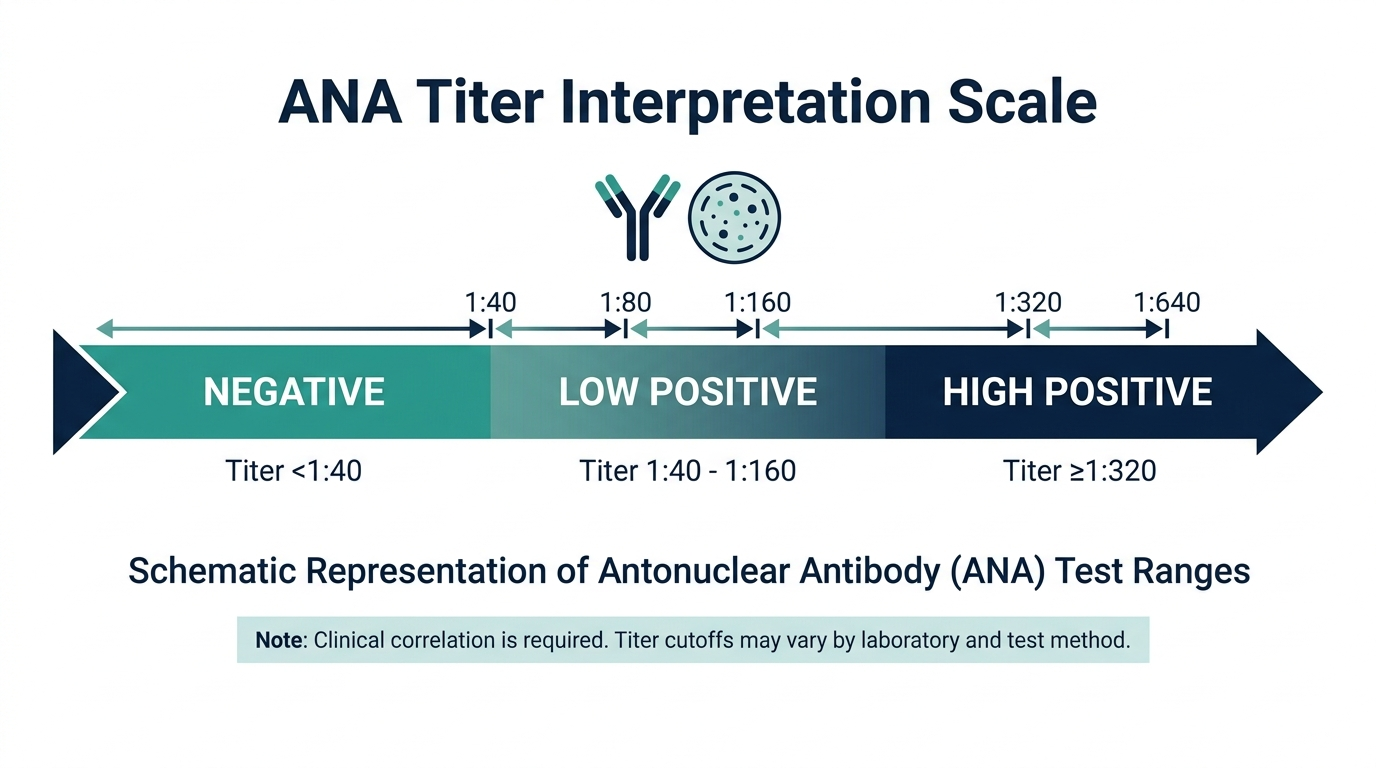
The titer tells you how concentrated your antinuclear antibodies are, and the higher it climbs, the more it tends to matter. Labs report it as a ratio such as 1:40, 1:80, 1:160, or 1:320. The number is how many times the lab could dilute your blood and still detect the antibodies, so 1:320 reflects far more antibody than 1:40.
This is where the nuance lives. Up to 30 percent of healthy people have a positive ANA at a titer of 1:40 or higher, which is exactly why low-titer positives are so often meaningless (UNC Rheumatology). Among patients with confirmed autoimmune disease, the median ANA titer was 1:320, a much stronger signal (UNC Rheumatology). The catch is that even high titers can show up in healthy adults, so titer raises or lowers suspicion without ever proving anything (UNC Rheumatology).
What does the ANA pattern mean?
The pattern describes how the antibodies light up the cell nucleus under the microscope, and it offers a hint about which specific antibodies might be present. Some samples make the whole surface of the nucleus glow, while others produce glowing speckles or dots (MedlinePlus).
A homogeneous pattern lights the nucleus evenly. A speckled pattern scatters bright dots across it. Other patterns include nucleolar and centromere. Each can steer a rheumatologist toward particular follow-up antibody tests, because different autoimmune diseases tend to favor different patterns. The pattern is a signpost for the next step, not a diagnosis on its own.
