
Your doctor ordered a routine STI panel, or you are pregnant and getting standard prenatal labs, and now there are three letters on the order or the result page that nobody explained: RPR. It sounds technical and faintly alarming, especially once you find out it has something to do with syphilis. Take a breath. RPR is one of the oldest, cheapest, and most useful screening tests in medicine, and once you understand what it actually does, a reactive result becomes a lot less frightening.
An RPR result confuses almost everyone at first read. See your full panel alongside it for a clearer picture. One at-home Superpower draw checks 100+ biomarkers, physician-reviewed.
Here is the part most people miss. RPR does not look for the syphilis bacterium at all. It looks for something your body makes when certain things go wrong, and that single fact explains almost everything strange about how the test behaves.
What is an RPR blood test?
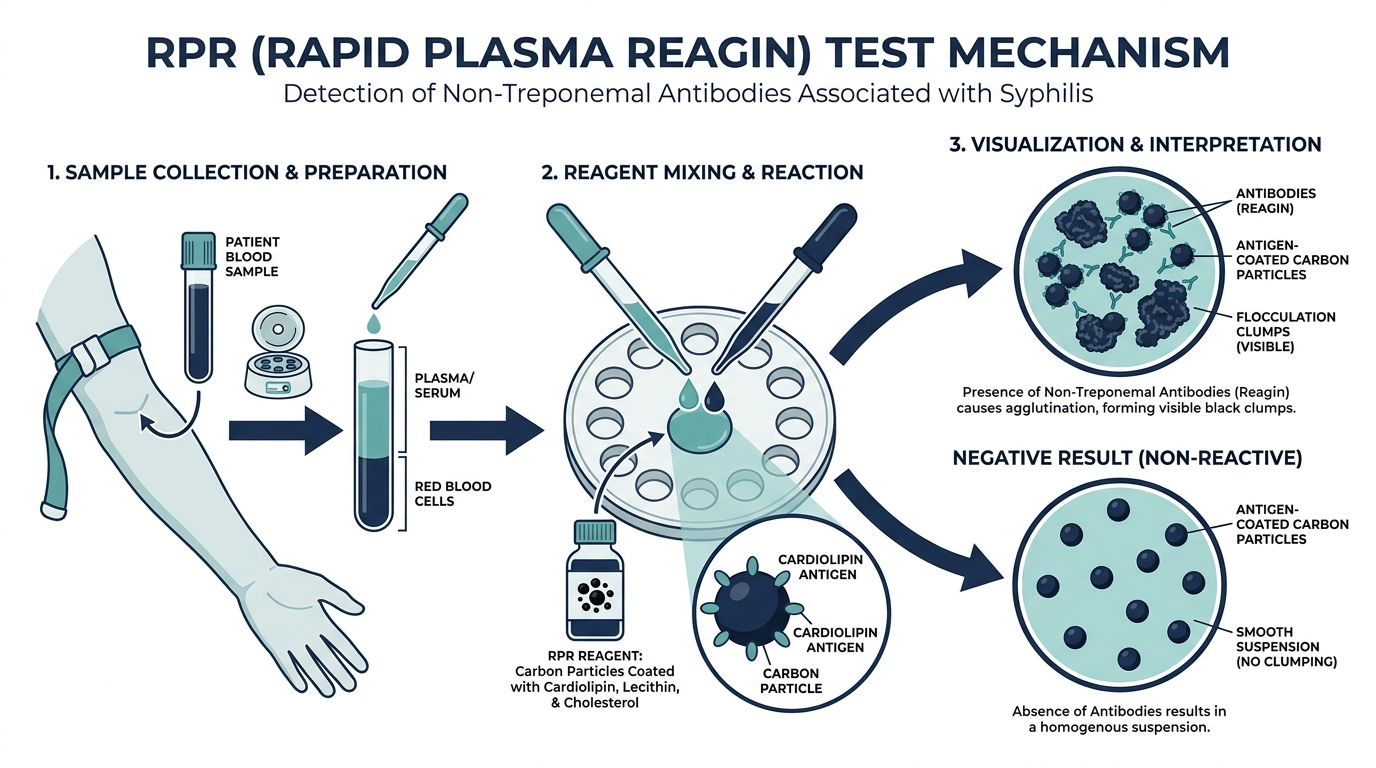
An RPR blood test, short for rapid plasma reagin, is a screening blood test for syphilis. It detects antibodies your body produces in response to the damage caused by a syphilis infection, rather than detecting the bacterium Treponema pallidum directly (MedlinePlus). When people ask what is RPR in a blood test, the honest one line answer is this: it is an inexpensive antibody screen that flags the possibility of syphilis so a more specific test can confirm it.
