
You took a home test, saw a faint line, and your clinician said the next step is a blood draw to “check your hCG.” Or maybe hCG showed up on a lab order and you have no idea why anyone would measure it. Either way, you are about to learn that this single hormone is one of the most information-dense numbers in early pregnancy, and that the blood version of the test tells a very different story than the stick you peed on.
Tracking hCG week by week is stressful enough. See how your full hormone and health panel looks too. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Most explainers stop at “it confirms pregnancy.” The blood test does far more than that, and understanding what the number actually means changes how you read your own result.
What is hcg blood test?
An hCG blood test measures human chorionic gonadotropin, a hormone the placenta starts making soon after a fertilized egg implants in the uterus (Cleveland Clinic). A lab draws blood from a vein in your arm and either confirms whether the hormone is present or measures exactly how much is there. In plain terms: hCG is the chemical signal a pregnancy sends into your bloodstream, and this test reads that signal directly from the source rather than waiting for it to show up in your urine.
That distinction matters. Because a blood test can detect very small amounts of hCG, it can confirm a pregnancy earlier than a urine test, sometimes before a missed period (MedlinePlus). It is also the version clinicians reach for when they need a number, not just a yes or no.

What is hCG in a blood test, and what are the two types?
There are two distinct hCG blood tests, and confusing them is the single most common source of patient anxiety. A qualitative test answers one question: is hCG present, yes or no. A quantitative test, often labeled “beta hCG,” measures the exact concentration of hormone in milli-international units per milliliter (MedlinePlus).
- Qualitative hCG. Reported simply as positive or negative. Negative means no pregnancy detected, positive means pregnant. This is the blood version of a yes or no pregnancy test (MedlinePlus).
- Quantitative (beta) hCG. Reported as a specific number. This is the one that lets a clinician date a pregnancy, track whether it is progressing, and catch problems early (MedlinePlus).
When people obsess over their “hCG number,” they are talking about the quantitative test. The qualitative test has no number to obsess over, which is exactly its point.
What is a normal hCG level in a blood test?