The part most people never hear: a positive ANA is usually a false alarm
Here is the insider reality that rarely reaches the patient. The ANA test was designed to be extremely sensitive, meaning it almost never misses lupus, and that sensitivity comes at a cost. It catches a huge number of healthy people too. When a test flags 15 to 30 percent of healthy people, a positive result in someone with no symptoms is more likely to be background noise than disease (American College of Rheumatology, UNC Rheumatology).
That is why rheumatologists have a quiet rule of thumb: a positive ANA without matching symptoms should not, by itself, send you down a long diagnostic rabbit hole (UNC Rheumatology). The test earns its keep when it is ordered for a reason, such as unexplained joint pain, rashes, fatigue, or other signs that fit an autoimmune picture. Ordered as a fishing expedition in a healthy person, it generates more anxiety than answers.
The practical takeaway: a positive ANA is a question, not a sentence. The right next move is a conversation with a clinician who can read it next to your actual symptoms, your titer, your pattern, and targeted follow-up tests, rather than a late-night search that convinces you of the worst.

The follow-up antibody tests after a positive ANA
When a positive ANA occurs in someone with real symptoms, the ANA itself is only the doorway. Rheumatologists then order more specific antibody tests that, unlike the broad ANA, tend to point at particular diseases. Knowing these names helps you understand a workup rather than fear it.
- Anti-double-stranded DNA (anti-dsDNA): closely tied to systemic lupus erythematosus and, in many patients, to lupus kidney involvement. It is far more specific for lupus than the ANA alone.
- Anti-Smith (anti-Sm): highly specific for lupus, though present in a minority of lupus patients, so a positive result carries weight while a negative one does not exclude lupus.
- Anti-Ro (SSA) and anti-La (SSB): associated with Sjogren’s syndrome and also seen in lupus. Anti-Ro matters in pregnancy because it can affect the baby, which is why it is checked carefully in some patients.
- Anti-centromere: linked with the limited form of scleroderma.
- Anti-Scl-70 (anti-topoisomerase): linked with diffuse scleroderma.
- Anti-U1-RNP: associated with mixed connective tissue disease.
The logic is a funnel. The ANA casts a wide net, and these specific antibodies narrow the field toward a particular diagnosis. This is exactly why a positive ANA in isolation settles nothing, and why the meaningful information often comes from the second round of testing chosen based on your symptoms.
How the ANA pattern steers the next test
The fluorescent pattern reported with an ANA is more than a curiosity. Because different antibodies produce different pictures under the microscope, the pattern gives a rheumatologist a head start on which specific tests to order.
- Homogeneous: an even glow across the nucleus, often associated with anti-dsDNA and anti-histone antibodies, which can raise consideration of lupus, including drug-induced lupus.
- Speckled: scattered bright dots, a common pattern seen with anti-Ro, anti-La, anti-Sm, and anti-RNP antibodies, and also frequently in healthy people.
- Nucleolar: glowing within the nucleoli, more often associated with scleroderma.
- Centromere: discrete dots corresponding to centromeres, associated with the limited form of scleroderma.
No pattern is a diagnosis on its own, and the speckled pattern in particular is so common in healthy people that it means little by itself. The value of the pattern is as a signpost that helps direct the specific antibody testing that follows, not as an answer.
Drug-induced ANA and lupus-like reactions
One cause of a positive ANA that patients rarely hear about is medication. Certain drugs can trigger the immune system to produce antinuclear antibodies, and in some people this leads to a lupus-like syndrome with joint pain and other symptoms. The important and reassuring feature is that drug-induced lupus typically improves after the responsible medication is stopped, unlike classic lupus.
This is one more reason a clinician reviews your full medication list when interpreting a positive ANA. Anti-histone antibodies are often associated with drug-induced lupus, which is why they may be checked when a medication is suspected. If you have recently started a new long-term medication and then developed joint aches with a positive ANA, that timing is worth mentioning, because the explanation may be straightforward and reversible.
Symptoms that justify ordering an ANA
Because the ANA flags so many healthy people, it works best when ordered for a reason rather than as a broad fishing expedition. It earns its value when symptoms already suggest an autoimmune connective tissue disease. Features that make the test meaningful include:
- Joint pain and swelling affecting multiple joints, especially with morning stiffness.
- A facial rash, particularly across the cheeks and nose, or rashes that worsen with sun exposure.
- Persistent unexplained fatigue combined with other autoimmune features.
- Dry eyes and dry mouth, which can suggest Sjogren’s syndrome.
- Fingers that turn white or blue in the cold (Raynaud’s phenomenon), skin tightening, or muscle weakness.
- Unexplained fevers or recurrent inflammation without an infectious cause.
When one or more of these are present, a positive ANA becomes a much more useful clue, because the pretest likelihood of disease is higher. In a person with none of these features, the same positive result is far more likely to be background noise. This is the core reason clinicians emphasize testing in context.
What the diagnostic workup actually looks like
Putting it together, here is the typical sequence after an ANA is ordered, which shows how rarely one number decides anything.
