
You have a blood draw coming up, maybe for a physical, a new job, a life insurance policy, or a court matter, and you used cannabis recently. The question keeps circling: would weed actually turn up in that vial of blood? It is one of the most anxiously googled drug-testing questions there is, and most of the answers online are either fearmongering or wishful thinking.
THC detection windows raise a lot of questions. Curious what else a blood panel could tell you about your health? One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Here is the short version before the detail. Yes, THC can show up in a blood test, but the window is far narrower than most people assume, and a routine blood panel from your doctor almost never looks for it in the first place. The nuance is what matters, so let us walk through it properly.
Would weed show up in a blood test?
Yes, weed can show up in a blood test, but only if the test is specifically designed to look for THC, and usually only within a short window after use. Standard blood work ordered by your physician, things like a complete blood count, cholesterol panel, or metabolic panel, does not screen for THC or any other drug. Those tests measure cells, electrolytes, lipids, and organ markers, not cannabis. So for the everyday question of whether weed shows up on blood tests at your annual checkup, the answer is essentially no, because nobody is testing for it.
When a blood test is built to detect cannabis, it measures delta-9-tetrahydrocannabinol (THC), the active compound, and sometimes its breakdown products. Blood testing for drugs is generally reserved for emergency departments and law enforcement, not primary care, because it is expensive, requires a trained phlebotomist to draw the sample, and only captures very recent use (PMC, objective testing for drugs). That same review notes blood testing typically reflects substance use within roughly 2 to 12 hours of the draw.

Does weed show up on a blood test, and for how long?
When a test is actually screening for it, weed does show up in a blood test, and the detection window depends almost entirely on whether you use occasionally or daily. THC enters your bloodstream within seconds of inhaling, peaks within minutes, then falls fast. In a controlled study, median whole-blood THC reached about 50 micrograms per liter just 15 minutes after starting to smoke, then dropped sharply, with most participants showing undetectable levels by 22 hours and only one still positive at that point (PMC, whole-blood cannabinoid pharmacokinetics).
So for an occasional user, the realistic blood detection window is short, often a matter of hours rather than days. Plasma THC commonly falls to 5 nanograms per milliliter or below within about 2 hours of smoking (PMC, human cannabinoid pharmacokinetics). This is exactly why a single weekend session is unlikely to register on a blood test taken days later, assuming you are not a heavy daily user.