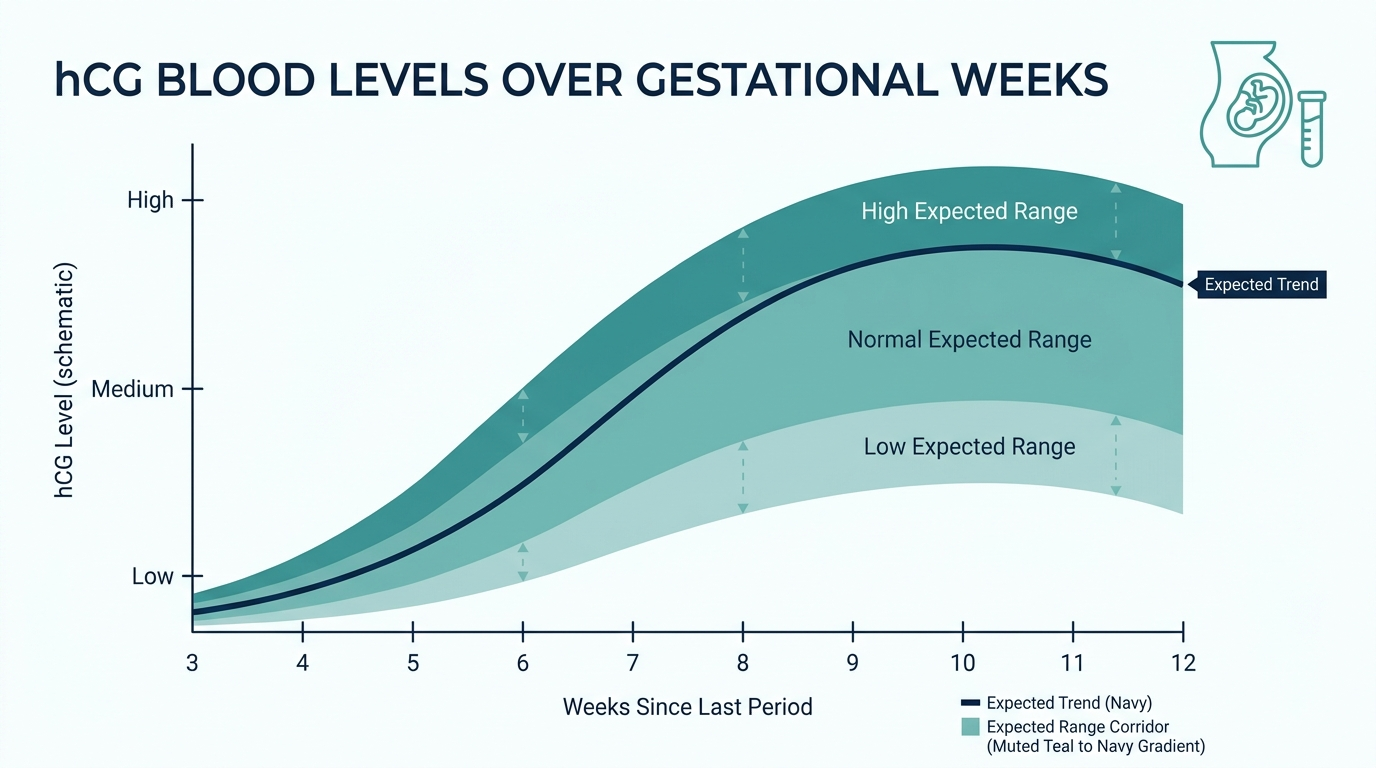
There is no single normal hCG level, because the number is supposed to climb steeply week by week in early pregnancy. An hCG level above 25 mIU/mL usually means you are pregnant (Cleveland Clinic). After that, the expected range widens dramatically as the weeks pass:
- Week 3: about 5 to 50 mIU/mL
- Week 4: about 5 to 426 mIU/mL
- Week 5: about 18 to 7,340 mIU/mL
- Week 6: about 1,080 to 56,500 mIU/mL
- Weeks 7 to 8: about 7,650 to 229,000 mIU/mL
- Weeks 9 to 12: about 25,700 to 288,000 mIU/mL
Those figures come from Cleveland Clinic, and the spread is enormous on purpose (Cleveland Clinic). At week 4, a perfectly healthy pregnancy might read 10 or it might read 400. This is why a single hCG value, on its own, tells you surprisingly little. The level peaks around week 10 or 11 and then declines for the rest of the pregnancy. If you are not pregnant, your hCG should be very low or undetectable.
How to read hCG blood test results?
The first rule of reading an hCG result is that the trend matters more than any single number. For a quantitative test, clinicians rarely act on one value. They draw it again 48 hours later and watch how it moves (StatPearls, NCBI).
Here is the framework most clinicians use:
- Qualitative result. Positive means hCG was detected. Negative means it was not. If the test is negative but pregnancy is still suspected, it is usually repeated about a week later, since hCG may simply be too low to detect yet (MedlinePlus).
- Single quantitative result. Compare it against the gestational week ranges above, remembering that the bands overlap heavily. One number alone almost never confirms how a pregnancy is doing.
- Two quantitative results, 48 hours apart. This is where the real information lives. In early pregnancy, hCG roughly doubles every 48 to 72 hours, and an approximate doubling at 48 hours is reassuring for a viable pregnancy (StatPearls, NCBI).
So the honest answer to “how do I read my hCG result” is: look at the direction and the speed, not just the size. A rising, doubling number is the signal clinicians want to see. A flat, falling, or slowly rising number is the one that prompts a closer look.

What does a high hCG level mean?
A high hCG level for your gestational age usually has a benign explanation, but a short list of conditions are worth ruling out. The most common reasons are simply being further along than you thought, or carrying twins or more, since multiple placentas produce more hormone (Cleveland Clinic).