RPR belongs to a family called nontreponemal tests, which the CDC has long recommended as first line screening for syphilis (StatPearls, NCBI). The other classic member of that family is the VDRL test. They work on the same principle and are often used interchangeably depending on the lab.

What does RPR mean in a blood test, and what does it actually measure?
RPR measures reagin, a type of antibody that appears in the blood when cells are damaged, which happens during a syphilis infection. The test does not see the spiral shaped bacterium itself. Instead it reacts to antibodies aimed at substances released from injured cells (StatPearls, NCBI).
This indirect design is the test’s great strength and its great weakness at the same time. The strength is that it is fast, cheap, and easy to scale across millions of pregnancies and clinic visits. The weakness is specificity. Because reagin antibodies can show up in other conditions that also damage cells, RPR can flag positive when syphilis is not the cause. That is why a reactive RPR is a starting point, never a final answer.
What is a normal RPR blood test result?
A normal RPR result is nonreactive, which is also called negative. A nonreactive result means no reagin antibodies were detected and is considered the normal finding (MedlinePlus). For most healthy people with no syphilis exposure, this is exactly what comes back.
One important caveat lives inside that reassuring word. A nonreactive RPR is not an ironclad all clear. The test can miss very early infection before antibodies have built up, and it can also miss very late stage syphilis, because the body does not always keep producing reagin at detectable levels (MedlinePlus). Positive serology usually appears only about 3 to 6 weeks after exposure (StatPearls, NCBI). So if you were exposed last week and test today, a negative result may simply be too early to count.
What does a reactive (positive) RPR result mean?
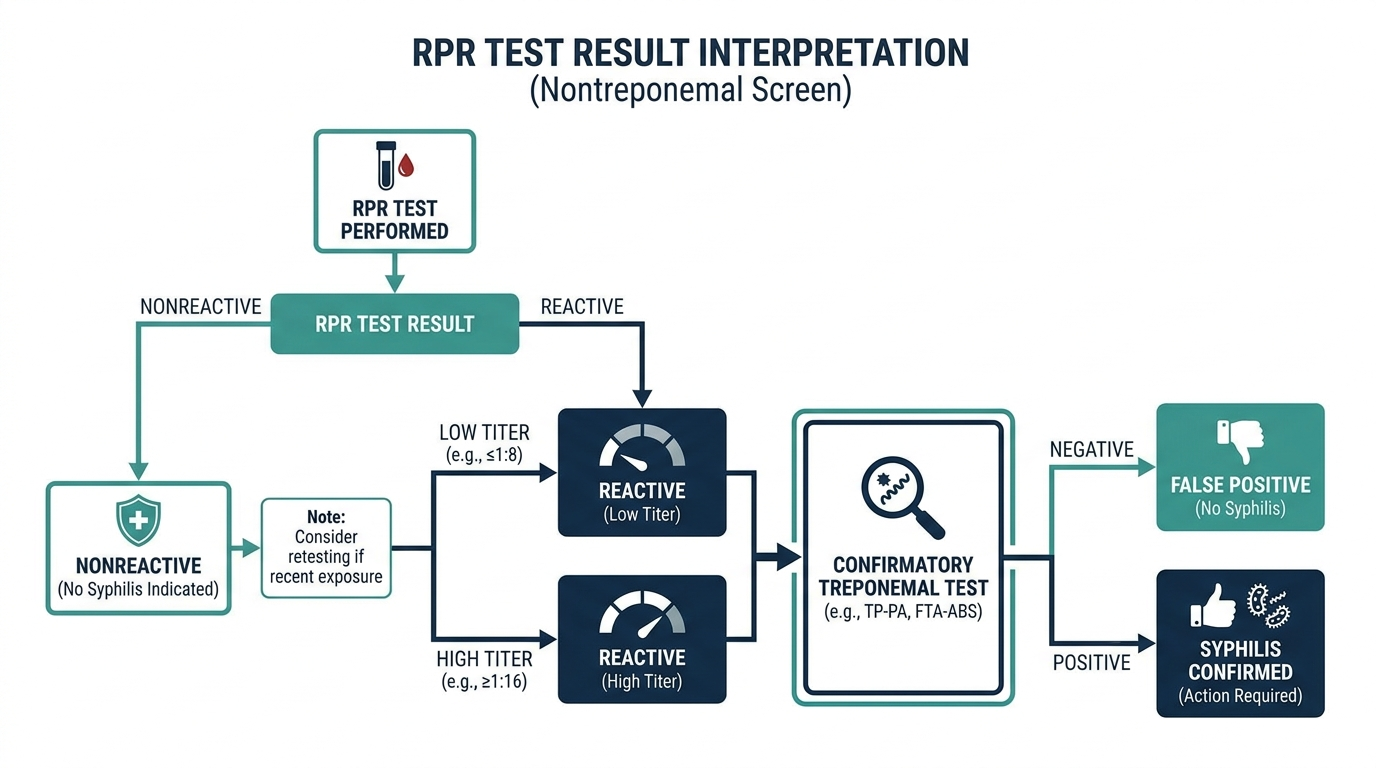
A reactive RPR result means reagin antibodies were found, which raises the possibility of syphilis but does not by itself prove it. A reactive result must be confirmed with a more specific treponemal test, such as the FTA-ABS test, before syphilis is diagnosed (MedlinePlus). Diagnosis requires both a reactive nontreponemal test like RPR and a reactive treponemal test (PMC, RPR and the serologic diagnosis of syphilis).
