
Your hands ache in the morning. Your knuckles feel stiff and puffy. So your doctor orders blood work, and a few days later a result lands in your portal with names that mean nothing to you: rheumatoid factor, anti-CCP, ESR, CRP. You stare at the page wondering which one is the actual rheumatoid arthritis test, and what it is trying to tell you.
RF, anti-CCP, ESR, and CRP each tell part of the joint-pain story. Want to see them together with your full panel? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Here is the part most people get wrong from the start. There is no single test that switches a rheumatoid arthritis diagnosis on or off. There is a small panel of tests, each measuring a different thing, and the diagnosis comes from reading them together with your symptoms. Understanding what each one does turns that confusing result into something you can actually follow.
What is the rheumatoid arthritis blood test?
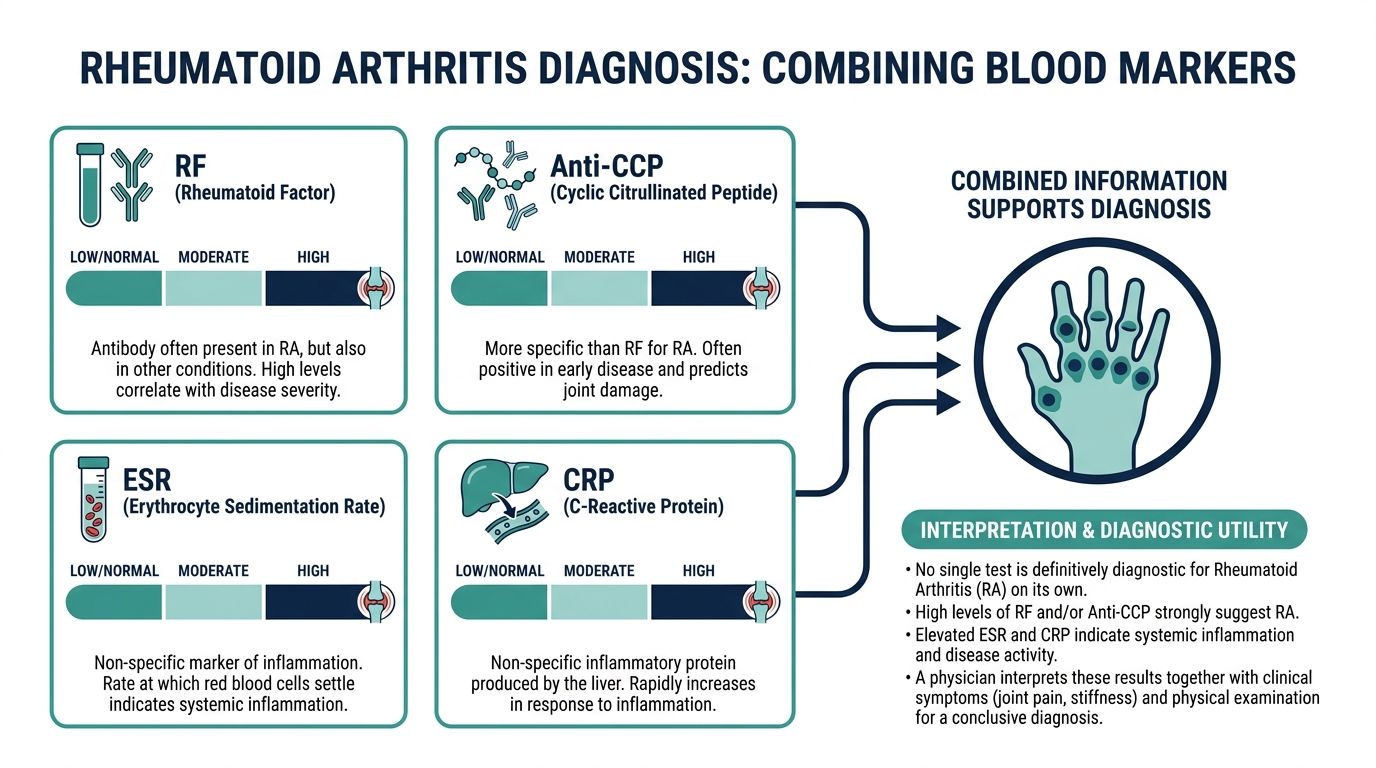
When people ask what is the rheumatoid arthritis blood test, the honest answer is that it is not one test but a set of blood tests used together to support a diagnosis. The two antibody tests that point most directly at rheumatoid arthritis are rheumatoid factor (RF) and anti-CCP (anti-cyclic citrullinated peptide). Alongside those, doctors usually run two inflammation markers, ESR and CRP, plus a complete blood count.