Chronic daily users are a completely different story, and this is the part that surprises people. Because THC is fat-soluble, it accumulates in body fat and leaks back into the blood for days. In a monitored-abstinence study of 18 chronic smokers, THC was still detectable in 16 of them on day 7, at a median of 1.1 nanograms per milliliter, with several still above 2 nanograms per milliliter (PMC, plasma THC in chronic smokers). For a heavy user, then, weed can still show up in a blood test a full week after the last joint.
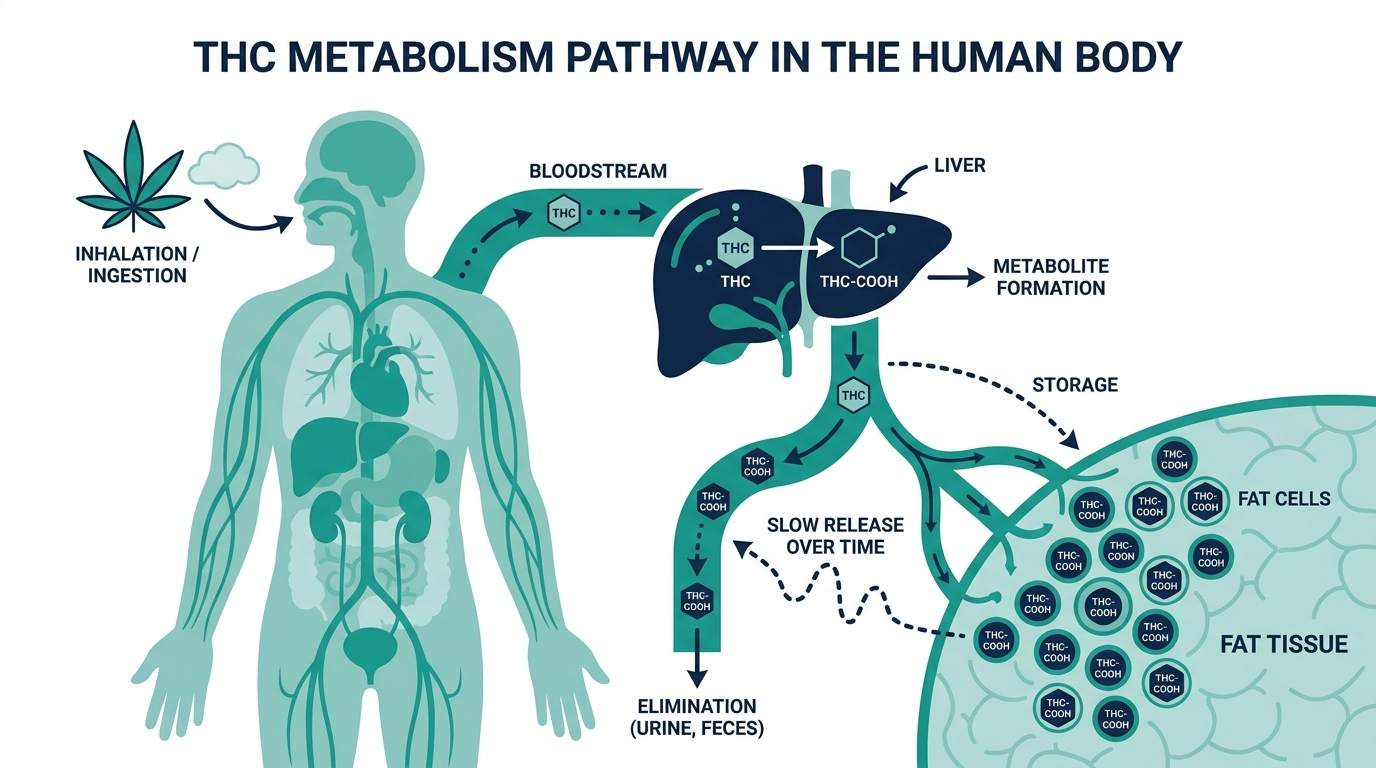
Why does weed leave the blood so fast but linger in the body?
Weed clears the blood quickly because THC is rapidly pulled out of circulation and into your tissues, especially fat. THC is highly lipophilic, meaning it loves fat, so right after it peaks in the blood it is taken up by well-perfused organs like the lung, heart, brain, and liver, then gradually redistributed into fatty tissue (PMC, human cannabinoid pharmacokinetics). That redistribution is what makes blood levels crash within hours even though the drug is still in your system.
The flip side is that fat acts as a slow-release reservoir. The same research found the fat-to-brain THC ratio climbed to roughly 21 to 1 after 7 days of exposure and 64 to 1 after 27 days, and described the terminal elimination half-life in chronic users as greater than 4 days (PMC, human cannabinoid pharmacokinetics). In plain terms: the rate-limiting step is not how fast your liver breaks THC down, it is how slowly your fat gives it back. That single fact explains nearly every confusing thing about cannabis testing, including why two people who smoked the same amount can test very differently.

Can weed show up in a blood test if you only used once?
For a true one-time or occasional user, weed can show up in a blood test only if the draw happens within a short window, usually the same day. The pharmacokinetic data is consistent here: after a single smoking session, whole-blood THC falls toward the limit of detection within hours, and most occasional users are negative by the next morning (PMC, whole-blood cannabinoid pharmacokinetics). The drug review puts the practical blood window at about 2 to 12 hours for recent use (PMC, objective testing for drugs).
This is the crucial distinction people miss when they panic about whether weed shows up in blood tests. Blood is the medium that best reflects recent, current impairment, which is precisely why DUI cases and emergency rooms use it. Urine, by contrast, detects inactive metabolites for far longer, up to about 30 days in heavy users by sensitive lab methods (PMC, objective testing for drugs). If you are worried about a test catching use from a week ago, urine is the medium to worry about, not blood, unless you are a daily user.
What does a positive THC blood test actually mean?
A positive THC blood test means measurable active THC was in your bloodstream at the moment of the draw, but it does not reliably prove when you used or whether you were impaired. This is the most misunderstood point in all of cannabis testing, and it has real legal weight.