Sensitivity, meaning how reliably the test catches true infection, depends heavily on the stage of disease. RPR shows about 86 percent sensitivity in primary syphilis, 100 percent in secondary syphilis, and drops to roughly 73 percent in latent syphilis (StatPearls, NCBI). In plain terms, the test is at its sharpest in the secondary stage and weaker at the very beginning and the very end of the disease.
A reactive RPR also comes with a titer, and understanding the titer is where this test gets genuinely interesting.

What is an RPR titer, and why does it matter so much?
An RPR titer is the highest dilution of your blood that still produces a reactive result, written as a ratio like 1:8 or 1:32. It is a rough measure of how much reagin antibody is present, and a higher number generally means more antibody and a more active process. The titer is what makes RPR a quantitative test rather than a simple yes or no (StatPearls, NCBI).
Two titer facts are worth carrying with you:
- Low titers tend to be less alarming. False positive results frequently sit at a titer of 1:8 or lower, and the test can stay reactive at a low titer long after successful treatment, a situation clinicians call the serofast state (StatPearls, NCBI).
- High titers raise the stakes. An RPR titer of at least 1:32 is associated with an increased risk of neurosyphilis, the form that involves the nervous system (StatPearls, NCBI).
This is also why one RPR number in isolation can mislead you. A single titer is a snapshot. The real signal is the trend over time, which is the next thing most patients are never told.
Why is RPR used to track syphilis treatment?
RPR is the standard way to monitor whether syphilis treatment worked, because the antibody level it measures should fall after successful antibiotic therapy. After treatment, RPR reactivity typically declines, and the test can also detect reinfection if the level climbs back up (StatPearls, NCBI).
The benchmark clinicians watch is a fourfold change in titer, which equals two dilution steps, for example a drop from 1:32 to 1:8 after treatment. A confirmed fourfold or greater rise in RPR signals reinfection or treatment failure and triggers a fuller workup, including repeat HIV testing, examination of cerebrospinal fluid for neurosyphilis, and additional treatment based on the stage of disease (PMC, RPR and the serologic diagnosis of syphilis). This is the reason a treponemal test alone cannot replace RPR. Treponemal antibodies usually stay positive for life, so they cannot tell you whether the infection is active or whether treatment is working. RPR can.
The part most people never hear: why a positive RPR is often not syphilis at all
Here is the insider truth that takes the fear out of a reactive result. In the United States, false positive nontreponemal results occur in roughly 1 to 2 percent of people tested (StatPearls, NCBI). Because RPR detects reagin rather than the syphilis organism, anything that injures cells in a similar way can light it up.
The usual suspects behind a false positive RPR include HIV, hepatitis, Lyme disease, malaria, certain types of pneumonia, intravenous drug use, and autoimmune conditions such as systemic lupus erythematosus (MedlinePlus; StatPearls, NCBI). Notably, false positives caused by these conditions tend to cluster at low titers, frequently 1:8 or below, which can prompt unnecessary worry and even invasive follow up if the titer is read without context (StatPearls, NCBI). One controlled study even documented transient false positive RPR in patients with acute malaria (PMC, false positive RPR in malaria).