So if you are wondering what blood test is for rheumatoid arthritis, the short list is RF and anti-CCP for the autoimmune signal, and ESR and CRP for how much inflammation is active right now. No single number on its own is a diagnosis. The rheumatoid factor test is mostly used together with other tests rather than alone (MedlinePlus).

What blood test shows rheumatoid arthritis most specifically?
If you want the single most telling test, it is anti-CCP. It is the test that comes closest to a yes or no answer for rheumatoid arthritis, because CCP antibodies are found in most people who have the disease and are almost never found in people who do not (MedlinePlus).
The numbers explain why rheumatologists lean on it. Anti-CCP has a specificity of roughly 98 percent for rheumatoid arthritis, with a sensitivity of nearly 80 percent using modern second generation testing (PMC, clinical application of anti-CCP). Specificity that high means a positive anti-CCP rarely shows up by accident. So when someone asks what blood test for rheumatoid arthritis carries the most weight, anti-CCP is the answer, especially for confirming the diagnosis and catching it early.
What are the blood tests for rheumatoid arthritis, one by one?
There are four core blood tests plus a CBC, and each answers a different question. Here is the panel in plain terms.
- Rheumatoid factor (RF). An antibody that, instead of fighting germs, can attack your own healthy tissue. High levels can point to rheumatoid arthritis or another autoimmune disease (MedlinePlus). It is the oldest test of the group and the least specific.
- Anti-CCP antibodies. The most specific autoantibody test for rheumatoid arthritis, and the one that can turn positive early, sometimes before joint damage shows (MedlinePlus).
- ESR (erythrocyte sedimentation rate). A simple measure of how fast red cells settle in a tube, which rises when inflammation is present. It cannot confirm or rule out any condition on its own (Cleveland Clinic).
- CRP (C-reactive protein). Another inflammation marker that often moves faster than ESR. Like ESR, it measures how much inflammation is active, not what is causing it.
- Complete blood count (CBC). Checks for the anemia of chronic disease that often shadows long-standing rheumatoid arthritis.
RF and anti-CCP tell you about the autoimmune fingerprint. ESR and CRP tell you how loud the fire is burning. The CBC catches a common side effect of chronic inflammation. Read together, they sketch a far clearer picture than any one of them alone.
What is a normal rheumatoid factor level?
A normal, healthy amount of rheumatoid factor is less than 20 units per milliliter, written as under 20 U/mL (Cleveland Clinic). A result under that cutoff is reported as negative, which is the result you want. A result above it is reported as positive and is the point where your clinician starts looking harder.
One catch worth knowing. Many people have small amounts of rheumatoid factor in their blood and are perfectly healthy, and even a high level is not always a sign of disease (MedlinePlus). Always compare your number to the reference range printed on your own lab report, because exact cutoffs vary slightly by laboratory.

What does a positive result mean, and can a blood test show rheumatoid arthritis?
Can a blood test show rheumatoid arthritis? It can show the antibodies and inflammation strongly associated with it, but it cannot deliver the diagnosis by itself. The strongest signal is a positive rheumatoid factor combined with a positive anti-CCP, which together make rheumatoid arthritis very likely (MedlinePlus).
Here is how clinicians weigh the antibody results:
- RF positive and anti-CCP positive: the most convincing pattern, often called seropositive rheumatoid arthritis.
- Anti-CCP positive, RF negative: still meaningful, and can mean early rheumatoid arthritis or a higher chance of developing it later (MedlinePlus).
- RF positive, anti-CCP negative: RF can also be raised by other autoimmune diseases, chronic infections, and some cancers, so this is less specific and needs more context (MedlinePlus).
So when people ask what is the blood test for rheumatoid arthritis that confirms it, the truthful answer is that confirmation comes from the antibody pattern plus your symptoms and exam, not from a lone positive line on a page.
Does a blood test show rheumatoid arthritis in everyone who has it?
No, and this is the part that catches people off guard. Does a blood test show rheumatoid arthritis reliably in every patient? It does not. A meaningful number of people have genuine rheumatoid arthritis with negative RF and negative anti-CCP, a pattern called seronegative rheumatoid arthritis.
This is exactly why a negative result does not clear you. A negative rheumatoid factor does not rule out rheumatoid arthritis if you have symptoms (MedlinePlus). If your hands are swollen and stiff for an hour every morning but your antibodies come back clean, the workup is not over. Your doctor will weigh the clinical picture, the inflammation markers, and imaging before deciding.