Here is the insider reality that toxicologists know and the public rarely hears: in chronic users, a low positive blood level can persist for days into abstinence, so a number like 1 to 2 nanograms per milliliter does not necessarily indicate recent smoking or current intoxication (PMC, plasma THC in chronic smokers). The authors of that study explicitly warned that THC in plasma may not indicate recent use in chronic smokers. Meanwhile an occasional user can be functionally impaired with a level that already dropped below a legal cutoff because their blood THC fell so fast. The result is a genuine scientific mismatch: blood THC and actual impairment do not line up cleanly the way blood alcohol does. Anyone who tells you a single THC blood number proves exactly when you smoked is overselling what the chemistry can deliver.
Does weed show up in your routine blood work?
No, weed does not show up in routine blood work, and this is worth saying plainly because it causes needless anxiety. A complete blood count, lipid panel, liver function test, thyroid panel, or basic metabolic panel contains no THC assay. Drug screening has to be ordered deliberately and separately, and routine blood testing for drugs is rare even when clinically relevant, because of its cost and invasiveness (PMC, objective testing for drugs).
If your employer, insurer, or physician wants to test for cannabis, they will almost always reach for a urine or oral fluid test, not blood, because those are cheaper and have longer or more practical windows. Blood is the specialist tool, used when the question is recent use and impairment, such as after a crash. So the everyday fear that your cholesterol check secretly flags your weekend is unfounded. Nobody is looking unless they told you they are.
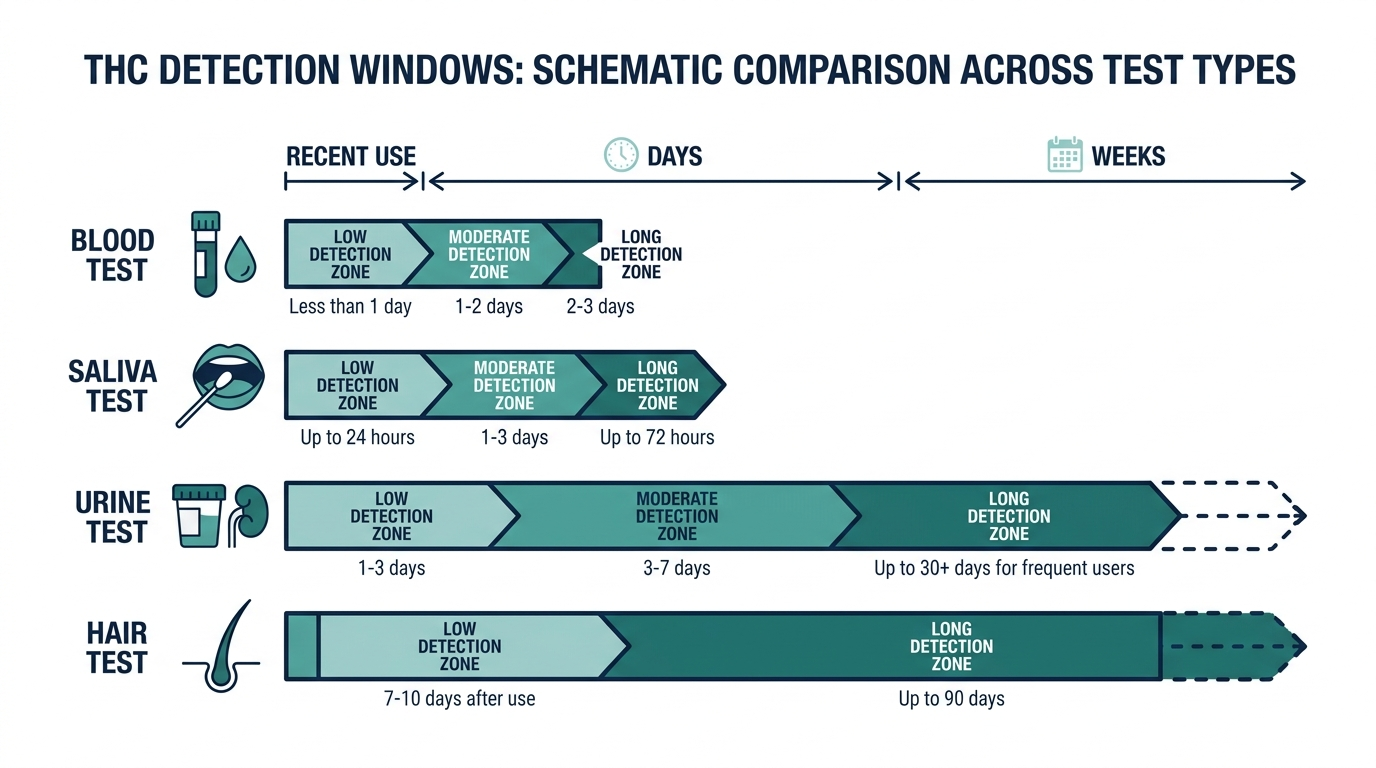
Blood versus urine, saliva, and hair: how the four tests compare
The single most useful thing you can do before worrying about a cannabis test is figure out which specimen is being collected, because the four common methods differ enormously in what they detect and for how long. Blood is actually the shortest-window test of the group for most people.