The practical message: a low titer reactive RPR with a negative confirmatory treponemal test usually points away from syphilis, not toward it. Many labs now run a reverse sequence algorithm, screening with an automated treponemal test first and using RPR to confirm and quantify, which can change how these mismatches are interpreted (PMC, RPR and the serologic diagnosis of syphilis). Either way, no single reactive RPR should ever be treated as a diagnosis on its own.

How RPR behaves across the stages of syphilis
Syphilis moves through distinct stages, and the RPR does not perform the same way at each one. Understanding this explains why a single test at the wrong moment can mislead.
- Primary syphilis is the stage of the initial sore, or chancre, usually appearing weeks after exposure. Because antibodies are still building, RPR sensitivity is only around 86 percent here, so a small but real share of early infections are missed. This is the window where a negative result is least trustworthy.
- Secondary syphilis is the stage of rash, mucous patches, and systemic symptoms. Antibody levels are at their peak, RPR sensitivity approaches 100 percent, and titers are typically high. This is the test’s sweet spot.
- Latent syphilis is the symptom-free stage that can follow. Reagin production can wane, so RPR sensitivity falls to roughly 73 percent, and titers often drift lower. A person can genuinely have syphilis here and show only a modest titer.
- Tertiary and neurosyphilis stages involve long-term damage to the heart, brain, and nerves. RPR may be reactive at varying levels, and a high titer, at or above 1:32, is associated with greater neurosyphilis risk, which can prompt examination of spinal fluid.
The lesson is that timing and stage are part of the result. The same test carries different weight depending on where in the disease course it is drawn.
The prozone phenomenon: when too much antibody hides the infection
This is the counterintuitive detail that even some clinicians overlook, and it matters most in exactly the people who can least afford a missed diagnosis. Normally more antibody means a stronger reaction. But occasionally there is so much reagin antibody in the blood that it overwhelms the test chemistry and prevents the clumping reaction from forming, producing a falsely nonreactive result. This is called the prozone phenomenon.
It is uncommon, reported in well under one percent of samples, but it clusters in secondary syphilis, in pregnancy, and in people with HIV co-infection, precisely the situations where syphilis is most dangerous and most transmissible. The fix is simple once it is suspected: the laboratory dilutes the serum and retests, and the true reactive result appears. So when the clinical picture strongly suggests active syphilis (a classic rash, for example) but the RPR comes back negative, an informed clinician can ask the lab to check for a prozone effect by running dilutions. It is a rare trap, but a consequential one, especially in pregnancy where the goal is to prevent congenital syphilis.
The two testing algorithms, and why your result may look backward
How your reactive or nonreactive result gets confirmed depends on which of two laboratory sequences your lab uses, and knowing this prevents confusion when the tests seem to disagree.
- The traditional algorithm screens first with the nontreponemal test (RPR), then confirms a reactive result with a specific treponemal test such as FTA-ABS or TP-PA. This is the classic order most people picture.
- The reverse sequence algorithm, now common because it can be automated, screens first with a treponemal test, then uses RPR to confirm and to provide the quantitative titer.
The reverse sequence sometimes produces a puzzling mismatch: a positive treponemal screen with a nonreactive RPR. This pattern often reflects previously treated syphilis, very early infection, or occasionally a false positive on the screen, and it is resolved with a second, different treponemal test. The practical point for a patient is that a confusing combination of results is usually the algorithm at work, not an error, and it is exactly the kind of thing a clinician sorts out rather than something to interpret alone.

Who should be screened, and how often
RPR is not just for people with symptoms. Because syphilis is often silent and has surged in recent years, screening is recommended for several groups regardless of how they feel.
- Pregnancy is the highest priority. Guidance calls for testing all pregnant people, and current obstetric recommendations advise screening three times during pregnancy, at the first prenatal visit, in the third trimester, and again at delivery, because untreated syphilis can cause devastating congenital infection that is entirely preventable with treatment.
- People with HIV, who are screened regularly given the frequent overlap of the two infections.
- People with new or multiple sexual partners, and men who have sex with men, who may be screened more often based on risk.
- Anyone diagnosed with another sexually transmitted infection, since co-infection is common.
- People with symptoms such as a painless genital sore or an unexplained rash on the palms and soles.
Because reagin antibodies take roughly three to six weeks to appear after exposure, a single negative test soon after a possible exposure may need to be repeated after the window has passed.