The other causes are less common but important:
- Molar pregnancy. An abnormal growth of placental tissue can drive hCG far above the expected range (Cleveland Clinic).
- Certain cancers. In rare cases, a high hCG in someone who is not pregnant can be a sign of a germ cell tumor or other cancer (Cleveland Clinic). A positive qualitative result without a uterine pregnancy can point to testicular cancer, a trophoblastic tumor, or ovarian cancer (MedlinePlus).
This is why hCG is occasionally measured in people who clearly are not pregnant, including men. It is one of the few tumor markers that doubles as a pregnancy hormone.
What does a low hCG level mean?
A low hCG level, or one that is not rising as expected, points to a problem with the pregnancy and is the main reason clinicians order serial blood draws. The common causes include a miscalculated due date, an early miscarriage, a blighted ovum where a sac forms but no embryo develops, or an ectopic pregnancy (Cleveland Clinic).
Ectopic pregnancy is the one clinicians fear most, because it can be dangerous if missed. The tell is often not a single low number but a sluggish rise. In studies of women later diagnosed with an ectopic pregnancy, the hCG rose only slowly, with a doubling time stretched well beyond the normal two days (PubMed, doubling time and hCG score for ectopic pregnancy). A number that should have doubled but barely budged is a red flag worth acting on.
The part most people never hear: the discriminatory zone
This is the concept that quietly drives most early-pregnancy decision making, and almost no patient is told about it. Clinicians work with something called the discriminatory zone, a threshold hCG level above which a normal intrauterine pregnancy should be visible on ultrasound. With a transvaginal ultrasound, that threshold is around 1,500 mIU/mL (StatPearls, NCBI).
Here is why it matters so much. If your hCG is above roughly 1,500 but the ultrasound shows nothing in the uterus, that mismatch is a warning sign for an ectopic pregnancy. If your hCG is still below that zone, an empty-looking ultrasound may just mean it is too early to see anything, and the right move is usually to repeat the blood test in 48 hours rather than panic (StatPearls, NCBI).