| Test type | What it detects | Typical detection window | Best at answering |
|---|---|---|---|
| Blood | Active THC (delta-9) | Hours for occasional users, up to about a week for chronic daily users (PMC) | Recent use and possible impairment |
| Saliva (oral fluid) | Active THC deposited in the mouth | Roughly a day, sometimes longer | Recent use, roadside screening |
| Urine | Inactive metabolite (THC-COOH) | Days to about 30 days in heavy users (PMC) | Past use, employment screening |
| Hair | Metabolites deposited in the hair shaft | Up to about 90 days | Long-term pattern of use |
The pattern is worth internalizing. Blood and saliva measure the active drug and answer “did you use recently,” while urine and hair measure inactive breakdown products and answer “have you used at all in the past weeks to months.” If you are anxious about a test catching last month’s use, that is a urine or hair concern, not a blood one.

Edibles behave differently from smoking
How you consume cannabis changes the timeline, and edibles are the biggest curveball. When you smoke or vape, THC hits the bloodstream within seconds and peaks within minutes, then falls fast (PMC). An edible takes a very different path.
- Slower onset, later peak. An edible has to be digested and absorbed through the gut, so blood THC rises over one to a few hours rather than in minutes. Someone who smokes and someone who eats the same dose will peak at very different times.
- A heavier metabolite footprint. Because an edible passes through the liver first, more of it is converted to metabolites before reaching the rest of the body. That larger pool of fat-stored metabolites is one reason edibles can extend the window seen on metabolite-based tests like urine.
- Less predictable. Absorption of an edible varies with what else is in your stomach and individual metabolism, making the timing harder to predict than inhaled cannabis.
The practical upshot: if you are estimating how long ago the active drug peaked in your blood, an edible pushes that peak later than smoking would, and it feeds the slow-release fat reservoir more heavily.
What lengthens or shortens your personal detection window
Two people who used the same amount can test very differently, and it is not random. Because the rate-limiting step is how slowly fat releases stored THC, anything that affects your body fat and metabolism affects your window (PMC).
- Frequency of use. This is the dominant factor. Occasional use clears in hours; chronic daily use builds a reservoir that leaks THC back into blood for days (PMC).
- Body composition. More body fat means more storage capacity for a lipophilic drug, which can prolong the slow release.
- Dose and potency. A larger amount of higher-potency cannabis loads more THC into the system to begin with.
- Individual metabolism. Genetic differences in the liver enzymes that process THC create real person-to-person variation.
Notice what is missing from this list: quick fixes. The window is governed by biology you cannot rush, which is exactly why the detox industry oversells what it can do.
Do detox drinks, water, or exercise actually help?
Because blood THC is driven by fat release rather than kidney clearance, the popular tricks aimed at flushing it out mostly miss the mechanism. It is worth being clear-eyed about this.
- Drinking lots of water does not pull THC out of your fat. It can dilute a urine sample, but for a blood test measuring active THC, hydration does not meaningfully change the level.
- Detox drinks and kits are marketed heavily but do not remove the fat-stored THC that a blood test can pick up in chronic users. There is no product that speeds the terminal elimination that takes days in heavy users (PMC).
- Exercise is a genuinely double-edged case. Burning fat can, at least in theory, release stored THC back into the blood, which means intense exercise shortly before a test could transiently raise, not lower, your blood level rather than clear it.
The only reliable variable is time. For occasional users that time is short, often hours. For chronic users the terminal half-life exceeds four days, so meaningful clearance simply takes days of abstinence (PMC).
Can CBD or secondhand smoke cause a positive blood test?
Two common worries deserve a straight answer, because both come up constantly and both have nuance.