Why are ESR and CRP run with the antibody tests?
ESR and CRP do not diagnose rheumatoid arthritis. They measure inflammation, which tells your doctor how active the disease is right now and, later, whether treatment is working. An ESR cannot confirm or rule out any condition on its own, but it is a fast way to learn whether inflammation is present (Cleveland Clinic).
This is also where the antibody tests and the inflammation markers part ways. RF and anti-CCP tend to stay positive even when the disease is well controlled, so they are not useful for tracking day to day activity. ESR and CRP rise and fall with the inflammation itself, which makes them the markers your rheumatologist watches over time to judge how you are responding.

The insider point: a positive anti-CCP can predate your first swollen joint
Here is the detail that rarely makes it into the patient-facing version. Anti-CCP antibodies can appear in the blood years before the first joint ever swells. A positive CCP result without a positive RF can mean you are in the early stages of rheumatoid arthritis or will develop it in the future (MedlinePlus).
That turns anti-CCP into something more than a confirmation test. It is a tripwire. Combined with its roughly 98 percent specificity, a positive anti-CCP in someone with vague early joint symptoms is a strong reason to get to a rheumatologist sooner rather than later (PMC, clinical application of anti-CCP). Early rheumatoid arthritis treatment protects joints before permanent damage sets in, so a positive anti-CCP caught early is one of the more actionable results on the whole panel. The flip side, and the cost of that high specificity, is that the test misses about one in five true cases, which is why a negative result never closes the door.
Reference ranges for the RA panel at a glance
Numbers only matter once you can place them against a range, and the RA panel mixes two very different kinds of test: antibody results that are essentially positive or negative, and inflammation markers that run on a scale. Here is how the common values line up. As always, the range printed on your own report is the one that governs, because labs and methods differ.
| Test | Typical reference | What it tells you |
|---|---|---|
| Rheumatoid factor (RF) | Negative, usually under 20 U/mL | An autoimmune signal, but low specificity |
| Anti-CCP | Negative below the lab cutoff | The most specific RA antibody, about 98 percent specific |
| ESR (men) | Roughly 0 to 15 to 22 mm/hr, rising with age | How much inflammation is active |
| ESR (women) | Roughly 0 to 20 to 29 mm/hr, rising with age | Same, with a higher ceiling than men |
| CRP | Often reported normal below about 3 mg/L | Inflammation, often moving faster than ESR |
Notice that ESR climbs with age and runs higher in women, which is normal physiology rather than a problem. A common rule of thumb sets the upper limit for men at roughly age divided by two, and for women at age plus ten divided by two. That is why an ESR that looks high for a young adult can be unremarkable for an older one, and why a raw number means little without the age and sex context beside it. CRP is a more direct chemical measure of inflammation and often rises and falls faster than ESR, which is why the two are frequently run together.