So when your clinician seems oddly calm about an inconclusive early ultrasound, or oddly insistent on a repeat draw, this is the math running in the background. Your hCG number is not being read in isolation. It is being read against what the ultrasound can and cannot see at that level. That single idea explains most of the “let’s wait and recheck” advice that frustrates people in the first few weeks.

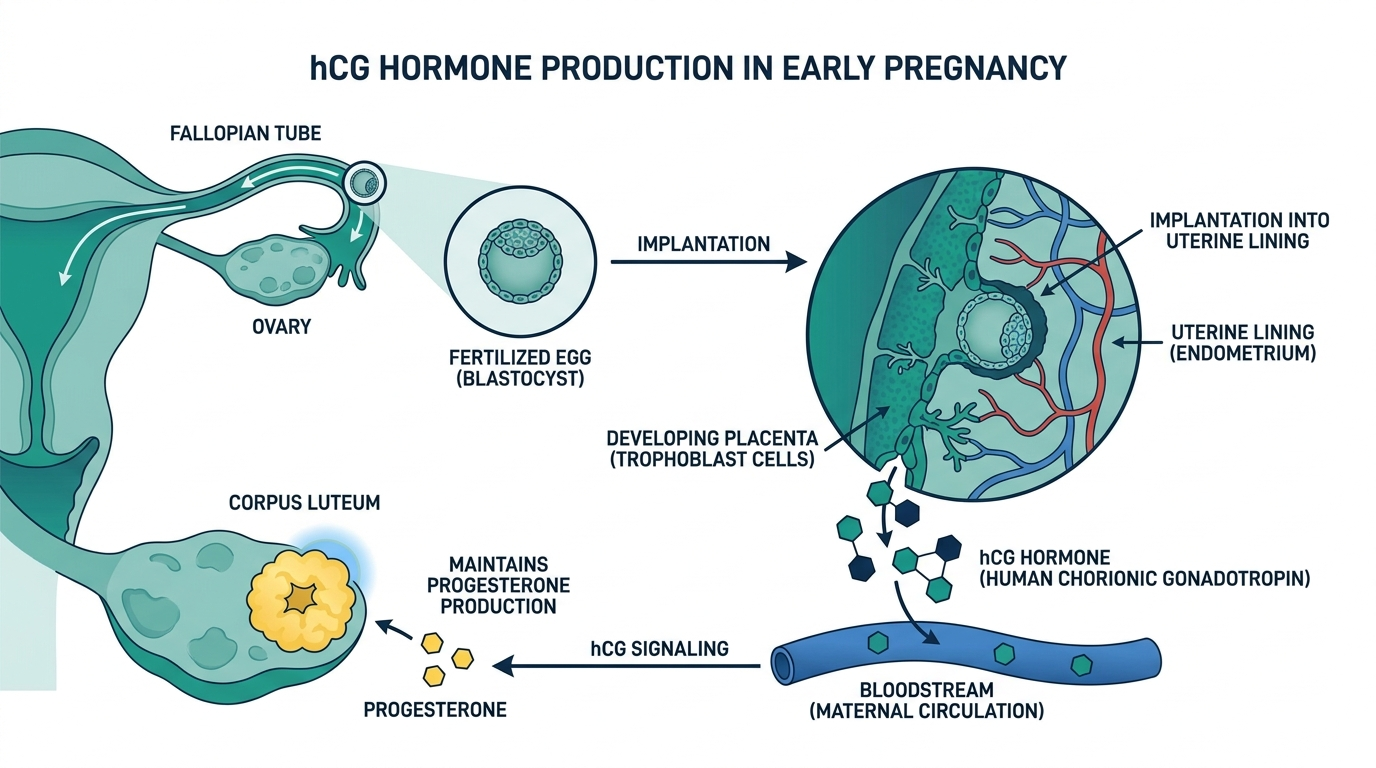
What hCG actually does in early pregnancy
Understanding why the hormone rises so steeply makes every number on your report more intuitive. hCG is not just a marker that happens to be convenient for testing. It has a real job, and that job explains its rise-then-fall curve.
After implantation, the early placenta produces hCG to send a message to the ovary: keep the corpus luteum alive. The corpus luteum is the structure left behind after ovulation, and hCG signals it to keep making progesterone, the hormone that maintains the uterine lining and sustains the pregnancy in its earliest weeks (Cleveland Clinic). Around the end of the first trimester, the placenta takes over progesterone production directly, the corpus luteum is no longer needed, and hCG is no longer required at such high levels. That handoff is exactly why hCG peaks around week 10 or 11 and then declines for the rest of the pregnancy. The curve is not random; it tracks a biological baton pass.
This also explains a familiar experience: morning sickness tends to be worst when hCG is highest in the first trimester and often eases as the level falls, which is one reason unusually high hCG, as in twins or a molar pregnancy, can come with more intense nausea.
When the number lies: false positives and false negatives
Because so many decisions ride on the hCG value, it helps to know the handful of situations where the test can mislead. These are uncommon, but clinicians actively watch for them, and knowing they exist can spare you unnecessary fear or false reassurance.
- The hook effect (falsely low or negative). When hCG is extraordinarily high, as in a molar pregnancy or advanced multiple gestation, the sheer amount of hormone can overwhelm the assay and paradoxically produce a low or even negative result. Labs overcome this by diluting the sample and retesting (PMC).
- High-dose biotin (falsely altered). Biotin, a common supplement found in hair and nail products, can interfere with many immunoassays and skew hCG results. This is why clinicians often ask you to pause biotin supplements before certain lab tests (PMC).