What happens after a confirmed diagnosis
If both the nontreponemal and treponemal tests are reactive and syphilis is diagnosed, the path forward is well established and, importantly, curable, especially when caught early. Treatment is centered on penicillin, with the specific regimen depending on the stage of disease. After treatment, the RPR titer is followed over time to confirm the therapy worked, since a successful response shows up as a falling titer, ideally a fourfold drop. A titer that fails to fall, or that rises fourfold, prompts a fuller evaluation for reinfection, treatment failure, or nervous system involvement. Diagnosis also triggers partner notification and testing, and screening for other sexually transmitted infections, because they so often travel together. None of this is something the RPR does alone; the number is the tool that tracks a process managed by a clinician.
How to prepare for the test and read your own result
The RPR draw is straightforward and does not require fasting or special preparation, which is part of why it scales so well across screening programs. The interpretation, though, benefits from a little context you can bring yourself.
- Know your timing. If you are testing because of a specific possible exposure, note how long ago it was. A test within the first few weeks may be too early, and a repeat after the antibody window may be advised.
- Bring your history. A prior treated syphilis infection, an autoimmune condition like lupus, a recent viral illness, pregnancy, or HIV status all shape how a result is read, especially a low-titer reactive one.
- Ask for the titer, not just reactive or nonreactive. Because the number carries the real information, and because change over time is what matters, having the actual titer recorded lets future tests be compared meaningfully.
- Expect a confirmatory step. A reactive screen is not a diagnosis. Anticipate a second, more specific test before any conclusion, and do not let a single reactive result drive fear before confirmation.
Common misunderstandings about RPR
- “A reactive RPR means I have syphilis.” Not by itself. It is a screen that must be confirmed with a treponemal test, and one to two percent of results are false positives, often at low titers.
- “A negative RPR always means I am clear.” Not necessarily. It can miss very early infection before antibodies rise, some late-stage cases, and rarely a prozone-effect case with very high antibody levels.
- “The RPR number is like a normal lab range.” No. The titer is a dilution ratio, not a concentration against a reference range, and its meaning comes mostly from how it changes over time.
- “Once treated, my RPR should be negative forever.” Not always. It may stay reactive at a low titer for a long time, a state called serofast, while the separate treponemal test typically stays positive for life.
- “A treponemal test can replace the RPR for monitoring.” It cannot. Treponemal antibodies persist for life and cannot tell you whether the infection is active or whether treatment is working, which is exactly what the RPR titer does.
Don’t just read about RPR, track it.
A single result is a snapshot. Superpower re-tests RPR and 100+ markers over time so you can watch them move as you change sleep, food, and training.
Frequently asked questions
Does a reactive RPR mean I definitely have syphilis?
No. A reactive RPR means reagin antibodies were detected, which raises the possibility of syphilis but is not a diagnosis. It must be confirmed with a specific treponemal test such as FTA-ABS, and false positives occur in about 1 to 2 percent of people tested (StatPearls, NCBI).
What is a normal RPR blood test result?
A normal RPR result is nonreactive, also called negative, meaning no reagin antibodies were found (MedlinePlus). Keep in mind that a negative result can miss very early infection, since antibodies usually take about 3 to 6 weeks after exposure to appear.
What does the RPR titer number mean?
The titer is the most diluted point at which your blood still tests reactive, such as 1:8 or 1:32, and it estimates how much antibody is present. Low titers are often less concerning and can reflect a false positive or a serofast state, while a titer of at least 1:32 is linked to higher neurosyphilis risk (StatPearls, NCBI).
Why is RPR repeated after treatment?
RPR is repeated to confirm treatment worked. The titer should fall, and a fourfold or greater rise signals possible reinfection or treatment failure that needs further evaluation (PMC, RPR and the serologic diagnosis of syphilis). Treponemal tests cannot do this because they usually stay positive for life.
What can cause a false positive RPR?
Conditions including HIV, hepatitis, Lyme disease, malaria, some pneumonias, intravenous drug use, and lupus can trigger a false positive, often at low titers (MedlinePlus; StatPearls, NCBI). This is why a reactive RPR always needs a confirmatory treponemal test before any diagnosis is made.
This article is for general educational purposes and is not medical advice. It cannot diagnose or treat you and does not replace your clinician. Always discuss your lab results and any health decisions with a qualified healthcare professional.
Related reading
Vital Signs Today may earn a commission if you buy through links on this page. It does not affect our editorial assessments.