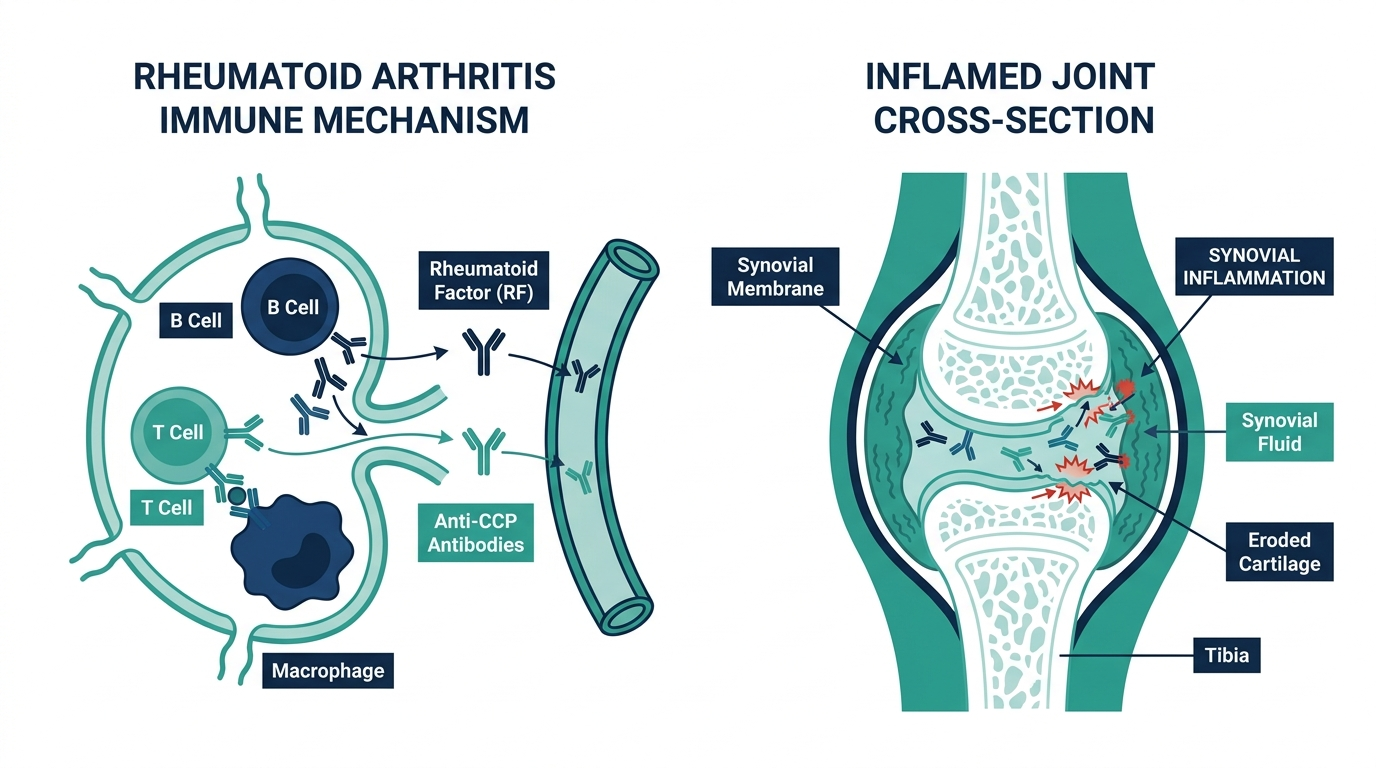
Symptoms that should prompt an RA workup
The blood tests only make sense in the context of the right symptoms, because rheumatoid arthritis is a clinical diagnosis that labs support rather than replace. The pattern of joint trouble is often more telling than any single ache.
- Symmetric joint involvement. Rheumatoid arthritis classically hits the same joints on both sides of the body, such as both wrists or the small joints of both hands, rather than one random knee.
- Prolonged morning stiffness. Stiffness that lasts well beyond an hour after waking is a hallmark, and it points more toward an inflammatory arthritis than the brief stiffness of ordinary wear-and-tear.
- Swelling and warmth in the small joints. Puffy, tender knuckles and finger joints, sometimes warm to the touch, reflect active inflammation in the joint lining.
- Fatigue and a general unwell feeling. Because rheumatoid arthritis is a systemic autoimmune disease, whole-body tiredness, low-grade fevers, and malaise often accompany the joint symptoms.
- Symptoms that persist for weeks. A few days of soreness after activity is not the same as several weeks of swelling and stiffness, and it is the persistence that raises the suspicion.
When several of these appear together and last, that is the moment the RF, anti-CCP, ESR, and CRP panel earns its keep. Catching rheumatoid arthritis early matters, because starting treatment before joints are permanently damaged is one of the strongest levers on long-term outcomes.

How to prepare, and what can skew the results
The RA panel is a routine blood draw, and for most people it needs no special preparation. Still, a few factors can nudge the inflammation markers in ways worth knowing.
- Fasting is generally not required for RF, anti-CCP, ESR, or CRP. If these are bundled with a metabolic or lipid panel, that other panel may call for fasting.
- Any active infection raises inflammation markers. A cold, a urinary tract infection, or any recent illness can push ESR and CRP up regardless of your joints, which can muddy the read. Mention any current infection to your clinician.
- Other conditions lift ESR. Anemia, pregnancy, older age, and even obesity can raise ESR independently, which is part of why it cannot confirm or rule out any single disease on its own.
- Some medications matter. Anti-inflammatory drugs and steroids can lower CRP and ESR, potentially masking active inflammation, so tell your clinician what you take.
The practical point is that a single high ESR or CRP is not proof of rheumatoid arthritis, and a normal one during treatment does not prove the disease is gone. These markers describe the current level of inflammation, and they are read in the context of everything else happening in your body that day.
Tests that help rule out the mimics
Several conditions can look like rheumatoid arthritis at first, so part of a good workup is testing to distinguish RA from its lookalikes. Your clinician may add tests beyond the core panel depending on the picture.