- Heterophile antibodies and phantom hCG (falsely positive). Some people have antibodies in their blood that trick the assay into reading positive when there is no pregnancy. The classic clue is a positive serum hCG with a negative urine test, since these interfering antibodies do not pass into urine. That mismatch is a key way labs unmask a phantom positive (PMC).
The practical lesson is that a result which does not fit the clinical picture, a sky-high hormone with a negative test, or a positive test with no evidence of pregnancy, is a reason to investigate the assay itself, not to accept the number blindly.
hCG in prenatal screening, not just pregnancy confirmation
Most people meet hCG as a pregnancy test, but the same hormone reappears later in pregnancy as one ingredient in prenatal screening. Here it is measured not to confirm pregnancy but to estimate the chance of certain conditions.
In first-trimester combined screening, a blood measurement of hCG (in its free beta form) is paired with another placental protein and an ultrasound measurement to estimate the risk of chromosomal conditions such as Down syndrome. In the second trimester, hCG is one of the analytes in the multiple-marker or quad screen. The important framing for patients is that these are screening tests, meaning they estimate probability, not diagnostic tests that give a yes or no. An abnormal screen leads to further, definitive testing rather than a diagnosis. So if you see hCG show up again weeks after your pregnancy was confirmed, it is likely playing this second role, and the number is being interpreted as part of a risk calculation rather than as a standalone result.

Tracking hCG down: miscarriage, molar pregnancy, and after treatment
hCG is not only watched on the way up. Following it back down to zero is a routine and important use of the quantitative test, and understanding why prevents a lot of confusion in a difficult time.
- After a miscarriage or pregnancy loss, clinicians often track hCG until it becomes undetectable, confirming that the pregnancy tissue has fully passed and no residual tissue remains. A stubbornly plateauing level can indicate retained tissue that needs attention.
- After a molar pregnancy, serial hCG monitoring is essential because a rising or persistently elevated level can signal persistent gestational trophoblastic disease that requires treatment. The hormone becomes the primary tool for detecting recurrence (Cleveland Clinic).
- As a tumor marker, in the rare cancers that produce hCG, such as certain germ cell tumors, the level is followed during and after treatment to gauge response, using the same quantitative assay that dates a pregnancy (MedlinePlus).
In all of these, the logic is identical to early pregnancy: the trend over serial draws, not any single value, carries the meaning.
Common misunderstandings about the hCG number
A few fixed beliefs cause a great deal of avoidable anxiety in the first weeks. Clearing them up is often more reassuring than any single result.
- A high starting number does not mean a healthier pregnancy. Because the week-by-week ranges overlap so widely, one person’s healthy pregnancy can read far higher or lower than another’s at the same gestational age (Cleveland Clinic). The rise matters, not the size.
- Doubling is a guideline, not a rigid law. hCG roughly doubles every 48 to 72 hours early on, but normal pregnancies show some variation, and the slope naturally slows as levels climb higher (StatPearls, NCBI).
- You cannot date a pregnancy precisely from one hCG value. The overlapping ranges make a single number a poor clock, which is why ultrasound is used for dating.
Blood versus home urine test: when each one wins
People often assume the blood test is simply the better version of the home stick, but each has a distinct role, and choosing the right one saves both money and worry.
- Home urine test. Cheap, private, and convenient, and highly accurate when used correctly on or after a missed period. Its limitation is that it is qualitative, a yes or no, and can read negative if taken too early when urine hCG is still low (MedlinePlus). Using first-morning urine, when it is most concentrated, improves early accuracy.
- Blood test. More sensitive, able to detect pregnancy slightly earlier, and, in its quantitative form, able to give an exact number that can be trended over 48 hours (StatPearls, NCBI). This is the test that matters when there is a specific concern, such as suspected ectopic pregnancy, monitoring after loss, or fertility treatment.
A reasonable rule of thumb: use a home test to answer “am I pregnant” once your period is due, and expect a blood test when a clinician needs a number to answer “how is this pregnancy progressing” or “why is something not adding up.”