CBD products. Pure CBD is a different compound from THC and is not what a THC test targets. The catch is that many over-the-counter CBD products, especially full-spectrum ones, legally contain trace THC, and mislabeling is common in an underregulated market. Heavy use of a THC-containing CBD product can in principle contribute THC to your system, so “it was just CBD” is not an automatic explanation for a positive.
Secondhand smoke. Realistically, incidental exposure to someone else’s cannabis smoke is very unlikely to produce a meaningful active-THC blood level. The concentrations involved in ordinary passive exposure are far below what heavy direct use produces, and blood clears active THC quickly. Extreme, prolonged exposure in an unventilated space is the only scenario where trace effects have been discussed, and it does not apply to a normal social setting.
The legal picture: why THC blood limits are contested
The mismatch between blood THC and impairment described earlier is not just academic. It sits at the center of how cannabis-impaired driving is prosecuted, and it is why the legal landscape is genuinely unsettled.
- Per se limits. Some jurisdictions set a specific blood THC threshold, such as a fixed nanograms-per-milliliter number, above which a driver is legally impaired regardless of actual behavior. These vary by state, and some use a zero-tolerance rule instead.
- The scientific objection. Because a chronic user can sit above such a cutoff days into abstinence while an occasional user can be impaired below it, toxicologists caution that a single blood number is a poor standalone proxy for impairment, unlike blood alcohol (PMC).
- What this means for you. If a blood THC result carries legal weight in your situation, the number alone rarely tells the full story, and the timing of the draw relative to use matters enormously.
None of this is legal advice, and rules differ sharply by location. The point is that the underlying chemistry, active THC crashing fast while impairment and metabolites follow their own timelines, is exactly why these laws remain debated.
What to do if you are facing a THC blood test
If you know a THC-specific blood draw is coming, the honest and useful advice is narrow, because most of what circulates online does not match the chemistry. Here is what actually applies.
- Confirm the specimen first. Ask, or read the paperwork, to learn whether they are collecting blood, urine, saliva, or hair. It changes everything about the window, and people often assume blood when the collector is actually taking urine.
- Understand you cannot rush biology. For occasional users the active THC in blood clears in hours, and for chronic users the terminal elimination takes days because fat releases stored THC slowly (PMC, human cannabinoid pharmacokinetics). Time abstinent is the only lever that reliably moves the number.
- Skip the intense workout right before. Because burning fat can release stored THC back into circulation, a hard gym session shortly before a draw may nudge blood levels up rather than down.
- Disclose what is relevant. If you use cannabis medically, or take a full-spectrum CBD product that can contain trace THC, note it so a result is read in context rather than as a surprise.
The larger point is calm rather than panic. A routine physician draw is not screening for cannabis at all, and even a dedicated THC blood test reflects a short, recent window for most people. Knowing which specimen you face, and knowing that only time meaningfully changes an active-THC level, replaces a lot of anxious guessing with a clear picture of what the test can and cannot see.
Curious what your own levels look like?
Baseline 100+ biomarkers today and retest as life changes, all in one membership with physician review.
Frequently asked questions
Does weed show up in a blood test at a normal doctor visit?
No. Standard blood work such as a complete blood count or metabolic panel does not test for THC. Drug screening must be ordered separately, and even then blood is rarely used because it is costly and only catches very recent use (PMC, objective testing for drugs).
How long does weed stay in your blood?
For occasional users, THC usually falls below detection within hours, often the same day, with the practical window around 2 to 12 hours (PMC, objective testing for drugs). In chronic daily users it can linger about a week, with THC still detectable in most people on day 7 (PMC, plasma THC in chronic smokers).
Can weed show up in your blood test if you only smoked once?
Only if the draw is within a short window of use, generally the same day. After a single session, whole-blood THC drops toward undetectable within hours and most occasional users are negative by the next morning (PMC, whole-blood cannabinoid pharmacokinetics).
Why does a urine test catch weed for longer than a blood test?
Blood tests measure active THC, which clears circulation fast as it moves into fat. Urine detects inactive metabolites that persist much longer, up to about 30 days in heavy users by sensitive methods (PMC, objective testing for drugs).
Does a positive THC blood test prove I was high?
Not reliably. Blood THC and impairment do not align the way blood alcohol does. In chronic users a low positive can persist into abstinence without recent use, so a single number cannot pin down timing or intoxication (PMC, plasma THC in chronic smokers).
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