- ANA (antinuclear antibody). Often ordered when lupus or another connective tissue disease is on the table, since those can also cause joint pain and a positive RF.
- Uric acid. Helps separate gout, which is caused by uric acid crystals, from an inflammatory arthritis like RA. Gout tends to strike suddenly in a single joint, classically the big toe.
- Imaging. X-rays, ultrasound, or MRI can show joint erosion, inflammation of the joint lining, or fluid, which supports the diagnosis and gauges damage that blood cannot see.
- Joint fluid analysis. In some cases, drawing fluid from a swollen joint helps rule out infection or crystal arthritis such as gout.
This is the same logic that runs through the whole panel. No one test settles the question. The diagnosis is assembled from the antibody pattern, the inflammation markers, imaging, and the clinical exam, and part of that work is confidently excluding the conditions that impersonate rheumatoid arthritis.
Using the panel to track the disease over time
Once rheumatoid arthritis is diagnosed, the blood tests take on a second job: watching how the disease behaves and whether treatment is working. Here the antibody tests and the inflammation markers split duties.
- RF and anti-CCP are mostly diagnostic, not for tracking. They tend to stay positive even when the disease is well controlled, so repeating them frequently adds little. Your antibody status is largely a fixed part of your profile.
- ESR and CRP are the monitoring markers. Because they rise and fall with active inflammation, your rheumatologist watches them over time to judge flares and responses to medication. A falling CRP on a new treatment is an encouraging sign.
- The CBC catches side effects. Chronic inflammation can cause anemia, and some RA medications require blood monitoring of their own, so a complete blood count often rides along at follow-up visits.
Clinicians usually fold these labs into a broader measure of disease activity that also includes how many joints are tender and swollen and how you rate your own symptoms. The number on the inflammation marker is one input into that composite, not the whole verdict, which is why the goal is a stable overall picture rather than a single perfect lab value.
Common misunderstandings about the RA blood tests
A few myths cause real confusion, and clearing them up changes how you read your own results.
- “A positive rheumatoid factor means I have RA.” Not necessarily. Many healthy people carry some rheumatoid factor, and it also rises with other autoimmune diseases, chronic infections, and some cancers. RF is a clue, not a verdict.
- “A negative panel means I do not have RA.” Seronegative rheumatoid arthritis is real. Some people have genuine disease with negative RF and anti-CCP, so a clean panel does not close the case when symptoms persist.
- “A high ESR or CRP means rheumatoid arthritis.” These markers only say inflammation is present, not what is causing it. Infection, other autoimmune diseases, and many everyday conditions raise them too.
- “If my inflammation markers are normal, my RA is cured.” Well-controlled inflammation is the goal of treatment, not proof the underlying autoimmune tendency is gone. RA is managed over the long term, and monitoring continues even when you feel well.
The thread tying all of this together is the article’s core message. The rheumatoid arthritis blood test is not one test but a panel, and its power comes from reading the antibody pattern and the inflammation markers together, in the context of your symptoms, your exam, and sometimes imaging.
Turn what you just learned about rheumatoid arthritis into action.
Superpower lets you test rheumatoid arthritis and 100+ biomarkers from home, then re-check them over time so you can actually see progress, physician-reviewed at every step.
Frequently asked questions
What blood test is for rheumatoid arthritis?
There is no single test. The core panel is rheumatoid factor (RF) and anti-CCP antibodies, which point to the autoimmune disease, plus ESR and CRP, which measure inflammation, and usually a complete blood count. RF testing is mostly used together with these other tests (MedlinePlus).
What blood test shows rheumatoid arthritis most specifically?
Anti-CCP. CCP antibodies are found in most people with rheumatoid arthritis and almost never in people without it, giving the test a specificity of about 98 percent (PMC, clinical application of anti-CCP).
Can a blood test show rheumatoid arthritis on its own?
Not by itself. A positive RF together with a positive anti-CCP makes rheumatoid arthritis very likely, but diagnosis still depends on your symptoms and exam (MedlinePlus). Inflammation markers like ESR cannot confirm or rule out any condition alone (Cleveland Clinic).
What is a normal rheumatoid factor level?
A normal level is less than 20 units per milliliter, under 20 U/mL (Cleveland Clinic). Compare your result to the reference range on your own lab report, since cutoffs vary slightly by laboratory.
Does a blood test show rheumatoid arthritis if my results are negative?
Not always. Some people have seronegative rheumatoid arthritis, with negative RF and anti-CCP despite real disease. A negative result does not rule out rheumatoid arthritis when symptoms are present (MedlinePlus).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