- Start with the clinical picture: the clinician evaluates your symptoms, examines you, and reviews your history and medications.
- Interpret the ANA in that context: the result is read alongside the titer and pattern, not as a yes-or-no verdict.
- Order specific antibodies when warranted: if symptoms and the ANA justify it, targeted tests such as anti-dsDNA or anti-Ro narrow the possibilities.
- Add supporting labs: tests like complement levels, inflammatory markers, blood counts, and urine studies help build or rule out a diagnosis.
- Refer to a rheumatologist: a specialist weighs the whole pattern, since autoimmune diagnoses rest on a combination of clinical and laboratory criteria rather than any single test.
The reassuring reality is that a diagnosis of lupus or a related disease is never made on a positive ANA alone. It requires a constellation of findings, which is precisely why a lone positive result in a well person is not the alarming news it can feel like at first.
Common misconceptions about the ANA test
A handful of myths cause the most needless worry after a positive ANA. Correcting them is some of the most valuable takeaway here.
- “Positive ANA means I have lupus.” Most people with a positive ANA do not have lupus or any autoimmune disease. The test is highly sensitive by design, so it flags many healthy people.
- “I should retest every few months to watch the number.” In healthy people without symptoms, repeatedly rechecking a positive ANA rarely helps and often adds anxiety. Unlike some antibodies, the ANA is not typically used to track disease activity over time.
- “A higher titer means my disease is worse.” A higher titer raises suspicion of disease but does not measure its severity, and even high titers occur in healthy adults. The titer is one input, not a severity score.
- “A negative ANA rules out all autoimmune disease.” A negative result makes lupus very unlikely, but some autoimmune conditions are not driven by antinuclear antibodies, so a clean ANA does not exclude everything.
The unifying correction is that the ANA is a screening signal read in context, never a standalone diagnosis or a dial that tracks how sick you are.
Should a positive ANA be repeated or monitored?
A frequent question after a positive result is whether it needs regular rechecking. For most people the answer is reassuring. If you have a positive ANA but no symptoms and a specialist has evaluated you, routinely repeating the test is generally not useful, because the number can persist for years without any disease ever developing. The ANA is best thought of as a one-time screening question rather than a marker to follow like blood pressure or blood sugar.
The situation differs if you develop new symptoms. If you were ANA-positive without disease and later notice joint pain, a photosensitive rash, dry eyes and mouth, or other autoimmune features, that is the moment to return to your clinician. At that point the earlier positive ANA, combined with the new symptoms, may justify the targeted follow-up antibody testing described above. In other words, what changes the plan is new clinical information, not the passage of time or the ANA number alone.
The bottom line on a positive ANA
A positive ANA is one of the most commonly misread results in medicine, and understanding it removes most of the fear it provokes. The test is deliberately sensitive, so it detects antinuclear antibodies in a large share of perfectly healthy people, and only a minority of positive results ever connect to lupus or another autoimmune disease. On its own, a positive ANA is a question, not a diagnosis.
What gives the result meaning is everything around it: your symptoms, the titer, the fluorescent pattern, your medications, and the specific follow-up antibodies a clinician may order. A positive ANA with matching symptoms is a useful clue worth pursuing. The same result in a well person with no signs of autoimmune disease is far more likely to be harmless background noise. The wisest response to a positive ANA is not a late-night search convinced of the worst, but a calm conversation with a clinician who can read the number in the full context of you.
Curious where your ANA really sits?
Baseline ANA and 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Is a positive ANA blood test something to worry about?
Usually not on its own. Up to 3 in 10 people without autoimmune disease test positive, and only about 11 to 13 percent of people with a positive ANA actually have lupus or another autoimmune condition (Cleveland Clinic, American College of Rheumatology). It is interpreted alongside your symptoms and follow-up tests, not in isolation.
What does an ANA test show in your blood?
It shows whether you have antinuclear antibodies, which are antibodies aimed at your own cell nuclei, along with a titer for how concentrated they are and a fluorescent pattern (MedlinePlus). It is a screening signal that helps point toward autoimmune diseases, not a diagnosis by itself.
What autoimmune diseases does an ANA blood test help detect?
It helps screen for systemic lupus erythematosus, Sjogren’s syndrome, scleroderma, mixed connective tissue disease, polymyositis and dermatomyositis, and autoimmune hepatitis, among others (Cleveland Clinic). It is most strongly tied to lupus, since over 95 percent of people with lupus test positive (American College of Rheumatology).
Can a healthy person have a positive ANA?
Yes, and it is common. Up to 15 percent of completely healthy people have a positive ANA, the rate rises with age, and it is especially frequent in women over 65 (American College of Rheumatology, MedlinePlus).
Does a higher ANA titer mean more serious disease?
A higher titer raises suspicion but does not prove disease. Up to 30 percent of healthy people are positive at 1:40 or higher, while the median titer in confirmed autoimmune disease is around 1:320, yet even high titers occur in healthy adults (UNC Rheumatology).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