What a healthy hCG rise looks like over 48 hours
The single most misunderstood idea about quantitative hCG is that a specific number tells you whether a pregnancy is healthy. It usually does not. In early pregnancy, the trend matters far more than any one value, which is why clinicians so often order a second draw about 48 hours after the first. The pattern of change is the real signal, and understanding it takes a lot of the fear out of waiting for that second result.
In a typical early intrauterine pregnancy, hCG rises briskly, and the classic teaching is that the level roughly doubles about every two to three days in the first weeks (StatPearls, NCBI). A rise that is clearly slower than expected, a plateau, or a fall can point toward a pregnancy that is not developing normally, including the possibility of an ectopic or an early loss. But there are important caveats. As levels climb higher, the doubling naturally slows, so a smaller percentage rise at a high starting number is not the same warning sign it would be at a low one. This is why the interpretation belongs with a clinician who sees your actual pair of numbers and the days between them, rather than a chart read in isolation.
The practical takeaway is to resist the urge to grade a single value against something you found online. If you have one number, you have a snapshot. If you have two numbers taken about two days apart, you finally have a trajectory, and the trajectory is what your care team is reading. Waiting for that second draw is genuinely more informative than agonizing over the first.
Questions patients often ask while waiting on hCG results
Few tests generate as much anxious searching as hCG, partly because the results carry so much personal weight and partly because the numbers behave in ways that feel counterintuitive. A handful of questions come up again and again, and short, honest answers tend to help more than reassurance alone.
Can I compare my number to my friend’s, or to my last pregnancy? Not usefully. The range of normal hCG at any given week is extremely wide, so two perfectly healthy pregnancies at the same stage can have values that differ several-fold. Your own trend over 48 hours is meaningful, but cross-comparisons rarely are. Does a very high number mean twins? It can raise the suspicion, since multiples often produce more hCG, but only an ultrasound confirms it, and plenty of singleton pregnancies run high as well.
Why does my clinic care about the number when I already had a positive home test? Because the home test answered whether hCG is present, while the blood number and its change over time help answer how the pregnancy is progressing and whether it is located where it should be. And finally, how long until things are clearer? Often the ultrasound becomes decisive once hCG passes the discriminatory zone discussed earlier, which is frequently a more reliable next step than repeating bloodwork indefinitely. Bringing these questions directly to your clinician, rather than to a search bar, is what turns a stressful wait into a plan.
Curious where your hcg really sits?
Baseline hcg and 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Does a normal blood test show hCG?
A standard panel like a complete blood count or basic metabolic panel does not measure hCG. It is a separate test that has to be specifically ordered, either as a qualitative pregnancy check or a quantitative beta hCG (MedlinePlus). So routine blood work will not reveal a pregnancy unless hCG was deliberately requested.
How do I get an hCG blood test?
You get one through a clinician, who orders it and sends you to a lab for a simple blood draw from a vein in your arm. No special preparation is needed (MedlinePlus). Many walk-in and online labs also offer it, but discussing the result with a clinician is what makes the number useful.
How early can an hCG blood test detect pregnancy?
A blood test can detect very small amounts of hCG and may confirm pregnancy before a missed period, earlier than most home urine tests (MedlinePlus). If an early test is negative but pregnancy is still suspected, it is usually repeated about a week later.
What is a normal hCG level if I am not pregnant?
If you are not pregnant, hCG is normally very low or undetectable, and a level above 25 mIU/mL generally indicates pregnancy (Cleveland Clinic). An elevated hCG in someone who is not pregnant can occasionally signal certain cancers and warrants follow-up.
What does it mean if my hCG is not doubling?
In early pregnancy, hCG normally roughly doubles every 48 to 72 hours, and an approximate doubling at 48 hours is reassuring (StatPearls, NCBI). A flat, falling, or slowly rising level can point to a miscarriage or an ectopic pregnancy and should be evaluated by a clinician promptly.
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


